
Abstract
Introduction
Monteggia-like lesions are rare injuries in adults that include a wide spectrum of complex fracture-dislocations of the proximal ulna and radius. In this retrospective study, we performed a modified Boyd approach and a standard surgical protocol for the treatment of these lesions. Our aim was to evaluate the results of the operative treatment for patients with Monteggia-like lesions, using a modified Boyd approach.
Materials and Methods
We present a retrospective study of 14 patients who underwent surgical treatment for Monteggia-like lesions. Preoperative clinical and radiological evaluation was performed. In 5 cases radial head prosthesis was placed, and in 3 cases the radial fracture was stabilized with the use of interfragmental screws. Regarding the proximal ulnar fracture, ORIF-anatomical plate and ORIF-straight plate was used in 12 and 2 cases, respectively.
Results
Average clinical follow up was 16.9 months. Postoperatively, the mean Mayo Elbow Performance score was 83.4 points (range 70-100) and the mean visual analog scale was 1.7 (range 0-14). Mean flexion and loss of extension were 122.1° (range 80°-140°) and 21.4° (range 5°-40°), respectively. Mean supination of the forearm was 66.8° (range 50°-80°) and the mean pronation was 67.5° (range 60°-75°). Heterotopic ossification was observed in 3 patients (21.4%) and 1 patient developed stiffness (7.1%). The patient who developed stiffness underwent reoperation for plate removal and arthrolysis, with satisfactory results.
Conclusions
The surgical treatment of Monteggia-like lesions in adults remains a challenge. In the present study, the use of a standard surgical protocol, with a modified Boyd approach, successfully restores the movement and stability of the elbow, with a low complication rate.
Keywords
Introduction
The term “Monteggia fracture” includes a wide spectrum of complex fracture-dislocations of the proximal ulna and radius. It was first introduced in 1814 by Giovanni Battista Monteggia as a fracture to the proximal third of the ulna with associated anterior dislocation of the radial head, only based on the mechanism of injury and on the physical examination.1,2 However, this fracture pattern only describes 60% of this type of injuries. In 1958, Jose Luis Bado created another classification system with 4 basic types, based on the direction of the radial head dislocation and the associated fractures. 3 In 1991, Jupiter et al 4 further classified the type II injuries of Bado classification (type II—fracture of the proximal or middle third of the ulna with posterior dislocation of the radial head) in 4 subtypes (types IIA, IIB, IIC, and IID), according to the type of fracture of the radial head and the location of the ulnar fracture. Due to the complexity of this type of injuries and the wide variety of fracture patterns, the term Monteggia-like lesions or Monteggia-equivalent injuries was introduced, in order to describe Monteggia lesions which include additional injuries, such as radial head fractures and coronoid fractures.5–7 Monteggia-like lesions are rare injuries, as they account for only 2% to 5% of the forearm injuries. 8 There are also other classification systems that are useful in terms of management and prognosis. Regan and Morrey classified the coronoid fractures 9 and radial head fractures were also classified according to Mason's system. 10 A variety of surgical approaches have been developed and performed to treat lesions of the elbow. Most of them allow treatment of less than 3 different simultaneous lesions of the elbow, so the majority cannot be used to treat Monteggia-like lesions, where lesions are 3 or more at the same time. Most commonly used approaches for those lesions are the extensile posterior approach (global approach), the posteromedial Taylor-Scham approach, the posterolateral Kocher approach and posterolateral Boyd approach. 11 The Boyd approach provides a safe exposure of the proximal third of the ulna and the radial head and neck, avoiding injury to the posterior interosseous nerve (PIN).11,12 The aim of this retrospective study is to evaluate the results of the operative treatment of patients with Monteggia-like lesions with the use of a modified Boyd approach. This approach includes releasing of the anconeus muscle, the lateral ulnar collateral ligament (LUCL), partial releasing of the annular ligament and the joint capsule, without an osteotomy. The closure includes repairing of those structures with the use of anchors.
Materials and Methods
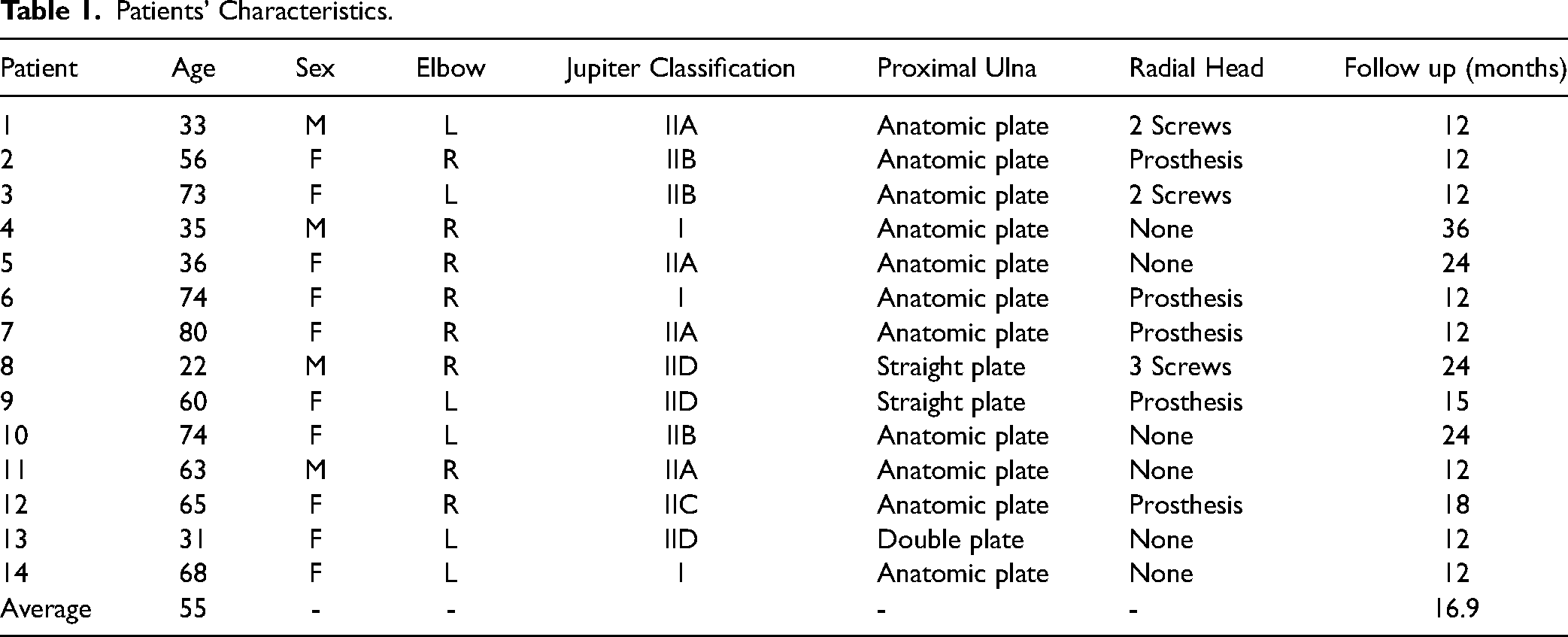
Between March 2010 and January 2021, 14 patients underwent surgical treatment for Monteggia-like lesions in our orthopaedic department. Inclusion criteria were age over 18 years and clinical and radiological follow up for over 6 months. All patients had preoperative radiographs and computed tomography (CT) scans to allow classification and planning. None of the patients had other pre-existing disorders and previous open fractures to the elbow and they all gave written informed consent. All patients included were treated with a modified Boyd approach. A total of 14 patients were included, 4 of them were male (28.6%) and 10 were female (71.4%). The mean age of the study population was 55 years (22-80 years). In 6 patients the left elbow was injured and in 8 patients the right elbow was injured. After reviewing the postoperative radiographs and CT scans, all lesions were classified according to the Jupiter classification. There were 3 type I fractures (21.4%), 4 type IIA fractures (28.6%), 3 type IIB fractures (21.4%), 1 type IIC fracture (7.1%), and 3 type IID fractures (21.4%) (Table 1).
Patients’ Characteristics.
Surgical Technique
The clinical and radiographic evaluation led to the diagnosis of Monteggia-like lesions (Figures 1a-b and 2a-d). Surgical management was selected, and operations were performed by the same senior surgeon (ZTK) from the department of shoulder and elbow surgery. The procedure was performed under general anesthesia. The patients were placed in lateral decubitus position on the nonaffected side (on the left side if the fracture was at the right elbow), with the arm supported in a leg holder. Care was taken to place the noninjured arm that was in hyperabduction, away from the injured elbow, in order to have enough space for the surgeons and the C-arm (Figure 1c). The procedure was performed under tourniquet control. In one patient with a very thick arm the procedure was performed without tourniquet control. The surgical landmarks were the lateral epicondyle, the olecranon, and the radial head. A long posterior incision was made, that was curved laterally over the olecranon (Figures 1d and 2e). Regarding deep exposure, the fascia covering anconeus and extensor carpi ulnaris was incised for the length of the skin incision. The anconeus, the LUCL and the joint capsule were identified, elevated from their insertions, and released directly as a single unit. The radial head was exposed first and was dislocated posteriorly with the forearm in full flexion to access the injury (Figure 1e). In 3 cases, interfragmental screws were placed for the reconstruction of the radial head, without releasing the annular ligament (Figure 1f-g). Additionally, in 5 cases, the fracture of the radial head was unreconstructable and was treated with radial head prosthesis (Figure 2h-i). For this purpose, releasing of the annular ligament was performed. The 3 structures released from the supinator crest (the capsule, LUCL, and annular ligament) were reconstructed with anchors to the proximal ulna, to prevent subluxation. Postoperatively, posterior plaster splints extending above the elbow were used for 2 weeks, with the elbow in 90° of flexion and neutral rotation. A sling was used at all times and regular active finger flexion and extension was encouraged. After 2 weeks the plaster was removed and a sling was maintained for 6 more weeks.

Anteroposterior (a) and lateral (b) radiographs of the left elbow of a 33-year-old male who presented in our emergancy department with severe pain after an injury, showing the existence of a Monteggia-like lesion. The fracture of the proximal third of the ulna involves the distal olecranon (Bado Type II, Jupiter IID). Additionally, the radiographs show fracture of the radial head (Mason type I). Intra-operatively, the patient was placed in lateral decubitus position on the nonaffected side (right side), with the arm supported in a leg holder. Regarding the noninjured arm (right), it was in hyperabduction, away from the injured elbow in order to have enough space for the surgeons and to facilitate the use of the C-arm (c). A long posterior incision was made that was curved laterally over the olecranon and extended distally, in order to expose the fractures (d). The fracture of the radial head was not displaced (e). Postoperative anteroposterior (f) and lateral (g) radiographs showing stabilization of the radial head fracture with 2 screws and open reduction and internal fixation of the ulnar fracture with the use of an anatomic plate.

Anteroposterior (a) and lateral (b) radiographs of the left elbow of a 60-year-old female who presented in our emergency department with severe pain after an injury, showing a Monteggia-like lesion. The patient underwent computed tomography scan that shows fracture of the proximal third of the ulnar diaphysis (Bado type II, Jupiter IIB) (c) and a fracture of the radial head (Mason type III) (d). A long posterior incision was made that was curved laterally over the olecranon and extended distally, in order to expose the fractures (e). Regarding deep exposure, the fascia covering anconeus and extensor carpi ulnaris was incised at the length of the skin incision (f). The radial head was replaced with a prosthesis (g). Postoperatively anteroposterior (h) and lateral (i) radiographs showing replacement of the radial head with prosthesis and open reduction and internal fixation of the ulnar fracture with the use of a straight plate. After 6 months of follow up the patient has a range of motion of 15° loss of extension (j), 130° flexion (k), 60° supination (l), and 70° of pronation (m).
Clinical Evaluation
The functional outcome was assessed for all patients by the same senior surgeon who had performed the operations. For the assessment the Mayo Elbow Performance Score (MEPS) was used in order to evaluate the elbow function, and the visual analog scale (0-10) (VAS) was used to measure pain during activity. Furthermore, the range of motion in all movements (elbow flexion and extension, forearm supination and pronation) was also measured using a standard full-circle goniometer, at the follow-up visits.
Radiographic Evaluation
All patients had anteroposterior and lateral radiographs and CT scan of the elbow preoperatively. Postoperatively, anteroposterior and lateral radiographs were performed immediately postoperatively and at the follow-up visits. The postoperative radiographs were reviewed for degenerative changes, heterotopic ossification, fracture union, and signs of loosening in the cases where radial prosthesis was used.
Results
All 14 patients were available for clinical and radiological follow-up visits at a mean of 16.9 months (range 12-36 months) postoperatively (Table 1). All fractures were united. Concerning the clinical results, we used 2 main scoring systems to evaluate the possible postoperative limitations of the operated elbows and to measure subjectively the pain that patients experienced. For this purpose, we used the MEPS or Mayo Elbow Performance Index (MEPI) and the VAS, respectively.13,14 The mean MEPS in this series was 83.4 points and the patients reported a mean VAS value of 1.7 at their last follow-up visit. We also evaluated the postoperative elbow's range of motion (Figure 2j-m). The mean flexion and loss of extension was 122.1° and 21.4°, respectively. The mean supination of the forearm was 66.8° and the mean pronation was 67.5° (Table 2). During the assessment of the postoperative radiographs no periprosthetic lucencies were observed. Furthermore, no abnormal radiographic findings were observed regarding the radiocapitellar line in the 5 cases where the unreconstructable fractures of the radial head were treated with a radial head replacement. This line was assessed to evaluate the alignment of the radial head prosthesis. Regarding the complications, heterotopic ossification (HO) around the elbow was observed in 3 patients (21.4%). None of these patients was subjected to reoperation. One patient developed stiffness (7.1%) and underwent surgical operation to remove the anatomic plate from the ulna and perform arthrolysis, with satisfactory results.
Postoperative Results of Scoring Systems and Mean Range of Motion.
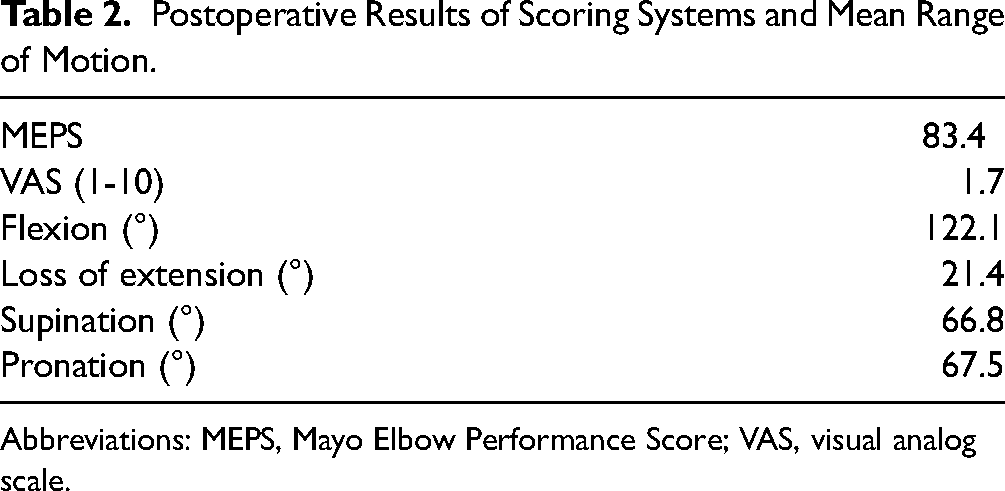
Abbreviations: MEPS, Mayo Elbow Performance Score; VAS, visual analog scale.
Discussion
Monteggia-like lesions are rare and their surgical treatment in adults remains a challenge for orthopedic surgeons. Correct clinical and radiological identification, as well as classification, followed by appropriate surgical treatment that addresses all components of the injury, can lead to good or even excellent postoperative results. 15 Access to the proximal ulnar and radial head for fracture fixation or prosthetic replacement of the radial head is usually gained through a lateral approach (Kocher, Kaplan, and extensor digitorum communis [EDC]-splitting approach) or a posterior approach. The Boyd approach is a posterior approach which requires incision and repair of the annular ligament. It was first described in 1940 and it allows access to all 3 joints (ulnohumeral, radiocapitellar, and proximal radioulnar) that may need to be visualized in order to treat Monteggia-like lesions. It allows treatment with a single-incision approach, as both radial head osteosynthesis and arthroplasty, as well as reconstruction of the ulnar fracture are easily performed using the same approach. However, the incision of the annular ligament and LUCL may lead to iatrogenic posterior instability of the elbow joint. 12
A modification of the Boyd approach, called Wrightington approach, has as major advantage that it leaves the related with posterior subluxation, annular ligament, and LUCL, intact. This approach was recently described and performed in 2 series of human cadavers.16,17 This modification provides excellent exposure to the radial head, the proximal ulna and the capitellum, as the anconeus muscle is dissected from the ulna and because of the osteotomy of the supinator tuberosity. The attached annular ligament to the tuberosity is moved as a single unit, offering excellent visualization without the complications associated with the incision of the annular ligament and the LUCL.16,17 By removing this mechanical block, the radial head is easily subluxated and so, its replacement is a much easier procedure for the surgeon. Moreover, the risk of damage to the capitellum through forced reduction of the radial head prosthesis is minimized thanks to sufficient exposure. Nerve injury, most commonly of the PIN, during lateral and posterolateral approaches to the radial head and proximal radius is always a concern due to the anatomical position of the nerve. The Kocher, Kaplan, and EDC-splitting approaches are more lateral and anterior than the Boyd and its variants and so they place the PIN at greater risk of injury. On the other side, in Wrightington approach does not place the PIN at risk of injury. Even though this approach offers excellent visualization of the proximal structures of the elbow to the surgeons and the decreased risk of nerve injury, there are also doubts concerning its use. Specifically, the osteotomy of the supinator crest may involve the risk of causing iatrogenic trauma. Performing an osteotomy may increase the risk of formation of HO. Another potential complication is nonunion of the osteotomized supinator crest causing posterior instability of the elbow.
There is another variation of the Boyd approach, which includes releasing of the lateral capsuloligamentous structures from the supinator crest without osteotomy. The biggest publication using this Boyd's variant performed by Robinson et al 18 was a series of 21 patients. By using this approach, surgeons release the annular ligament, the LUCL and the joint capsule with sharp dissection, and avoid osteotomy of the supinator crest. The exposure of the radial head and neck is excellent and at the same time complications associated with an osteotomy are eliminated. Besides, in this approach the PIN is protected by the elevated supinator muscle. The closure includes repairing of the capsuloligamentous structures with transosseous sutures. The number of studies regarding Monteggia-like lesions treated with this surgical technique is limited.
Our approach, a modified Boyd approach, provides excellent exposure of the radial head by releasing the anconeus muscle, the LUCL and the joint capsule. Another major advantage of this extension is that it leaves the related with posterior subluxation, annular ligament partially intact. The posterior interosseous nerve which runs deep to the supinator muscle is protected. As it is already described in the literature, after the use of the Boyd approach or its modifications, one of the most common complications is the formation of HO, that is usually associated with concomitant fractures of the olecranon or proximal ulna. 18 Although this is not well documented due to the limited number of patients in these studies, we also had 3 cases of HO in our group of patients. These 3 cases were classified as types IIA, IIB, and IID according to the Jupiter classification, and all of them included the distal part of the ulna. In all of them the ulnar fracture was stabilized with plates and in only 1 case the radial head was replaced. None of these patients needed further surgical treatment.
The main difference between our approach and the modification performed by Robinson et al, is that during closure instead of creating bone tunnels to stabilize the lateral capsuloligamentous structures with transosseous repair, we use anchors. Even though the anchors are more expensive than the transosseous sutures, this technique is faster and less traumatic because drilling through the entire diameter of the bone is avoided.
Conclusion
The current retrospective study aimed to evaluate the results of Monteggia-like lesion in adults who were treated with this modified Boyd approach. Surgical treatment with this surgical protocol successfully restored the movement and stability of the elbow, with a low complication rate in our series of 14 patients with Monteggia-like lesions. With a follow up of a mean period of 16.9 months, a total of 5 patients (35.7%) had unreconstructable fractures of the radial head, and as a result we replaced the radial head with prosthetic heads. We strongly believe that this modified Boyd exposure, which is characterized by using anchors to repair the lateral ligament complex, offers great access to the radial head and enables a sufficient restoration of the stability of the elbow. In addition, this technique is not only safe and reproducible, but it is also associated with a low complication rate. It can be a useful tool for every surgeon responsible for the treatment of Monteggia-like lesions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.