
Abstract
Abstract
Purpose
Subtalar arthroereisis has been described for the treatment of flexible juvenile flatfoot. However, the mechanism responsible for deformity correction has not yet been investigated adequately. The aim of this study was to document the effect of subtalar arthroereisis on the tarsometatarsal bone morphology.
Methods
We retrospectively reviewed the clinical and radiological data of 26 patients (45 feet) with juvenile flexible flatfoot deformity treated by subtalar arthroereisis at our department between 2000 and 2018. Radiological evaluation included angular measurements of tarsometatarsal bone morphology as well as hindfoot and midfoot alignment. Mean radiographic follow-up was 19.4 months (sd 8.8; 12 to 41).
Results
A significant change of angular measurements of tarsometatarsal bone morphology was found after subtalar arthroereisis (p < 0.001). While there was an increase of the distal medial cuneiform angle (DMCA) and the medial cuneo-first metatarsal angle on the anteroposterior view, a decrease of the naviculo-medial cuneiform angle and the medial cuneo-first metatarsal angle was seen on the lateral view. Furthermore, we found significant improvements of all hindfoot and midfoot alignment parameters except the lateral tibio-calcaneal angle and the calcaneal pitch angle (p < 0.001).
Conclusion
Our data support the theory of tarsometatarsal bone remodelling, which may contribute to the effect of subtalar arthroereisis for the treatment of flexible juvenile flatfoot.
Level of evidence
IV
Introduction
Although paediatric flatfoot deformity is one of the most frequent skeletal disorders in children,1,2 no general accepted consensus exists regarding the indication, timing and type of treatment. Most flatfeet have a tendency to correct spontaneously without any treatment. Nevertheless, several different nonoperative and operative methods for symptomatic flatfoot in children have been established so far. 3 While initial conservative management with stretching programs of the Achilles tendon and the longitudinal-arch-building muscles is frequently recommended, conflicting evidence exists on the effects of paediatric foot inlays and orthoses.4–7 In case of failure of conservative measures (defined by persistent pain and flatfoot deformity), numerous surgical procedures for flatfoot correction in children have been proposed, including subtalar arthroereisis,8–11 calcaneus osteotomies,12–15 subtalar arthrodesis16,17 and tendon lengthening and transfers.3,18 Arthroereisis procedures placing different bone blocks8,19 or absorbable or non-absorbable synthetic implants9,10,20 in the sinus tarsi were introduced in the 19th century. At our institution, we routinely perform a minimal-invasive extraarticular arthroereisis of the subtalar joint using a cancellous screw – the so-called ‘calcaneo-stop technique’ introduced by Recaredo Alvarez in Spain in 197011,21 – for the treatment of non-neurogenic and neurogenic symptomatic flexible flatfeet in children since 2000.
The effect of the arthroereisis procedure is presumed to be not only mechanical by restricting excessive subtalar joint eversion, 3 but also proprioceptive by influencing dynamic joint ankle stability via stimulation of the sinus tarsi mechanoreceptors and nociceptors.21–23 Furthermore, long-term effects of subtalar arthroereisis are supposed to be caused largely by tarsometatarsal bone remodelling.
Thus far, significant improvements in the radiological alignment of the hindfoot and midfoot (e.g. Costa-Bartini angle, calcaneal pitch, talocalcaneal angle, talonavicular coverage, talo-first metatarsal angle) have already been described after subtalar arthroereisis.9–11,21,24 However, the effect of subtalar arthroereisis on bone remodelling of the tarsal bones has not been investigated so far. Therefore, the aim of this study was to document the effect of subtalar arthroereisis on the tarsometatarsal bone morphology. We hypothesized that the tarsometatarsal bone morphology would be changed after subtalar arthroereisis.
Materials and methods
This study was approved by our institutional review board (ethics committee approval number: 1239/2018). We retrospectively reviewed all patients with juvenile non-neurogenic or neurogenic flexible flatfoot deformity treated by subtalar arthroereisis between 2000 and 2018 at the University Hospital for Orthopaedics of Innsbruck, Austria. The patients were identified from our surgical database. The inclusion criterion was: diagnosis of a symptomatic juvenile non-neurogenic or neurogenic flexible flatfoot deformity in children that had failed conservative treatment. Failure of conservative treatment was defined by persistent pain and flatfoot deformity. Exclusion criteria were as follows: incomplete radiological data (preoperative and postoperative radiographs missing or inadequate radiographic projections), radiological follow-up of < 12 months, previous surgery of the affected foot and non-neurogenic or neurogenic flatfoot associated with any other pathology (e.g. adult flatfoot, post-traumatic flatfoot, talo-calcaneal coalitio, congenital vertical talus).
We identified 67 patients (117 feet) with flexible flatfoot treated by subtalar arthroereisis from our surgical database. A total of 41 patients (72 feet) were excluded due to incomplete/insufficient radiological data (n = 54), a follow-up of < 12 months (n = 13) or early revision surgery within 12 months after index surgery (n = 5). Thus, data of 26 patients (45 feet) was available for final radiological and statistical analysis (Fig. 1).
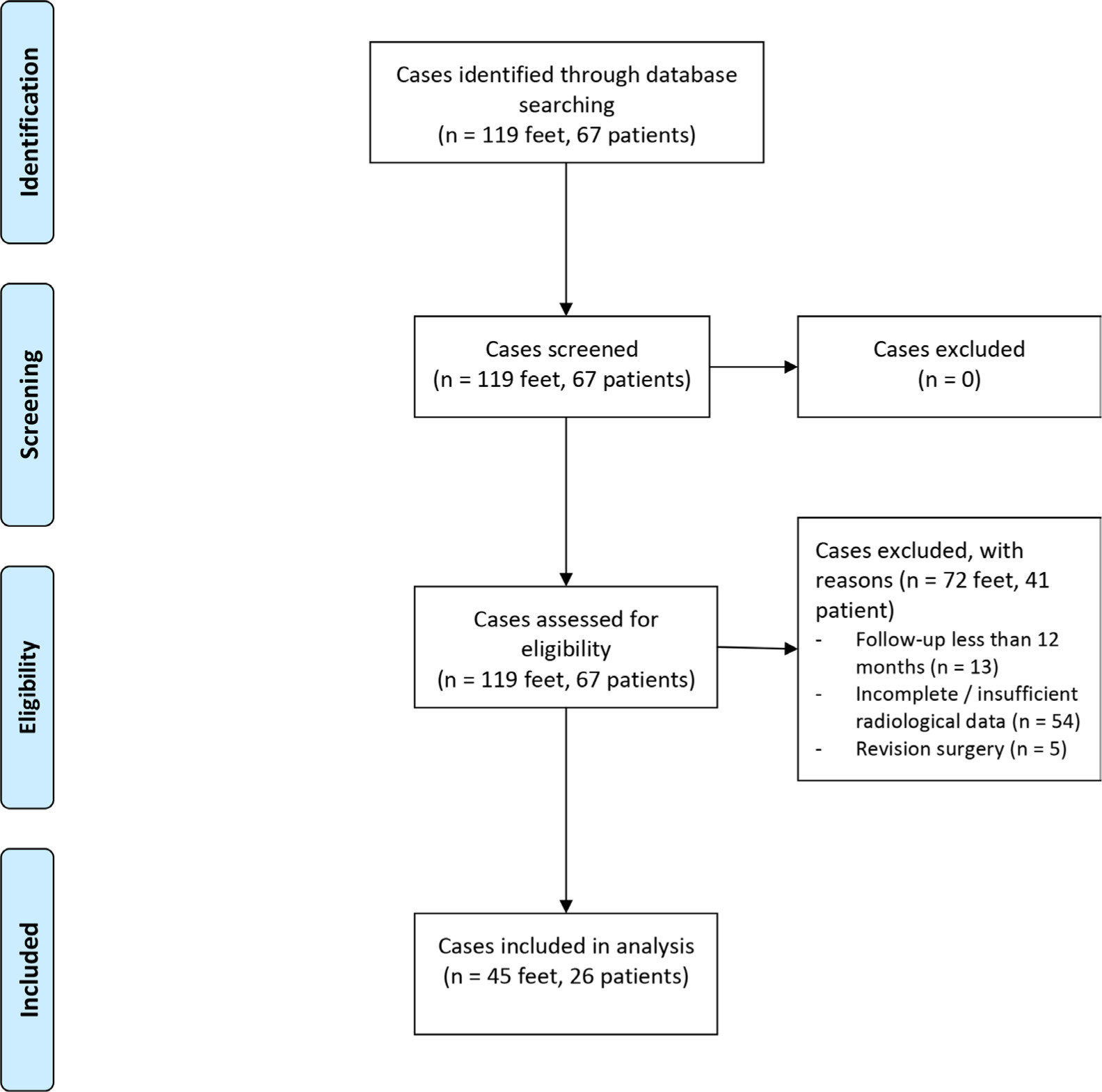
Flow diagram.
Mean age at operation was 10.3 years (sd 2.8; 4 to 13). Subtalar arthroereisis was usually indicated between the age of eight to 13 years. However, surgery was performed at an earlier age in six patients (ten feet) due to progressive neurogenic flatfoot (five patients, eight feet; mean age at operation: five years (4 to 7)) or due to the express wish of the parents (one patient, two feet; age at operation: seven years). Subtalar arthroereisis was performed in 20 right/25 left and in 27 male/18 female feet. Mean radiographic follow-up was 19.4 months (sd 8.8; 12 to 41).
Operative technique
All operations were carried out by supervised trainees or consultant orthopaedic surgeons specializing in foot and ankle surgery. A small lateral skin incision was carried out over the sinus tarsi and blunt subcutaneous dissection was performed to expose the sinus tarsi. After manual varization and supination of the hindfoot, a cranio-caudal and slightly dorso-ventral directed Kirschner (K)-wire was inserted into the calcaneus just below the lateral process of the talus. After verifying the correct position using image intensification the K-wire was over-drilled and a 6.5-mm cannulated cancellous bone screw was inserted into the calcaneus. Following final clinical and radiological evaluation of the correction achieved and range of movement the skin was closed in layers and a sterile dressing was applied. Full weight-bearing as tolerated was allowed immediately after the operation and the patients were discharged the first day after surgery after obtaining a weight-bearing radiograph control. Implant removal was recommended routinely after the expected end of bony remodelling at the final clinical examination. Screws were removed routinely in 18 patients (31 feet, 69%) at the age of 14 years (sd 1.4; 12 to 17) at a mean of 33 months (sd 9.3; 12 to 41) after index surgery. In three patients (five feet) implant removal was carried out earlier due to prominent hardware at the age of five, seven and ten years after 19, 23 and 24 months, respectively.
Radiographic examinations
All available pre- and postoperative (first and last postoperative) weight-bearing or simulated weight-bearing anteroposterior and lateral foot radiographs were retrospectively examined by the same investigator at two different points in time. The last postoperative radiographs were taken earlier to screw removal with the screw still in situ in all cases. Standard radiographic techniques following our institutional guidelines were used to obtain reproducible and accurate films for radiological evaluation. Only radiographs with an adequate lateral view of the foot and ankle (defined as a radiograph with the medial and lateral talar domes superimposed on one another) were included for evaluation. The intra- and interobserver reliabilities and the age-related changes for the most commonly used radiological parameters of flatfoot have already been studied in the literature.25–27 One independent orthopaedic resident (MR) supervised by a fellowship-trained foot and ankle surgeon (DD) examined each radiograph.
Radiological evaluation included the following measurements of tarsometatarsal bone morphology as well as hindfoot and midfoot alignment parameters (Figs 2 and 3). Tarsometatarsal bone morphology parameters measured were the distal medial cuneiform angle (DMCA) and medial cuneo-first metatarsal angle (ap CM1) on the anteroposterior view and the medial arch sag angle (MASA), naviculo-medial cuneiform angle (NMCA) and medial cuneo-first metatarsal angle (lat CM1) on the lateral view. The DMCA was formed by the distal joint orientation line of the first talo-metatarsal joint and a line perpendicular to the mechanical axis of the medial cuneiform on the anteroposterior view. 28 The ap CM1 was created by the intersection of the line drawn through the longitudinal axis of the medial cuneiform and through the longitudinal axis of the first metatarsal on the anteroposterior view. 29 The MASA was measured as the angle between the proximal articular surface of the navicular and the proximal articular surface of the first metatarsal on the lateral view. The MASA is negative when the proximal articular surface of the first metatarsal is plantarflexed compared with the proximal articular surface of the navicular. 30 The NMCA was formed by the angle between a line parallel to the naviculo-medial cuneiform joint and a line horizontal to the floor on the lateral view. 30 The lat CM1 was defined by the angle between a line parallel to the medial cuneiform-first metatarsal joint and a line horizontal to the floor on the lateral view. 30
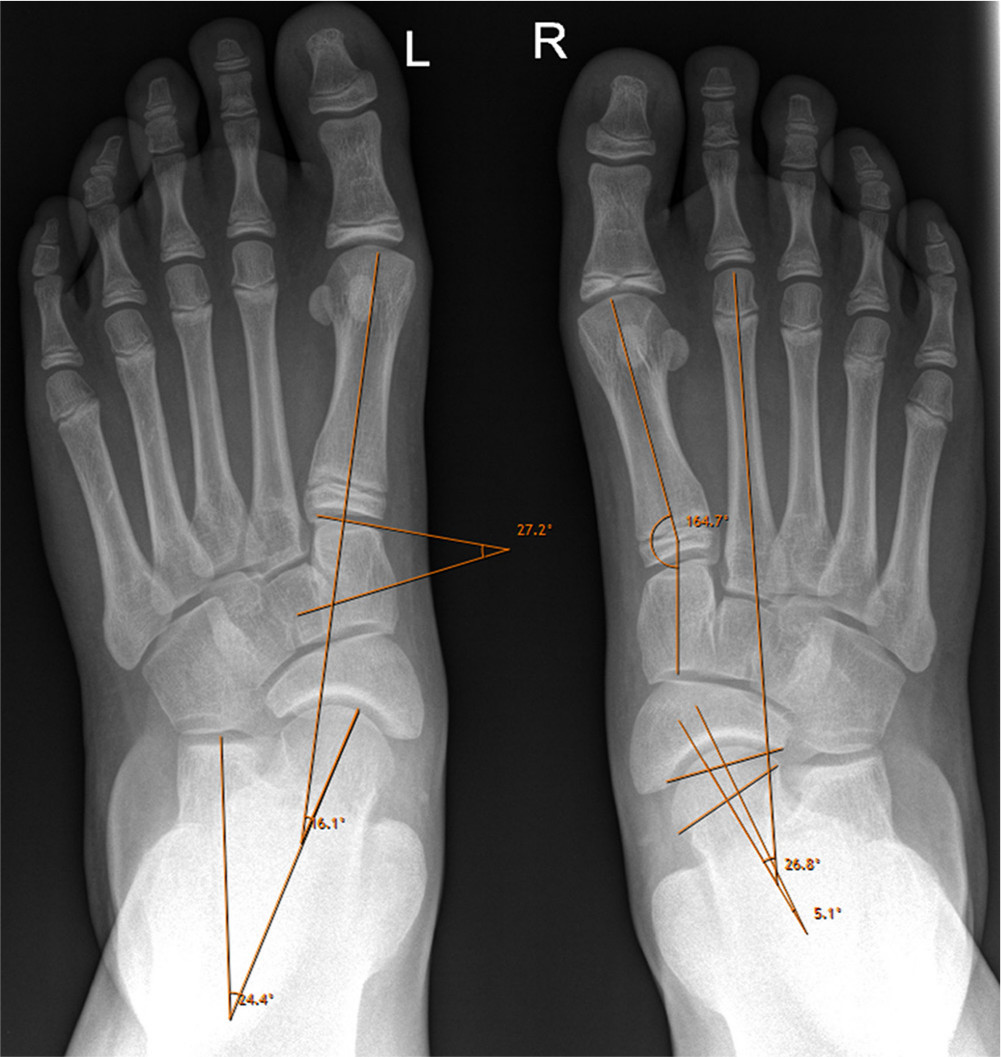
Anteroposterior radiological measurements: measurement of the distal medial cuneiform angle, talometatarsal I angle and talocalcaneal angle (left foot) and the medial cuneo-first metatarsal angle, talometatarsal II angle and talonavicular (coverage) angle (right foot). Further explanations for the determination of each angle are given in the material and methods section.
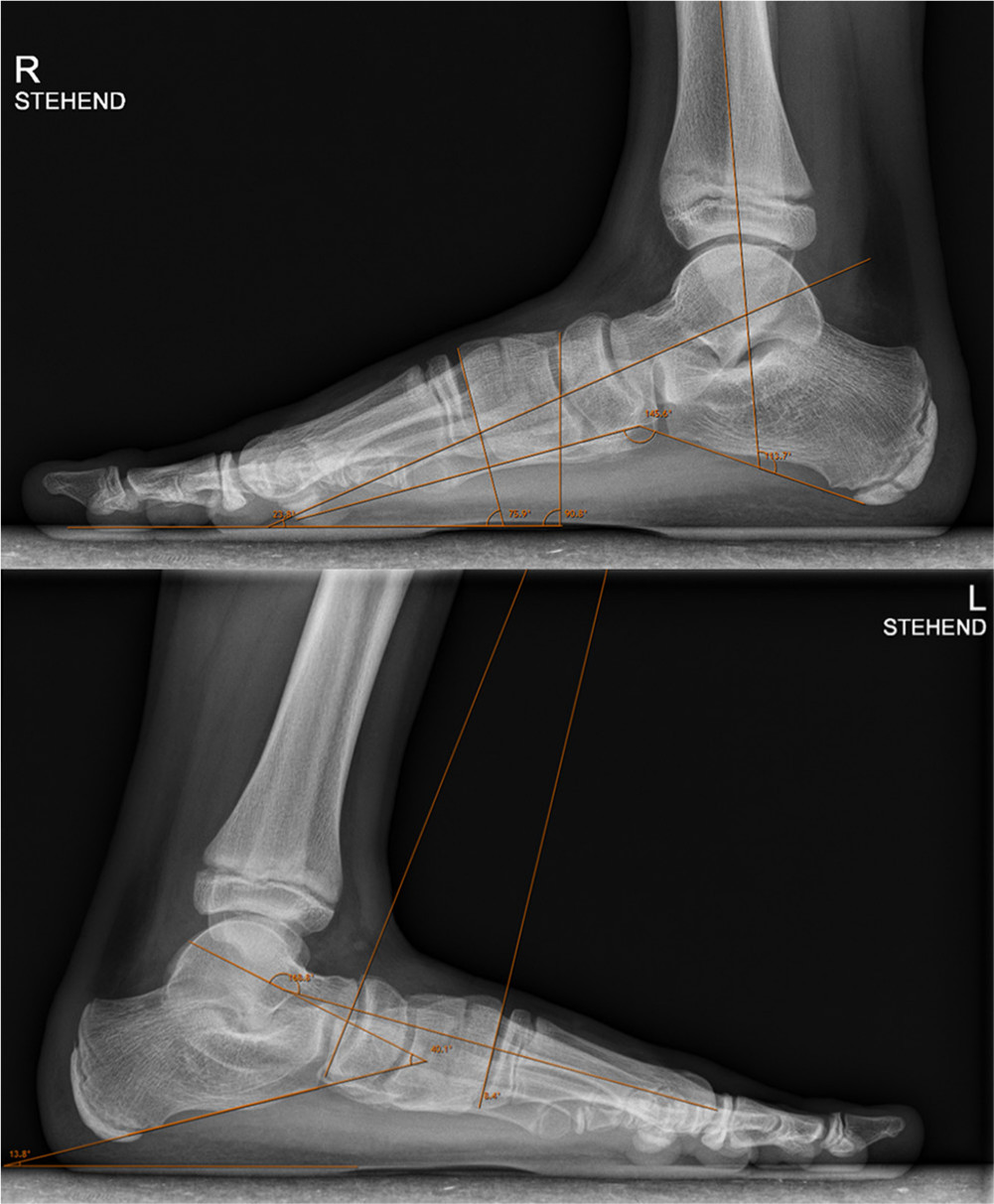
Lateral radiological measurements: measurement of the talar inclination angle, medial cuneo-first metatarsal angle, naviculo-medial cuneiform angle and Costa-Bartani angle (right foot) and the calcaneal pitch angle, talocalcaneal angle, talometatarsal I angle and medial arch sag angle (left foot). Further explanations for the determination of each angle are given in the material and methods section.
Hindfoot and midfoot alignment parameters included the talocalcaneal angle (Kite's angle), talonavicular (coverage) angle (talonavicular joint congruency), talometatarsal I angle and talometatarsal II angle on the anteroposterior view and the talocalcaneal angle, tibiocalcaneal angle, talometatarsal I angle (Meary's angle), calcaneal pitch angle (calcaneal incidence), Costa-Bartani angle and talar inclination angle (talohorizontal angle, talar declination) on the lateral view. The anteroposterior talocalcaneal angle (Kite's angle) was formed by the intersection of the line drawn through the longitudinal axis of the talus and through the longitudinal axis of the calcaneus. An increased angle indicates valgus of the hindfoot.27,31 The talo-navicular coverage angle (talo-navicular angle, talo-navicular joint congruency) was defined as the angle between a line bisecting the anterior articular surface of the talus and another line bisecting the proximal articular surface of the navicular.26,32 The anteroposterior talo-first metatarsal angle was formed by the intersection of the line drawn through the longitudinal axis of the talus and through the longitudinal axis of the first metatarsal. 26 The talo-second metatarsal angle was measured using the anteroposterior radiograph and was defined as the angle formed by a line through the midpoint of the talus from anterior to posterior with a line bisecting the second metatarsal. 33 The lateral talo-calcaneal angle was defined by the intersection of a line through the longitudinal axis of the talus and a line along the plantar surface of the calcaneus. 27 It is increased with valgus deformities of the hindfoot. The tibio-calcaneal angle was defined as the intersection between the anatomical axis of the tibia and plantar surface of the calcaneus. 27 The lateral talo-first metatarsal angle (Meary's angle) was created by the intersection of the talar and the first metatarsal longitudinal axes. The values are increasingly positive for flatfoot deformities. 34 The calcaneal pitch angle (calcaneal incidence) was defined as the angle between a line drawn along the edge of the plantar soft-tissue shadow and a line drawn along the lower margin of the calcaneus. 35 The Costa-Bartani angle was formed by a line from the lower point of the medial sesamoid to the lower point of the talonavicular joint and a line from the lower point of the talonavicular joint to the lower point of the posterior calcaneal tuberosity. 21 The talohorizontal angle (talar inclination angle, talar declination) was formed by the intersection of the lateral longitudinal axis of the talus and a line horizontal to the floor.27,36
Statistical methods
Data was managed and processed by the data manager (MB) using Excel software (Microsoft, Redmond, Washington). Data was validated by the programmed range, validity and consistency checks. Additionally, there was a manual/visual check for medical plausibility. Statistical analysis was performed using SPSS Statistics 22 (IBM Analytics, Armonk, New York). Data was expressed as means with sd and range, unless indicated otherwise. The primary dependent variables were analyzed using a multivariate analysis (analysis of variance) with a Greenhouse-Geisser correction. A p-value < 0.05 was considered significant.
Results
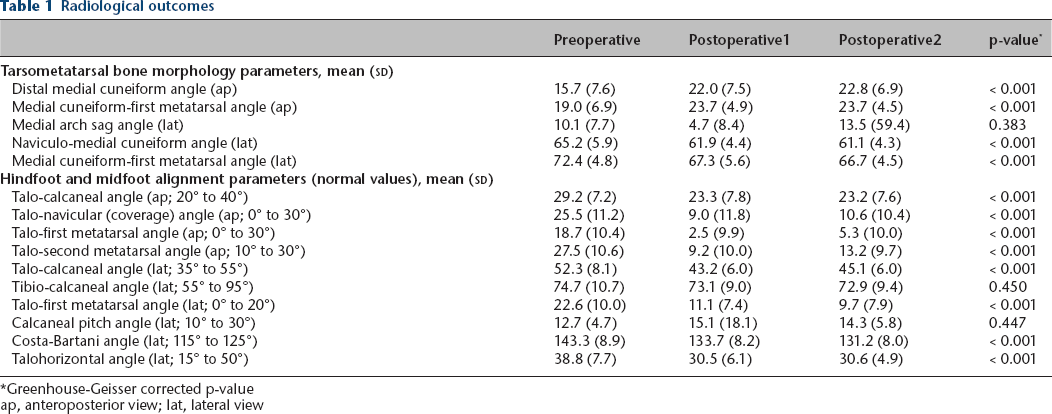
Radiological outcomes are presented in the Table 1. A significant change of tarsometatarsal bone morphology was found after subtalar arthroereisis (p < 0.001). While there was an increase of the DMCA and the ap CM1, a decrease of the NMCA and the lat CM1 was seen on the lateral view. The MASA decreased by 5.4° from preoperatively to the first postoperative radiograph control, but increased again by 8.8° in the postoperative course. Furthermore, we found significant improvement of all hindfoot and midfoot alignment parameters except in the lateral tibio-calcaneal angle and the calcaneal pitch angle (p < 0.001). Table 2 summarizes the values of each angle reported in the literature and serves as a historical control group to our results.
Radiological outcomes
Greenhouse-Geisser corrected p-value
ap, anteroposterior view; lat, lateral view
Values of radiological measurements reported in the literature
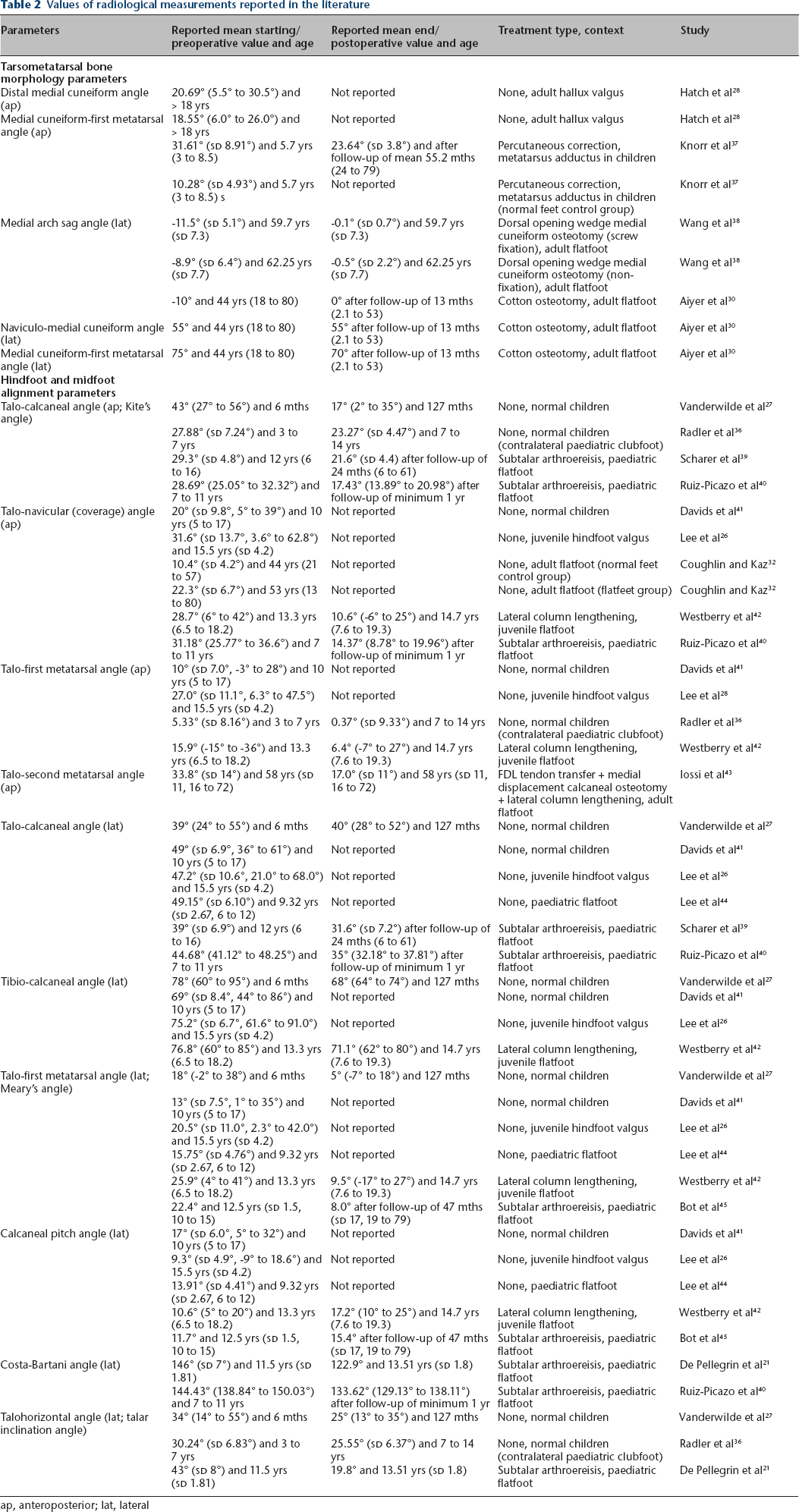
ap, anteroposterior; lat, lateral
Discussion
Flexible flatfoot in children and adolescents is a common orthopaedic condition, which often remains asymptomatic and thus requires no treatment.1–4 In case of severe and symptomatic flatfoot with pain that interferes with normal activities and failure of nonsurgical management, flatfoot surgery is recommended to relieve symptoms and to restore a medial longitudinal arch of the foot.3,4 Among other surgical procedures, subtalar arthroereisis – either by means of placing different bone blocks8,19 or absorbable/non-absorbable synthetic implants9,10,20 into the sinus tarsi or by subtalar extra-articular screw arthroereisis11,21 – can be performed to limit excessive pronation of the tarsus at the level of the subtalar joint, hereby restoring the height of the medial arch of the foot through a combination of static, dynamic and proprioceptive mechanisms.21,24 Although arthroereisis represents a minimally invasive procedure to correct a flexible flatfoot in children offering the advantages of technical simplicity and rapid recovery, opinions remain polarized in respect of safety and effectiveness.3,24 While the exact mechanisms of action by which arthroereisis improves foot alignment remain to be elucidated, several clinical and radiological studies have demonstrated good outcomes following subtalar arthroereisis. Specifically, improvements of radiological hindfoot and midfoot alignment in terms of the talo-calcaneal angle, the Costa-Bartani angle, the talar inclination angle and the calcaneal pitch angle have been observed.9–11,21,24 In this study, we investigated tarsometatarsal bone remodelling and radiological alignment of the hindfoot and midfoot after the calcaneo-stop procedure. Our results showed a significant change of tarsometatarsal bone morphology in terms of the DMCA, the CM1, the MASA, the NMCA and the lat CM1. Furthermore, we found significant improvement of all hindfoot and midfoot alignment parameters except of the lateral tibio-calcaneal angle and the calcaneal pitch angle.
The improvement of hind- and midfoot alignment found in our study is well in line with the existing literature. In their critical review of the literature on subtalar joint arthroereisis, Metcalfe et al 24 summarized radiological outcomes after subtalar arthroereisis. They found a mean improvement of 13° (compared with the 12.1° found in our study), 20.9° (14.9°), 6.8° (6.0°), 2.2° (1.6°), 16° (13.4°) and 14.5° (8.2°) for the Costa-Bartani angle, the talonavicular coverage angle, the lateral talocalcaneal angle, the calcaneal pitch angle, the lateral talometatarsal I angle and the talohorizontal angle, respectively. The limited improvement of the calcaneal pitch angle observed in our study thereby might be explained by the site of correction at the level of the subtalar joint and has been observed by other authors as well.21,24 However, the comparison of the radiological outcomes reported between the studies is hampered by substantial variation in the radiological parameters reported and missing definitions of measurement procedures for the reported values. 24
The morphology of a flatfoot deformity can be described clinically using external visual parameters (flattening of the medial foot arch, rearfoot valgus and forefoot arch) or radiographically by measuring the shape and length of bones and their position relative to one another. This is usually done by measuring conventional radiographs in which the foot as a 3D structure is transformed into a 2D representation. However, this transformation is prone to great variability through positioning, posture and variability of the projection. In this study, we tried to measure the impact of subtalar arthroereisis on the morphology of the foot by determining angular measurements between the tarsal bones on conventional radiographs. The advantages of the use of conventional radiographs are their widespread routine use in the evaluation of flatfoot deformity, their relatively low cost, their high availability and the possibility to obtain a standardized imaging of the weight-loaded foot. However, the observed changes of the angular measurements may partially be explained by differences in radiological projections, dynamic (e.g. dorsiflexion of the first toe) factors and age-related changes of the tarsometatarsal bones. Ultimately, it may only be possible to draw definitive conclusions about the changes in tarsal bone morphology using a 3D method (such as CT or MRI).
Strengths and limitations
The validity of our data may be limited and our findings must be interpreted with caution for the following reasons.
Our study is limited by its retrospective nature and a comparably high drop-out rate of 61% of cases. This drop-out rate is largely attributable to the strict radiographic quality criteria applied because only radiographs with an adequate lateral view of the foot and ankle (defined as a radiograph with the medial and lateral talar domes superimposed on one another) were included for evaluation. However, the authors believe that systematic bias due to the comparably high drop-out rate is unlikely.
Repeatability of radiological measurements is subject to technical error.46–49 In young children and non-ambulating patients especially, standardization to provide reproducible radiographs often proves to be difficult. Furthermore, radiographic measurements are known to be subject to significant intra- and interobserver error. 42 Intra- and interobserver variability has not been investigated for all angles reported in our study.
Measurements of the 3D foot on 2D images produces potential errors when comparing radiographs with cadaver models. However, advanced radiological imaging (CT and MRI) is neither medically indicated nor economically and ethically justifiable for flexible flatfoot deformity in children. The use of angular measurements instead of bone length measurements in this study may only partially allow one to draw indirect conclusions on bony tarsal remodelling. Furthermore, the angular measurements reported in this study can be affected by static (e.g. bone morphology) and dynamic (e.g. dorsiflexion of the first toe) factors. However, standard radiographic techniques following our institutional guidelines were used to obtain weight-bearing or simulated weight-bearing anteroposterior and lateral foot radiographs, thereby minimizing the influence of dynamic factors on our measurements.
Skeletal development has an impact on radiographic measurements as well. Age-dependent alterations of the measured angles have not been reported universally. 27 Consequently, the differentiation between natural resolution of a flatfoot deformity with age and that owed to the intervention must be considered. Therefore, another limitation to our study was the lack of a control group of children with flexible flatfoot with surgical indication who had not undergone surgery. However, the changes of tarsometatarsal bone morphology found in our study exceeded the expected age-related development of the foot form.
Finally, clinical outcomes are not reported in this study. Although radiological measures have been applied as markers of success after flatfoot surgery, the correlation of radiological alignment and patient-reported outcome after paediatric flatfoot has not been investigated so far.
Conclusion
With regard to our findings we conclude that changes of tarsometatarsal bone morphology as well as changes of subtalar hind- and midfoot alignment contribute to the effect of subtalar arthroereisis for the treatment of flexible juvenile flatfoot.
Footnotes
MR: Radiological measurements.
DD: Radiological measurements, Supervision.
PH-P: Study design, Data processing, Statistical analysis.
JW: Data processing, Manuscript preparation.
RB: Study design, Manuscript preparation, Supervision.