
Abstract
Abstract
Purpose
Slipped upper femoral epiphysis (SUFE) is one of the most common adolescent hip pathologies in children with potential for life-long morbidity secondary to avascular necrosis (AVN). The primary aim is to determine an up-to-date demographic of SUFE, as well as current trends in presentation and radiological characteristics. Secondary aims are to quantify prophylactic fixation and subsequent contralateral SUFE.
Methods
Between 01 January 2013 and 31 December 2015, all cases of SUFE were identified in Northern Ireland. Patient demographics, slip characteristics and outcomes are presented and the incidence rates were calculated using census data. Temporal changes in incidence, compared with a previous cohort, are demonstrated.
Results
A total of 56 patients (80 hips) were identified. Based on census data, SUFE incidence has declined from 7.14 to 4.69/100,000 population aged < 16 years. Male cases predominated by > 2:1 ratio, and tended to be older than female cases. Approximately 75% of patients were above the 75th centile for age-sex adjusted body weight. Knee pain as a presenting symptom led to a delay in diagnosis. Prophylactic fixation was performed in 25.9%, with contralateral slips occurring in 27.5%. AVN occurred in 7.4% and remained static.
Conclusion
The incidence of SUFE has declined ∼34% in our region. When SUFE occurs, knee pain often results in a delay in definitive diagnosis, and commands clinical vigilance to avoid delays in diagnosis. Patients in our region should be aware of a 1-in-4 contralateral slip rate. Overall, AVN rates remain static and are acceptable, despite the declining incidence of SUFE.
Level of evidence
Level III - Retrospective Cohort Study
Introduction
Slipped upper femoral epiphysis (SUFE) is one of the most common adolescent hip disorders affecting the peripubertal child. 1 However, incidence rates vary between studies and by geographical location.1–9 The exact pathophysiological mechanism is widely reported and multifactorial.1–9
SUFE can be complicated by the development of avascular necrosis (AVN) of the femoral head, with associated functional disability and increased morbidity. As such, the appreciation, prompt recognition and diagnosis of this condition is paramount in reducing the long-term morbidity. Anecdotally, the senior authors (JB and AC) of this study felt there was a reduction in frequency of SUFE procedures being performed regionally, and those that were being treated appeared to be presenting much longer from onset of symptoms. We, therefore, decided to review the practice regionally within Northern Ireland, which has a small number of paediatric orthopaedic units, a low rate of population migration and a regional radiology and theatre management system with which to identify this population cohort.
The current study primarily aims to determine the current demographics of SUFE in Northern Ireland, as well as the clinical and radiological characteristics of SUFE.
Secondary aims are to report our AVN, prophylactic fixation and contralateral slip rates.
Materials and methods
A retrospective review of all SUFE patients in a three-year period between 01 January 2013 and 31 December 2015, inclusive, was performed. Patients were identified using a regional picture archiving and communication system (PACS) with specific search criteria (age < 16 years; intraoperative fluoroscopy of hip, pelvis or femur; performed at paediatric surgery capable sites). These results were independently reviewed to exclude any non-SUFE cases. Cross referencing of case was performed through interrogation of electronic theatre management systems to identify all patients receiving any procedure involving ‘cannulated’ screw fixation. These were again reviewed to remove any incorrect theatre coding, and then cross referenced against the PACS results to ensure all patients were captured.
Study approval was provided by the Audit and Research Department, Belfast Health and Social Care Trust (BHSCT Ref 5084).
All patients had a minimum of 24 months clinical and radiological follow-up.
Patient weight was recorded for all paediatric patients as routine, however, not every patient has height data available and as such body mass indices could not be calculated for all patients. Therefore, classifying patients by weight centiles, using United Kingdom age- and sex-adjusted weight centile plots for children, was performed.
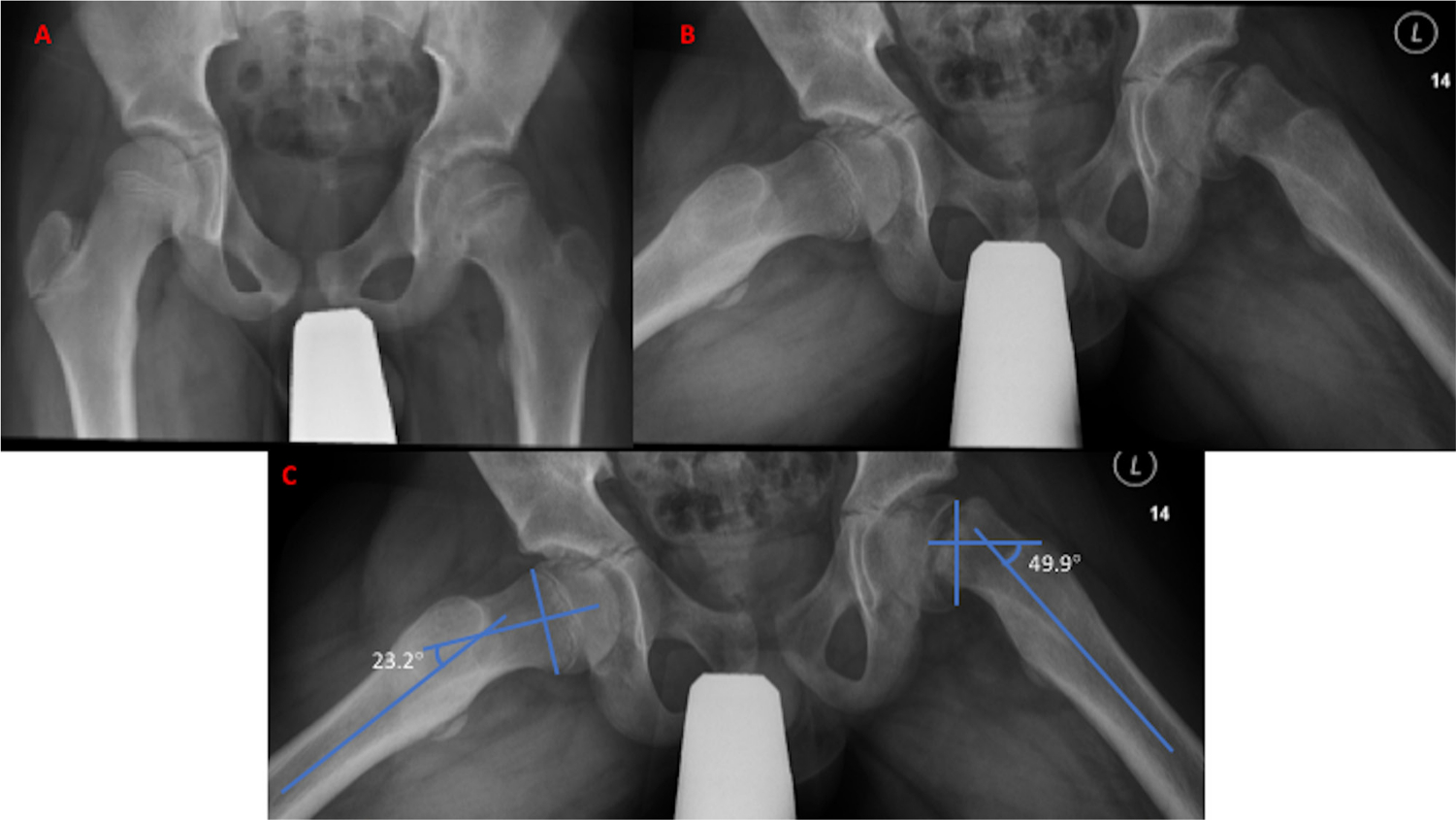
SUFE classifications were documented using the temporal classification of acute (less than three weeks), chronic (more than three weeks) and acute-on-chronic (more than three weeks with an acute exacerbation of symptoms). The Loder stability was also documented from the clinical notes. Southwick angles were measured for each patient using the method described by Aronsson and Carlson. 10 The angle of slip is thus the angle on the normal side subtracted from that in the affected hip, on the Lauenstein frog leg lateral view (Fig. 3). The SUFE can then be graded as mild (grade I; < 30°), moderate (grade II; 30° to 50°) or severe (grade III; > 50°).
Surgical technique
Surgical technique was by way of a lateral percutaneous approach under general anaesthetic in the supine position. Surgery was performed either freely draping on a standard radiolucent operating table or by placing the foot in a boot on a fracture traction table. Choice of technique was at the discretion of the operating surgeon. Guidewire placement was by way of a fluoroscopically guided freehand wire.
At the time of surgery, if serendipitous reduction occurred, the hip was fixed with in situ fixation.
In the case of grade I SUFE, these were pinned in situ. For all acute grade II, i.e. within 24 hours of onset, a gentle attempted reduction by positioning was performed. Otherwise, it was pinned in situ. Acute grade III SUFE was managed as per grade II, except failure to improve with closed reduction by positioning to an acceptable position prompted a modified Dunn open reduction and pinning. Chronic grade II and III SUFE were pinned in situ if possible. If deemed not possible, elective open reduction and internal fixation was performed.
In all cases, a 6.0 mm to 7.0mm cannulated stainless steel screw was used after successful fluoroscopically-guided placement of guidewire. Screw placement was intended to be perpendicular to the physis, aiming for the centre of the epiphysis.
Contralateral prophylactic pin fixation was performed at the discretion of the operating consultant. Variables in determining this included younger age at onset/skeletally immature (i.e. open triradiate cartilage), significantly overweight patient, any history of similar pain in the opposite hip with normal radiographic findings and the presence of known risk factors for SUFE. Also taken into consideration was the parents’ ability to reliably appreciate contralateral symptoms and report early. If this was deemed limited, then prophylactic fixation was considered.
Postoperatively, patients were partial weight bearing for four weeks minimum. All were followed up long term until the capital epiphysis had closed.
Census data was obtained from the open data repository at the Northern Ireland Statistics and Research Agency, 11 which allowed calculation of the incidence.
Analysis
Trends are reported, with sex-specific breakdown provided. For continuous data, mean values with sd, and ranges are given, unless otherwise stated. Appropriate statistical analyses for parametric and non-parametric data were performed and a p-value < 0.05 was considered statistically significant. SPSS for Mac v22 (IBM, Armonk, New York) was used to perform all analyses and comparisons.
Results
Demographics
We identified 56 patients, comprising 83 hips undergoing surgery. All were Caucasian individuals. There were two primary bilateral SUFE, 54 unilateral, of whom 14 had prophylactic pinning of the contralateral side and 11 patients demonstrated subsequent contralateral slips.
We previously quoted the incidence of SUFE within the same population base between 1997 and 1999. Data from the Northern Ireland Statistics and Research Agency census data, which is freely available online, allowed calculation of the incidence during the years of interest. The average incidence at that time was 7.14/100 000 (95% confidence interval (CI) 7.096 to 7.184) population aged 16 years or under, 9 compared with 4.69/100 000 (95% CI 4.662 to 4.718) population aged 16 years or under between 2013 and 2015. This indicates a decline in incidence of 34% in a comparative population cohort 15 years later.
There was a 2.5:1 male preponderance. Mean age overall was 12 years (8 to 16; median 12 years; modal age 14 years). Mean age by gender for girls was 11.6 years, and for boys was 12.2 years. Left-sided slips were more common than right (34 versus 20). Mean body weight was 57.78 kg (sd11.9). Centiles were plotted according to United Kingdom age-matched paediatric growth charts, and 43/56 (76.8%) of patients plotted above the 75th centile for age- and sex-matched weight (Figs 1 and 2) and 25/56 (44.6%) were > 95th centile.
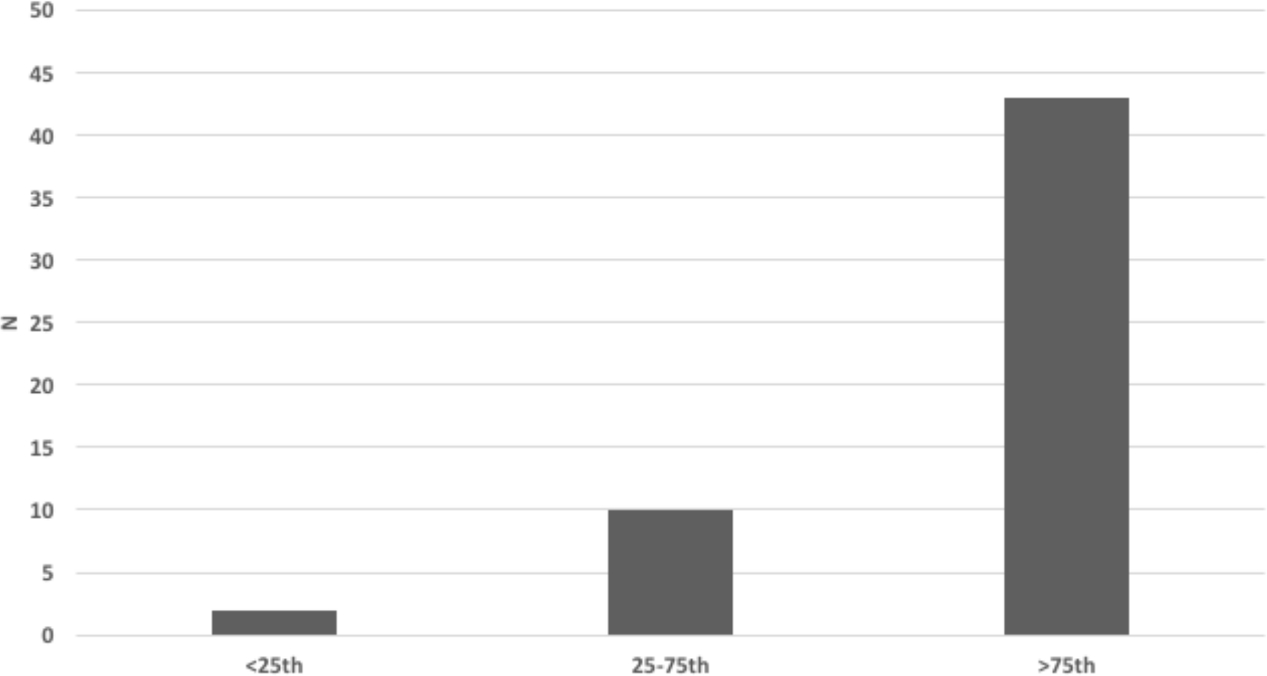
Proportion of patients according to weight centiles.
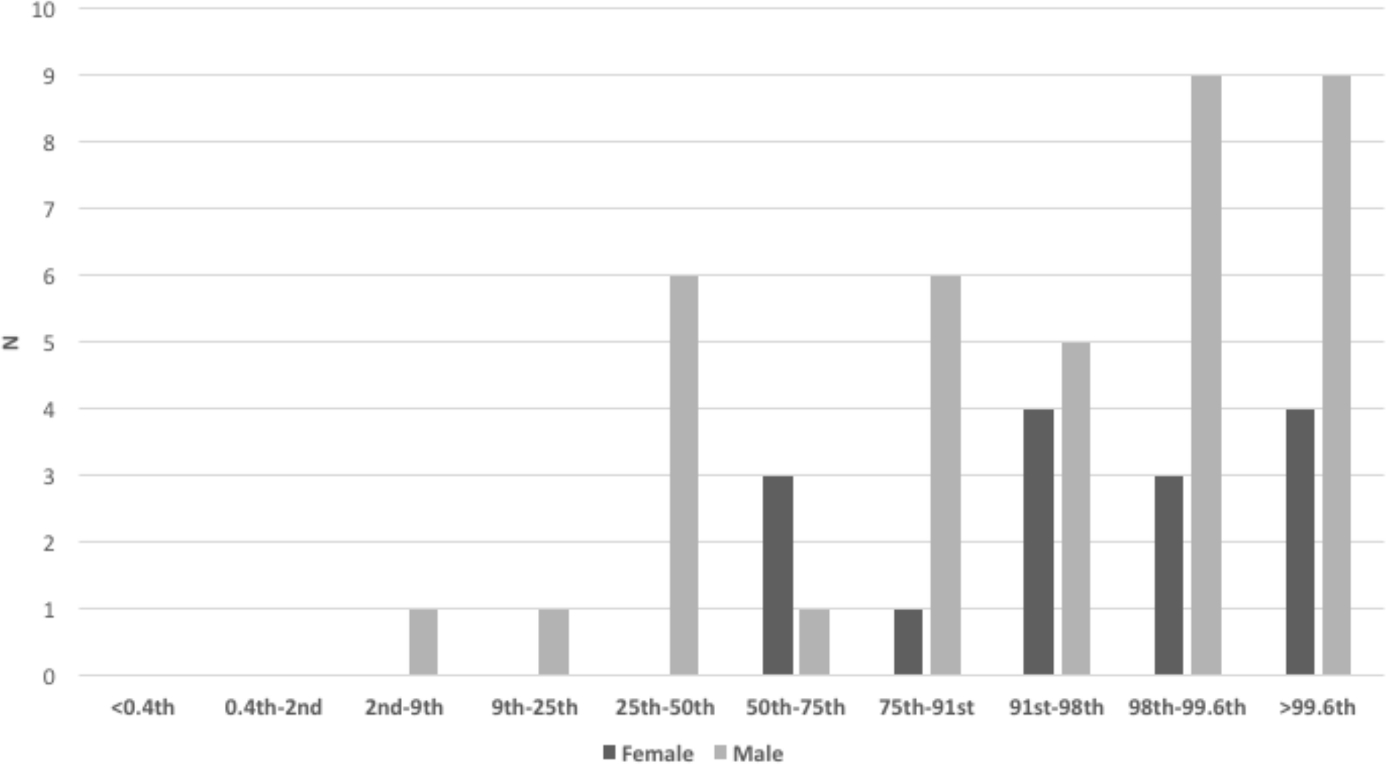
Distribution of United Kingdom sex- and age-adjusted weight centiles.
Two out of the 56 patients had Trisomy 21 (Down's Syndrome) over the three years. The incidence of Down Syndrome in Northern Ireland is ∼30/year, equating to approximately 1/1000 births. 12 Therefore, Down Syndrome has an approximate 30-fold relative risk (RR = 29.798 (95% CI 6.826 to 130.084); p < 0.0001) for developing SUFE. Both these patients had serology demonstrating hypothyroidism. No other cases of hypothyroidism were observed.
Time to presentation
Median time to presentation was 33 days (interquartile range (IQR) 15.5 to 76.5), with a subsequent median time to presentation to service of one day (IQR 0 to 6.5). All delayed presentations outside this median time frame had isolated knee pain as a feature, where the mean time to presentation was 22 days versus 11 days if hip pain was the only presenting symptoms.
Presenting symptoms were recorded. Most patients (87.5%) had two or more symptoms, most commonly hip pain in combination with an additional symptom (42/56 patients, 75.0%). When additional symptoms were analyzed, the most common was a limp in 17/32 (53.1%). A history of a preceding ‘traumatic’ event, e.g. fall etc, was reported in a 12/33 (36.4%).
Overall, ten hips (17.9%) were ‘unstable’ according to the Loder classification, with children being unable to mobilize, even with the assistance of crutches. Onset was acute in 20/56 (35.7%), chronic in 23/56 (41.1%) and acute on chronic in 13/56 (23.2%). Of the latter, two-thirds had a preceding traumatic mechanism.
Radiological classification
Radiological assessment of the Southwick Angle was performed on the Lauenstein/frog leg lateral radiograph. The mean Southwick angle was 23.4° sd 14.7° (1.6° to 62.2°; IQR 11.2° to 33.4°). There was a total of 33 grade I slips (58.9%), 20 grade II (35.7%) and three grade III slips (5.4%).
At the time of surgery, intraoperative fluoroscopy demonstrated a reduction in slip angle in 26/52 (50%), either by way of serendipitous, or formal closed, reduction. There were four open reduction procedures. Fixation was by way of a single cannulated screw in 50/56 (89.3%), with the remainder using two parallel screws.
Complications, contralateral slips and prophylactic pinning
There were no occurrences of chondrolysis. One case of coxa vara was noted. There were two revisions of metal work fixation for screw migration/grew off the screw. There were two modified Dunn procedures performed for unilateral SUFE, neither of which developed AVN at latest follow-up. In total, AVN developed in 4/54 (7.1%) of cases, which is comparative with the previous study cohort. 9 These tended to be overweight, unstable, high grade slips. Patient characteristics of those who developed AVN versus those who did not is demonstrated in Table 1, and representative radiographs are shown in Figures 4 to 7.
Group comparison of those developing avascular necrosis (AVN) versus those who did not
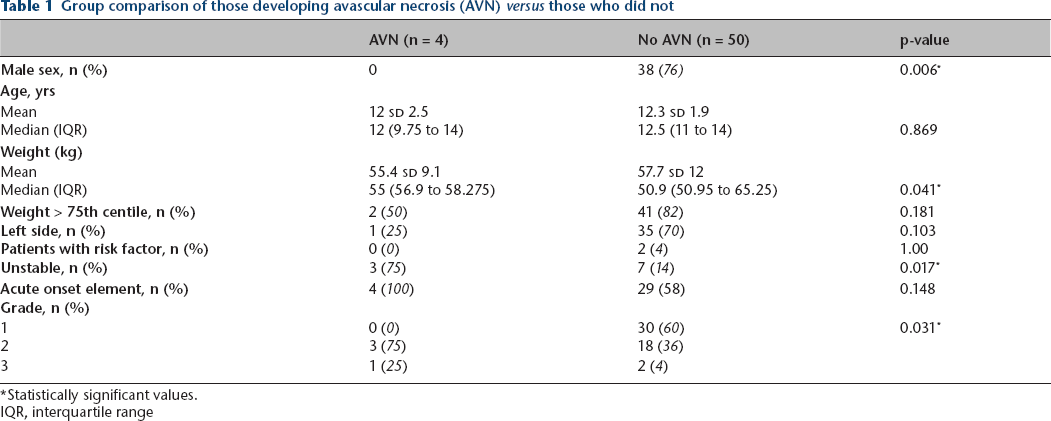
Statistically significant values.
IQR, interquartile range
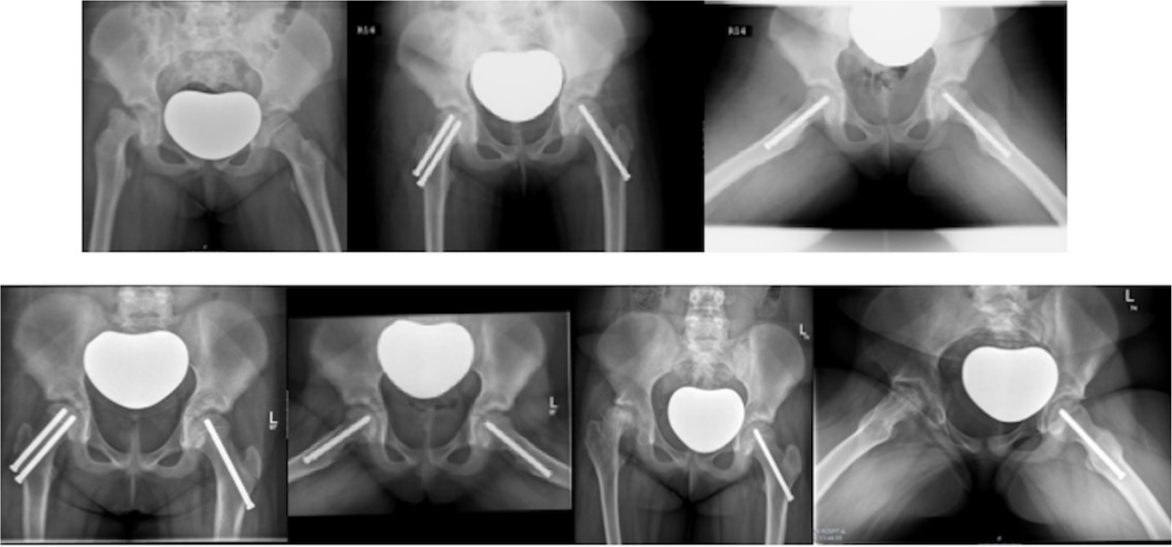
Radiographs of Patient 1 who sustained right hip avascular necrosis (AVN). A nine-year-old female, weight 51.5 kg (99.6th centile) with an acute grade 3 slipped upper femoral epiphysis (Southwick 62.2°) treated with open reduction. Pre- and immediate postoperative radiographs (top). Postoperative films at six and 21 months demonstrating AVN of the right hip (bottom).
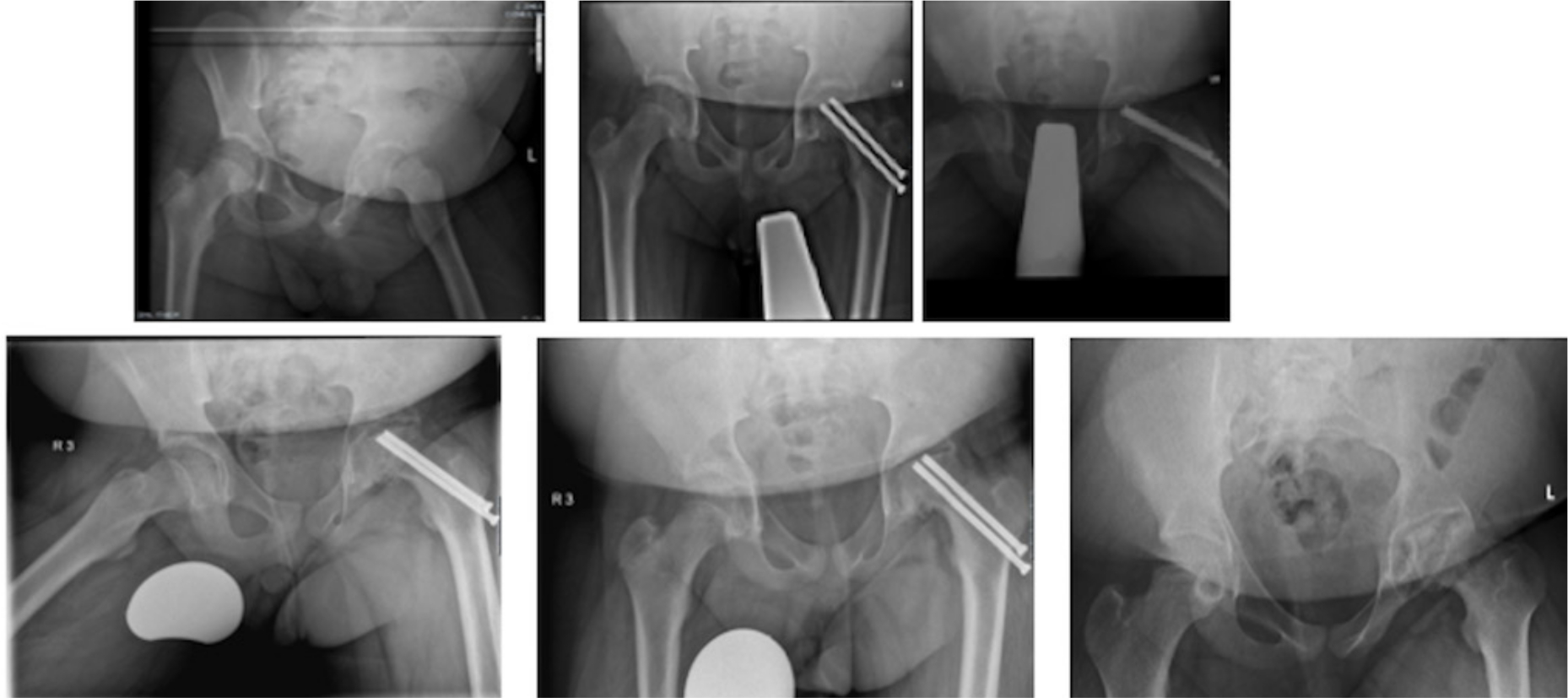
Radiographs of Patient B who sustained left hip avascular necrosis (AVN). A 13-year-old boy, weight 65 kg (98th centile) with an acute grade 2 slipped upper femoral epiphysis (SUFE) (Southwick 34.5°). Pre- and immediate postoperative radiographs (top). Postoperative films at five and 15 months demonstrating AVN of the left hip (bottom).
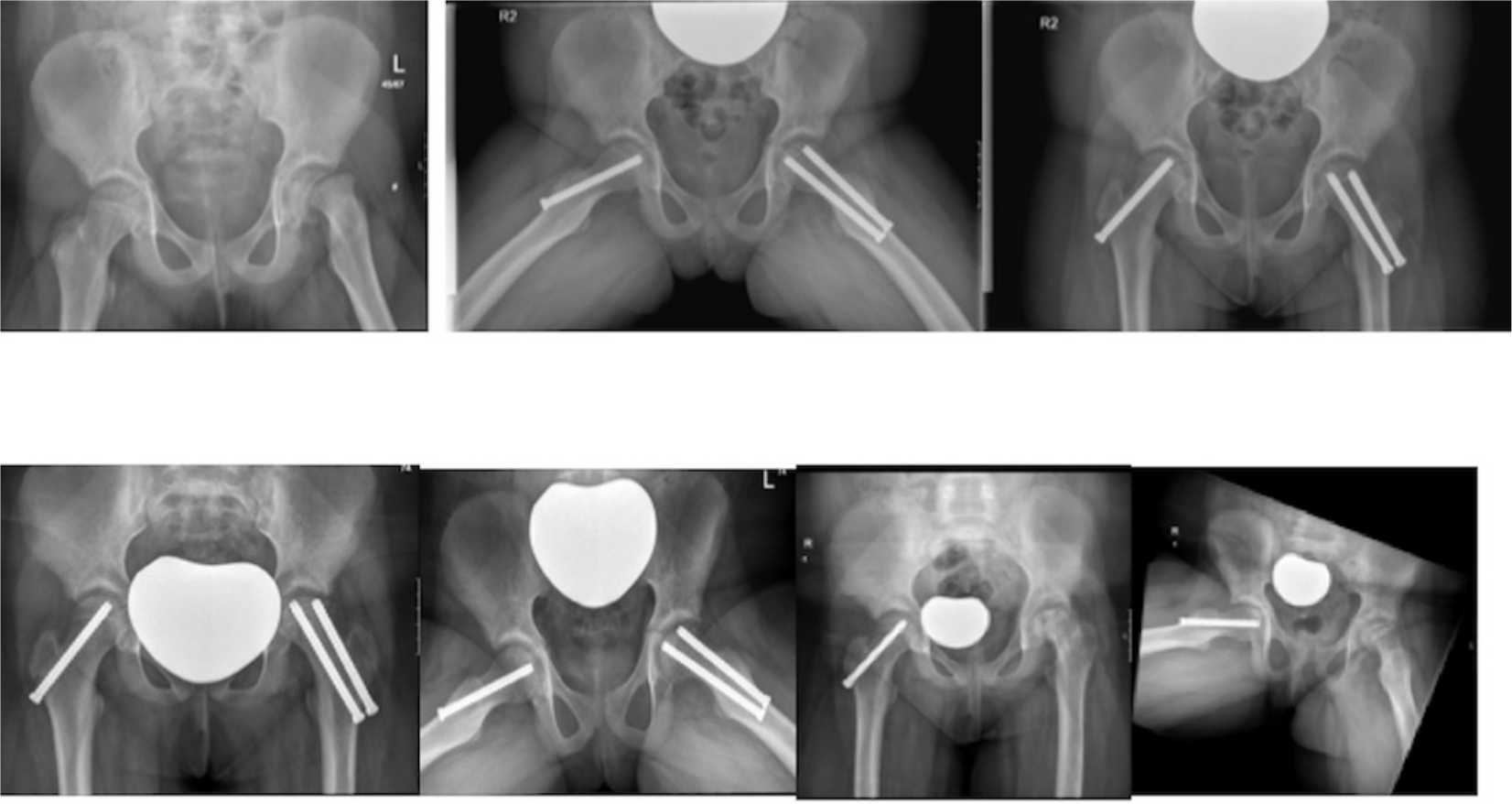
Radiographs of Patient C who sustained left hip avascular necrosis (AVN). An 11-year-old female patient, weight 45 kg (75th centile) with an acute grade 2 (Southwick 31.5°) slipped upper femoral epiphysis. Pre- and immediate postoperative radiographs (top). Postoperative films at three and six months demonstrating AVN of the left hip (bottom).
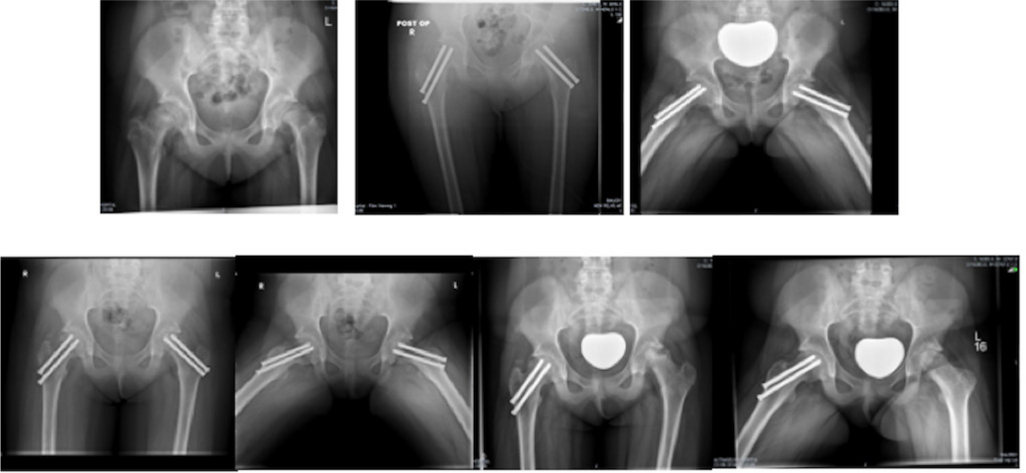
Radiographs of Patient D who sustained left hip avascular necrosis (AVN). A 14-year-old female, weight 50.9 kg (50th centile) with bilateral acute on chronic grade 2 slipped upper femoral epiphysis (SUFE), treated with open reduction. Pre- and postoperative radiographs of staged bilateral SUFE (top). Postoperative films at five and ten months demonstrating AVN of the left hip (bottom).
There were two simultaneous bilateral SUFEs. Of the remaining patients, 14/54 (25.9%) patients underwent contralateral prophylactic pinning. These patients tended to be significantly younger (11 sd 1.9 versus 12.8 sd 2.0 years; p = 0.006) than those who were not prophylactically pinned on the contralateral side. Proportionately more of these patients (9/14, 64.3%) were above the 95th centile for weight, but it this not statistically significant.
Of the remaining 40 hips, a contralateral slip occurred as an isolated event in a further 11 patients, giving a contralateral slip rate of 27.5%. All contralateral slips presented as separate episodes, with confirmatory history and examination findings, and radiological signs indicating SUFE. Of these separate events, ten were grade I and one grade II. Median time to the contralateral slip was 91 days (IQR 47.5 to 296; mean 174.5 sd 164.4). Table 2 summarizes the prophylactic fixation and single side fixation groups, whilst Table 3 summarizes the contralateral slip event versus no subsequent slip. There was no significant difference between this latter subgroup cohort.
Comparisons of the prophylactic pinning group versus those unilaterally pinned for slipped upper femoral epiphysis
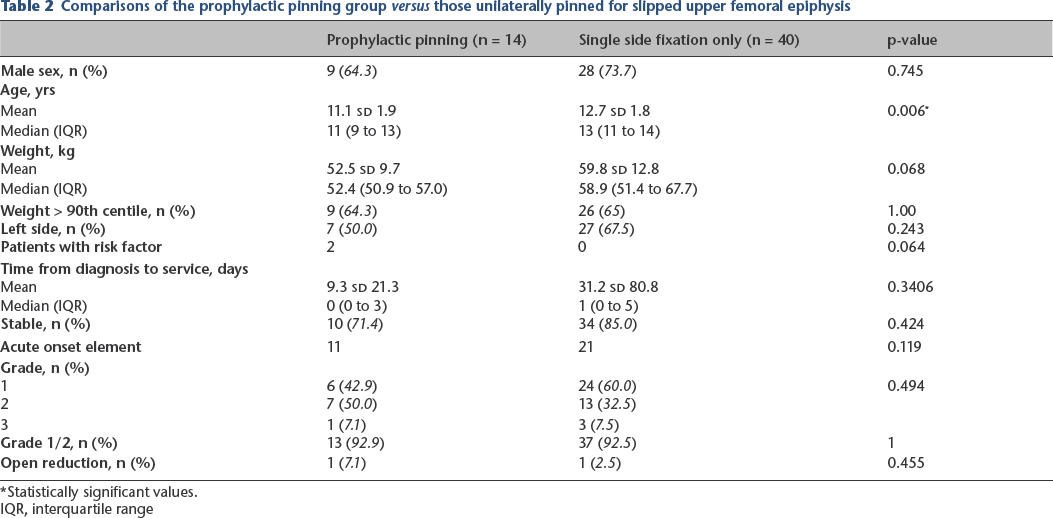
Statistically significant values.
IQR, interquartile range
Group comparison of those sustaining a contralateral slipped upper femoral epiphysis versus those who have not had a second slip event
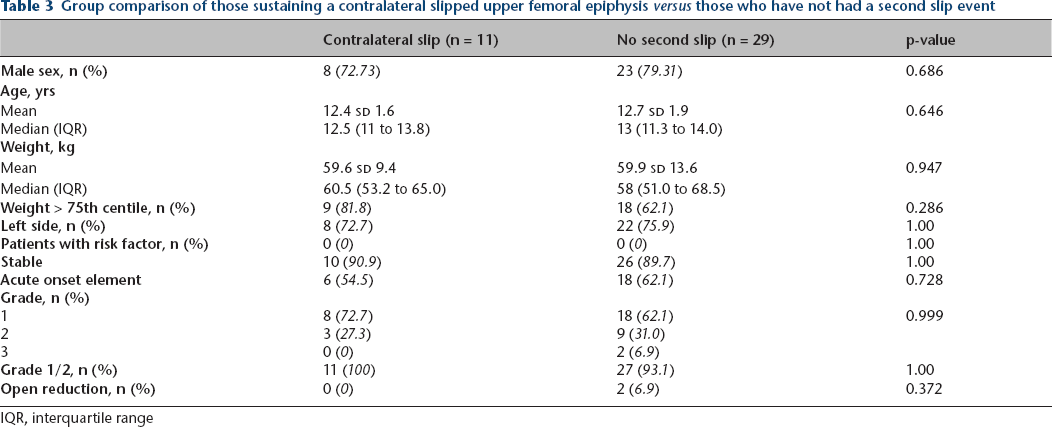
IQR, interquartile range
Comparison of second slip event versus no subsequent slip demonstrated no difference in patient demographics. Table 4 summarizes the data.
Group comparison of contralateral slips versus those prophylactically fixed
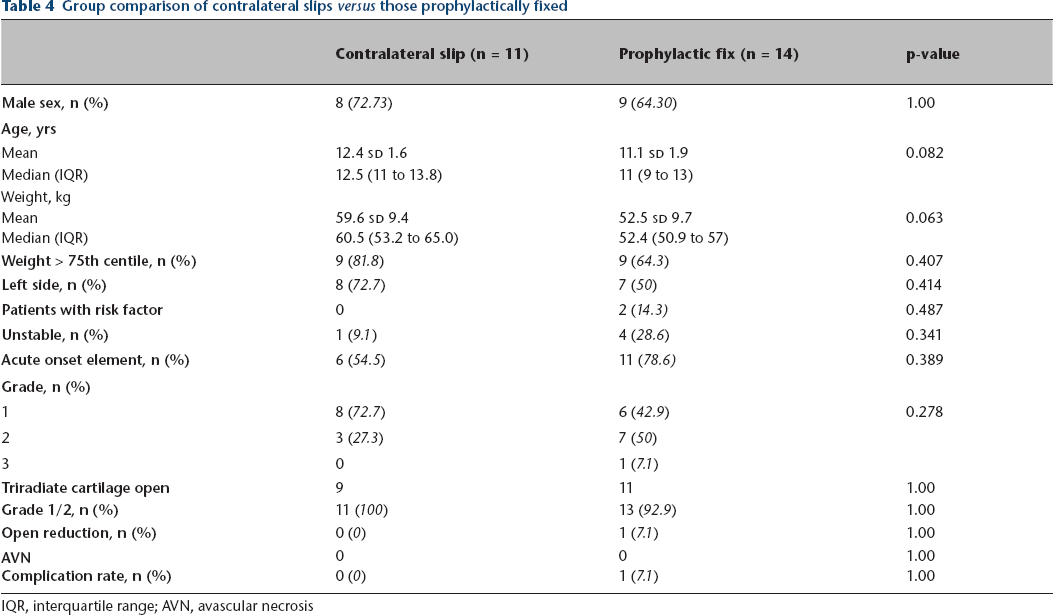
IQR, interquartile range; AVN, avascular necrosis
Discussion
SUFE is a common orthopaedic presentation in the paediatric patient. However, delay in diagnosis can convey a significant long-term morbidity, with life changing complications. The underlying pathophysiological mechanism remains unclear but is felt to be due to multiple biomechanical, biochemical and mechanical factors that result in weakening and failure through the hypertrophic zone of the paediatric physis, often occurring during the pubertal growth spurt, between the ages of 12 and 15 years. 13
During this period, androgenic hormones increase chondrocyte proliferation, increasing the physeal height, weakening the perichondral ring with resultant loss of physeal strength. This is felt to account for higher rates in male cases, where testosterone is known to reduce physeal strength. 14 Recent literature implicates pro-inflammatory mediators, with subsequent down-regulation of type II collagen in SUFE patients versus normal controls. The loss of these proteins leads to microarchitecture softening, enhanced inflammatory response and weakening of the physes resulting in SUFE.15–21 Increased weight, body mass index and height at the upper centiles have all been reported to predispose to SUFE.22–24 Additional risk factors including local physeal morphology such as decreased femoral anteversion, increased physeal slope, deeper acetabular sockets or increased centre-edge angles have also been suggested. 24
The presence of endocrine and pituitary axis disorders has also been implicated in its pathogenesis. These disorders are often found to be increased in overweight individuals compared with normal controls.4,8,13,22,23,25–29 In our study, two patients had Down Syndrome and associated hypothyroidism. Bosch et al 30 has reported that patients with Down's syndrome and SUFE have a higher incidence of hypothyroidism. Outcomes in these cohorts are poor, highlighting the need for hip screening in this specific population. 31
The risk of SUFE has been shown to be increased in Black, Hispanic and Polynesian children.2,3 Equally, these populations have been shown to be increasingly overweight compared with Caucasian counterparts, however, childhood obesity appears to be increasing as a whole in all races.2,3 Lehmann et al 3 found a static incidence in the United States, but reported an increasingly earlier age at onset. In the United Kingdom, Murray and Wilson 8 demonstrated an earlier onset, in conjunction with increasing childhood obesity, but also a 2.5-fold rise in the incidence of SUFE in Scotland from 1981 and 2000.
Whilst literature regarding patient characteristics is consistent, incidence rates vary by geography considerably. Table 4 provides a synopsis by country. A study from New Mexico, United States demonstrated an increase in the incidence of SUFE from 2.13 to 5.99/100 000 children, occurring over a 40 year period, which occurred in conjunction with rising childhood obesity rates, especially in overweight male children. 4 However, the study was confounded by the possibility of earlier diagnosis and better health care provision over this time frame. Australasia has also demonstrated increases in SUFE, especially in Aboriginal and Maori populations, where patients tended to be younger and overweight.5,32 Singapore, Korea and Japan have all demonstrated increasing incidences in SUFE which appear to be in conjunction with rising levels of childhood obesity.6,7,33
Witbreuk et al 1 reported the Dutch incidence of 11.6 per 100 000 children aged between five and 19 years of age. Interestingly, whilst there was no significant difference in gender, the number of affected female children was found to be increasing.
Their review reported a male:female ratio range from 1.4 to 4.1. Our current study lies within this range with a ratio of 2.6, and agrees with a rising trend in female presentations with an increase from a ratio of 1.8 reported previously. 9
Two consistencies are noted across geographical regions – a rising incidence in association with a worldwide increase in obesity levels, particularly in the latter half of the 20th century. 34
A recent United Kingdom-based review of a general practitioner database not only reiterated the link between SUFE and obesity, but also demonstrated higher rates of SUFE in areas of socioeconomic deprivation. 35 Additionally, knee pain was found to delay diagnosis, with 75.4% of these patients having multiple episodes of primary care contact. Whilst the predominant symptom in our study was hip pain, we still had a significant mean time to presentation of almost five weeks, suggesting that definitive diagnosis is delayed due to either an initial failure to seek medical attention, or failure to appreciate referred pain to the knee as a presenting symptom. This reinforces the educational message to consider SUFE in adolescents presenting with knee pain.
Understanding the temporal changes of SUFE may have far-reaching impacts on service provision and potential restructuring, as declines in incidence may result in management of SUFE being transferred to specialist centres.
Temporal changes and the decline in SUFE incidence may impact on service provision, channelling these cases to specialist centres. In 2002, the senior authors reported a regional incidence of 7.14/100 000, 9 which was within the range quoted by the literature (Table 5). In the following 15 years, the Public Health Agency has published data which demonstrates a rising childhood obesity epidemic in Northern Ireland, with 18% of children aged two to 15 being classed as obese – a figure which has doubled since 1999 and remained static in the last five years. 36 It should be noted that ‘obesity’ refers to > 95% centile for body mass index, but there is no corresponding value for age-sex matched paediatric growth charts in order to draw a direct comparison. The current study agrees with the literature demonstrating a link between childhood obesity and SUFE. However, we have demonstrated a recent reduction in SUFE incidence rates from 7.14/100 000 to 4.69/100 000 population aged 16 years or younger.
Review of study incidence rates and temporal changes if applicable
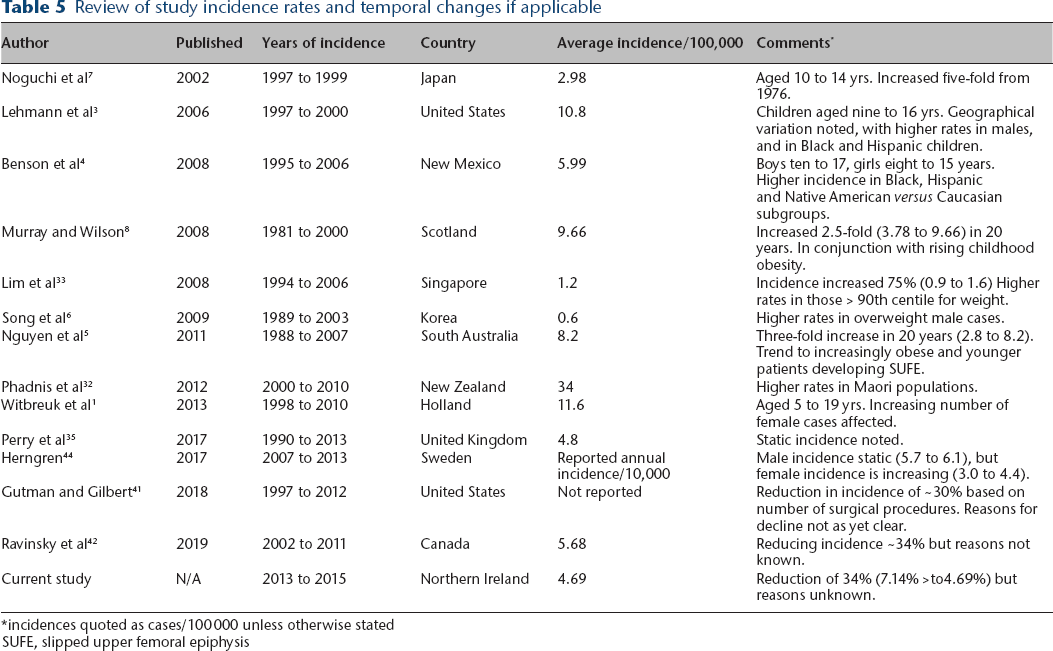
incidences quoted as cases/100 000 unless otherwise stated
SUFE, slipped upper femoral epiphysis
The study strengths are the robust follow-up, with no loss to follow-up or missing cases in the study time frame, detailing the change in incidence at a regional level. Our figures indicate a declining incidence, the exact reasons for which are unclear. It may reflect a more sedentary population, with a reduction in the presentation of traumatic acute on chronic slips. Whilst a history of preceding trauma was reported in approximately one in four cases (14/53; 26.4%), there is a lack of literature reporting the traumatic incidence of SUFE. However, the incidence of paediatric fractures is reportedly in decline, which may in part explain the decreasing number of SUFE cases if one considers SUFE as a Salter-Harris type I physeal injury.37–39
The paper is limited by its retrospective nature. This is a common finding for many publications on SUFE, as there is a lack of high quality prospective multicentre studies from which to derive further conclusions. The overarching principle of SUFE treatment is to prevent AVN in the adolescent period and to minimize the risk of secondary osteoarthritis long term. 40 This paper demonstrates that whilst SUFE demographics within Northern Ireland are similar to other published studies, our incidence rate is decreasing. Heights were not available for all patients, and as such body mass index could not be calculated for all patients. We, therefore, used age- and sex-adjusted weight centiles, and the results appear to correlate with the conclusions based on body mass index. As such, we feel that this should not limit the validity of the study.
The current study serves as a recent epidemiological follow-up study showing the decrease in incidence of SUFE on a regional perspective, with appropriate treatment protocols. Two recent studies have demonstrated a reduction in SUFE incidence in the United States and Canada.41,42 Both studies concluded the reasons for this are unclear, and further epidemiological studies are required to determine if this is reflected in other geographical regions. Larger cohort studies are currently underway, specifically the United Kingdom-based British Orthopaedic Surgery Surveillance on SUFE, 43 and whilst the results of this study are yet to published, it will be interesting to see how our national data of Northern Ireland compares with a large prospective longitudinal cohort study.
If the reduction in SUFE is true, and echoed elsewhere, this could impact on delays in diagnosis with increased morbidity as the condition becomes less common. Implications for healthcare systems are that they require restructuring. One could argue that experienced surgeons in high volume centres should be managing all SUFE cases in order to optimize postoperative outcomes, moving the treatment away from the occasional District General Hospital trauma surgeon.
Conclusion
Clinician vigilance and prompt recognition, especially for atypical presentation of SUFE, is essential in reducing the associated long-term morbidity. Patient characteristics remain relatively unchanged from the previous study in 1999, and are similar to those described by Loder 20 years ago. 2 However, our incidence of SUFE is unexpectedly in decline compared with 1999. This requires sustained, longitudinal, prospective epidemiological surveillance and comparison with other countries to examine this trend further.
Footnotes
JB: Study concept, Manuscript preparation and editing.
AC: Study concept, Data collection and analysis, Manuscript preparation and editing.
All authors have been involved in the study and completion of the manuscript. All authors have read and approved the final manuscript for submission.