
Abstract
Abstract
Purpose
Glutaric acidemia type 1 (GA1), a rare hereditary metabolic disease caused by biallelic mutations of
Methods
We performed a retrospective chart review spanning 28 years identifying 114 GA1 patients, most from the Old Order Amish population of Lancaster County, Pennsylvania, who were homozygous for a pathogenic founder variant of
Results
Over an average follow-up of 4.7 ± 3.4 years, 24 (21%) of 114 patients had musculoskeletal problems requiring orthopaedic consultation. Scoliosis (n = 14), hip dislocation (n = 8/15 hips), hip subluxation (n = 2/three hips), and windswept hip deformity (n = 2) in the spine and hip joint were most common. In total, 35 orthopaedic surgeries were performed in 17 (71%) patients. The most common primary operations were one-stage procedures with proximal femoral varus derotation osteotomy and/or pelvic osteotomy (n = 8/14 hips) for subluxation or dislocation. In all, 11 patients had posterior spinal fusion for severe scoliosis. With the recommended metabolic management, there were no disease-specific complications in this cohort.
Conclusions
Children with GA1 who have static striatal lesions are at risk for musculoskeletal complications, especially scoliosis and hip dislocation, and appropriate operative management requires consultation with a metabolic specialist with specific considerations for fluid management and nutrition.
Level of Evidence
IV
Introduction
Glutaric acidemia type 1 (GA1; OMIM #231670) is a disorder of systemic and cerebral organic acid metabolism caused by biallelic variants of glutaryl-CoA dehydrogenase (
Neuronal
Outcomes for GA1 have improved considerably over the last two decades; with the combination of newborn screening for glutarylcarnitine (C5DC), adherence to a lysine-restricted/arginine-enriched prescription diet,19,20 and inpatient therapy during intercurrent illnesses,18,21 fewer than 10% of GA1 patients develop brain injury. 19 Those who remain neurologically healthy until their second birthday face an excellent long-term prognosis.22,23 Nevertheless, the risk for striatal degeneration remains high for patients born in resource-limited settings who do not have access to tandem mass spectrometry-based newborn screening or prescription medical foods.8,24
Regardless of their timing or mechanism, static striatal lesions result in a complex extrapyramidal movement disorder that is the principal determinant of clinical outcome.8,16–19,22 Severe, generalized dystonia is the most common motor pattern observed among neurologically injured GA1 patients, and entrains serious gastrointestinal, pulmonary and musculoskeletal complications that exact a heavy disease burden.22,25 The orthopaedic surgeon can play a critical role in alleviating this burden. Here, we review orthopaedic complications and their surgical management in a large cohort of GA1 patients treated at a single tertiary care centre.
Methods
Following institutional review board approval, we retrospectively collected data on 114 patients found within our institutional database who had a confirmed diagnosed of GA1. For subjects born between 1988 and 1994, the diagnosis was based on a characteristic clinical phenotype paired with detection of GA and 3HGA in urine by gas chromatography-mass spectroscopy. Detection of a pathognomonic metabolite (C5DC) using tandem mass spectrometry was incorporated into Pennsylvania newborn screening in 1994, and detection of the
Using our institution's inpatient and outpatient electronic medical records system, we extracted data about the method and age of diagnosis, current age, Gross Motor Function Classification System (GMFCS) score, medical comorbidities, gastrostomy tube status, seizure history, orthopaedic diagnoses, surgical interventions and postoperative follow-up. The large majority of physical examinations and operative decisions were conducted by a single senior pediatric orthopaedic surgeon (FM).
Indications for reconstructive surgery of a subluxed or dislocated hip included severe movement restriction, difficulty in perineal care, or pain with ambulation, transfers or sitting. The primary surgical technique was proximal femoral varus derotation osteotomy (VDRO) performed in a single stage. The reconstructive procedure combined routine varus shortening osteotomy with soft-tissue lengthening 26 and acetabular reconstruction with peri-ilial pelvic osteotomy 27 commonly used in children with cerebral palsy. No hip spicas were used. Physical therapy commenced on the first postoperative day and hip movement was allowed as much as the patient could tolerate. A smooth perioperative transition typically required aggressive management of both pain and the movement disorder using epidural blocks, oral and intravenous analgesics, and high doses of diazepam.
When structural scoliosis was evident on physical examination, patients were evaluated with sitting whole spine radiographs; spinal curvature ≥ 60 degrees was typically considered an indication for fusion. The strategy for posterior spinal fusion (PSF) followed rules of scoliosis secondary to cerebral palsy, meaning all curves were fused from T1 or T2 to the pelvis. These patients similarly needed careful postoperative monitoring to control pain and exacerbation of extrapyramidal movements while also mitigating any risk for metabolic instability.
Statistical analysis
Parametric and nonparametric analyses were performed. Descriptive and frequencies statistics were used to describe the population by mean and standard deviation. Statistical analysis was performed using SPSS v25 (IBM, Armonk, New York).
Results
Our retrospective review included a total of 114 children (50% female) diagnosed with GA1 during a 28-year period from 1988 to 2018 (Table 1). Mean age at follow-up was 11.9 ± 9.0 years (range six months to 40 years). In all, 24 (21%) GA1 patients had significant orthopaedic pathology on physical examination. The most common problems were severe scoliosis (n = 14) and abnormalities of the hip joint, including dislocation (n = eight patients/15 hips), subluxation (n = two patients/three hips), windswept deformity (n = 2), and dysplasia (n = 1) (Table 2). Although 48% of the patients in this cohort were GMFCS I (normal motor function) and 22% had milder motor problems (GMFCS II or III), primarily patients with severe impairments (GMFCS IV-V) developed significant orthopaedic deformities requiring surgical treatment (Table 1).
Demographic characteristics of overall cohort of patients with glutaric aciduria type 1 (GA1)
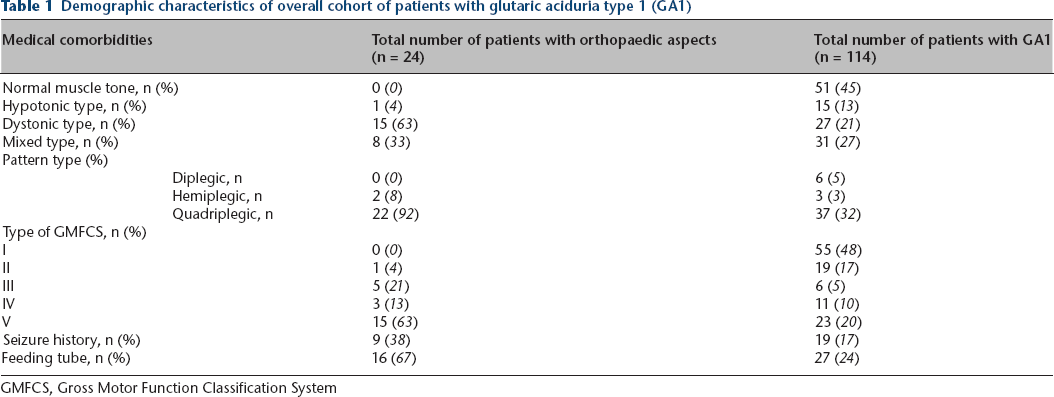
GMFCS, Gross Motor Function Classification System
Case list of patients with significant musculoskeletal pathology
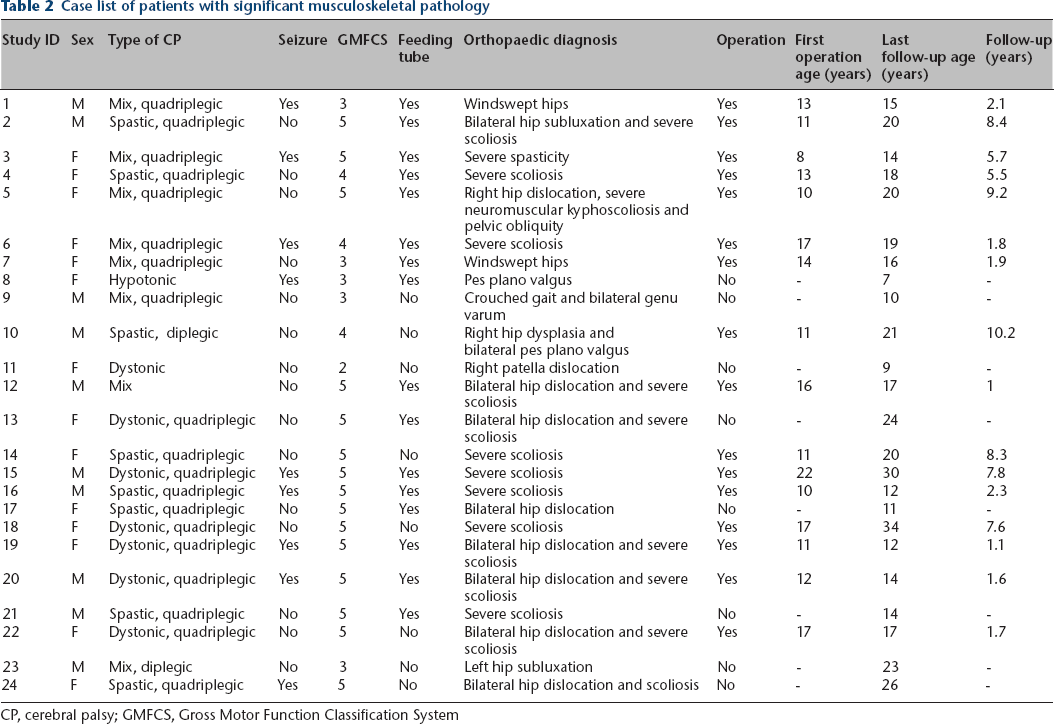
CP, cerebral palsy; GMFCS, Gross Motor Function Classification System
A total of 35 surgeries were performed in 17 (71%) of 24 patients with musculoskeletal pathology. The mean age at first operation was 13.8 ± 4.8 (range six months to 25 years) and mean postoperative follow-up was 4.7 ± 3.4 years (range six months to 10 years). Nine (38%) individuals required multiple procedures (two surgeries (n = 3) three surgeries (n = 4), five surgeries (n = 2)) and the mean interval between the first and second operation was 3.4 ± 1.4 years (range nine months to five years). The most common primary surgical procedures were PSF for severe scoliosis (n = 11) and one-stage VDRO and/or pelvic osteotomy for subluxation or dislocation of the hip (n = eight patients/14 hips) (Table 3). Three patients experienced significant postoperative complications: blade plate prominence caused skin irritation requiring removal in three hips of two patients and one individual (patient 5, Table 3) underwent revision VDRO due to recurrent hip dislocation.
List of orthopaedic procedures performed
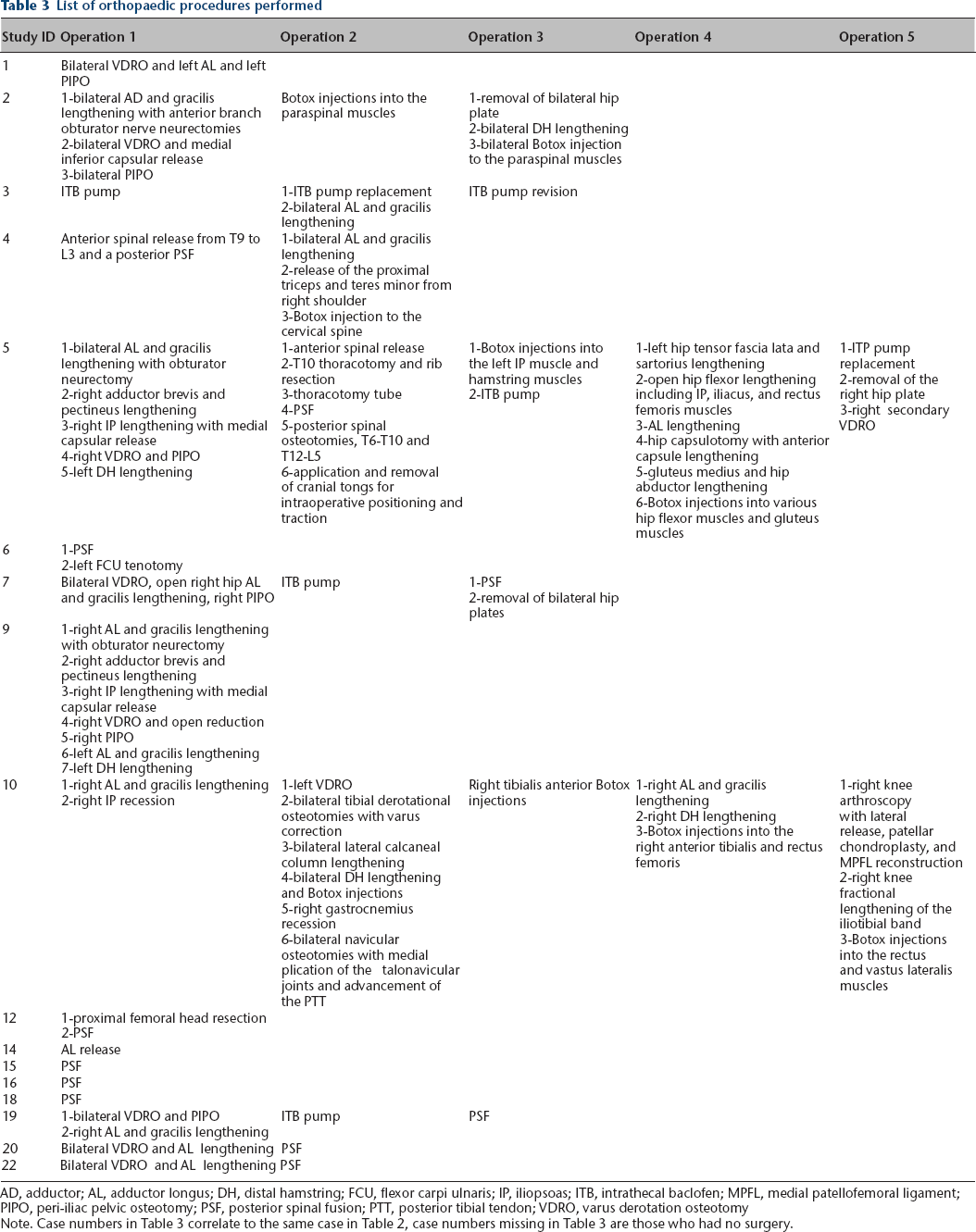
AD, adductor; AL, adductor longus; DH, distal hamstring; FCU, flexor carpi ulnaris; IP, iliopsoas; ITB, intrathecal baclofen; MPFL, medial patellofemoral ligament; PIPO, peri-iliac pelvic osteotomy; PSF, posterior spinal fusion; PTT, posterior tibial tendon; VDRO, varus derotation osteotomy
Note. Case numbers in Table 3 correlate to the same case in Table 2, case numbers missing in Table 3 are those who had no surgery.
An intrathecal baclofen (ITB) pump was implanted in four patients to palliate severe, medically intractable dystonia. The catheter tip was positioned at the low cervical-high thoracic spinal cord level and average ITB usage time was 4.1 years (range seven months to ten years). The ITB pump was replaced three times in two patients, twice due to expired battery life and once due to dysfunction. (Table 3). Four patients had one or more botulinum toxin injections in paraspinal (n = 2) or lower extremity (n = 2) muscles for transient relief of focal dystonia.
Discussion
When the diagnosis of GA1 is made after an acute encephalopathic crisis, irreversible degeneration of striatal neurons leaves patients with a dystonic movement disorder irrespective of
We found a relatively high incidence of neurological injury among individuals in our cohort (Table 1), most of whom were
Because GA1 manifests clinically as a static rather than progressive encephalopathy, the orthopaedic approach is similar to that for cerebral palsy, but with a critical distinction: surgical planning in patients with GA1 should include a detailed anticipatory strategy to support intermediary metabolism during fasting and surgical stress. 45 We recommend that elective procedures be planned in consultation with a metabolic specialist, who can cooperate with an anesthesiologist to develop a perioperative treatment protocol that safeguards against metabolic complications45–48 (Table 4).
Management guidelines for elective surgery with glutaric acidemia type 1
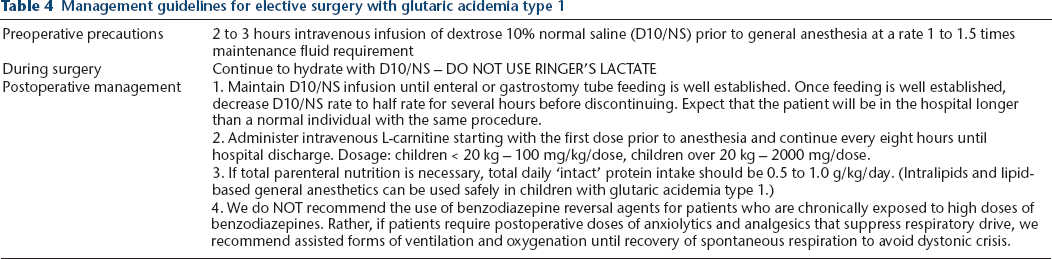
For any patient with severe dystonia, medical providers should also recognize risks for pulmonary aspiration, post-extubation laryngeal dystonia and adverse reactions to paralytic agents. 48 During the postoperative period, effective analgesia is especially important to prevent a self-reinforcing cycle of pain, anxiety and worsening dystonia that can escalate to life-threatening status dystonicus.25,39 High intravenous doses of analgesic and anxiolytic medications are typically required to control such ‘dystonic storms’. Recognizing the risk for this and other serious complications, we prefer to correct all musculoskeletal deformities in a single surgical session.
The literature includes reports of botulinum toxin injection and ITB for treatment of the dystonia associated with GA1.31,49 In four patients with focal or generalized dystonia, Burlina and colleagues found that botulinum toxin was particularly beneficial for the upper extremities but had minimal impact on craniocervical dystonia. 49 Kyllerman et al 31 used ITB to successfully treat two patients with severe dystonia, and found that botulinum toxin injection of the cervical paraspinal and lower extremity muscles controlled focal dystonia following PSF. In four patients from our cohort, ITB provided relatively effective palliation for intractable dystonia but required close follow-up for pump refills and management of mechanical problems.
In conclusion, severe dystonia and its attendant musculoskeletal complications are common among GA1 patients who develop static stiatal lesions during the first few years of life. Encephalopathic crisis strikes fewer than 10% of affected children in the modern era of newborn screening and appropriate prospective care,8,9 but this outcome still remains tragically high in resource-limited settings.24,37 Among neurologically injured patients with GA1, scoliosis and hip dislocation are the predominant indications for orthopaedic intervention, and all elective surgeries should be executed with a perioperative strategy to minimize metabolic stress (Table 4) and a postoperative plan to control the cycle of pain and anxiety that can culminate in life-threatening status dystonicus.25,39
Footnotes
KAS: Acquisition, analysis or interpretation of data for the work; Revising it critically for important intellectual content; Final approval of the version to be published; Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
GFO: Substantial contributions to the conception or design of the work; Drafting of the work; Final approval of the version to be published; Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
FM: Substantial contributions to the conception or design of the work; Acquisition, analysis or interpretation of data for the work; Drafting of the work; Revising it critically for important intellectual content; Final approval of the version to be published; Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved