
Abstract
Abstract
Purpose
Supracondylar humerus fractures are among the most common injuries in the paediatric population, accounting for 16% of all paediatric fractures and roughly 60% to 70% of all paediatric elbow fractures. Typical treatment for displaced and unstable supracondylar humerus fractures is surgical intervention, often with percutaneous Kirschner-wire (K-wire) fixation. Timing of surgery is dependent on the patient's neurovascular status on presentation, with surgical emergencies being performed at all hours of day and night. Percutaneous fixation of paediatric elbow fractures can be challenging as a result of the propensity for the elbow to become quite swollen with these fractures, particularly in smaller and physiologically more immature elbows.
Methods
We have developed a simple operative technique to guide placement of percutaneous wires for supracondylar humerus fractures using a hypodermic needle as a reference marker.
Results
In our experience, trainees utilizing this technique demonstrate greater appreciation for start point and trajectory of wires during percutaneous pinning, with better communication amongst surgical team members about necessary adjustment for optimal placement of K-wires.
Conclusion
Utilization of this technique has the potential to refine surgical technique by minimizing errant wire passes, radiation and operative time when performing percutaneous pinning of reduced type III supracondylar humerus fractures.
Level of Evidence
V, Novel Surgical Technique
Keywords
Introduction
Supracondylar humerus fractures are among the most common injuries in the paediatric population, accounting for 16% of all pediatric fractures. 1 Typical treatment for displaced supracondylar humerus fractures is a closed reduction and fixation with percutaneous Kirschner (K)-wires.2–4
We have developed a simple technique to guide placement of percutaneous wires for supracondylar humerus fractures using a hypodermic needle as a reference marker. Pin placement is a critical component of fixation in the supracondylar humerus fracture. Both biomechanical and clinical data support the utility of accurate wire placement.3–5
Our technique uses a widely available hypodermic needle to act as a radiographic and clinical reference for the placement of percutaneous wires. This simple and easy to execute tactic has the potential to minimize errant wire passes, minimize radiation and decrease operative time and frustration.
Surgical technique
The only equipment needed for this technique is a 20-gauge hypodermic needle. This is often already on the field as a means to administer local anaesthetic at the end of the case.
The hypodermic needle is used as a reference point to guide placement of the first percutaneous wire. In order to successfully place a wire, the surgeon must understand four variables: coronal plane wire direction, coronal plane wire starting point, sagittal plane wire direction and sagittal plane wire starting point. The hypodermic needle allows for precise understanding of the sagittal plane starting point and direction while the surgeon uses fluoroscopy on anteroposterior imaging to place the first wire.
The surgeon may use whatever reduction methods deemed necessary to reduce the fracture. Once the surgeon has a satisfactory reduction and control of the fracture as demonstrated by radiograph, the hypodermic needle is firmly placed by hand into the soft bone of the capitellum (Figs 1a and 1c). It does not matter where it is placed, as the hypodermic needle is only a reference mark for the first wire.
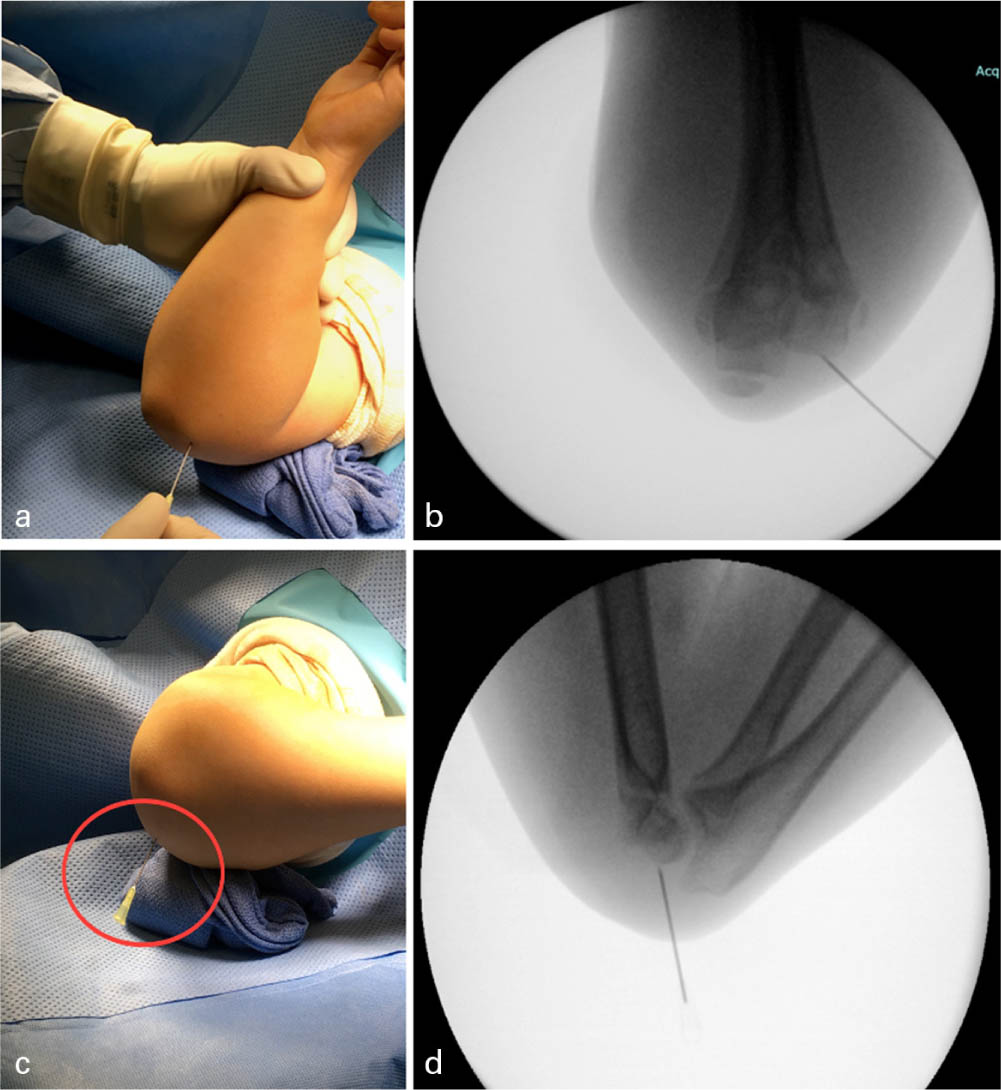
Hypodermic needle placed percutaneously (A) to create reference guide for K-wire placement via visualization of needle on lateral intraoperative fluoroscopic image (B).
Fluoroscopic images are obtained using the C-arm with just the needle inserted through the skin and firmly into the bone of the distal lateral humerus (Figs 1b and 1d). We then transfer the lateral fluoroscopic image to the second screen (often the ‘right-hand screen’ on a standard C-arm imaging system) using the last image hold functionality of the C-arm, and continue to use the ‘left-hand screen’ for any additional radiographs.
The lateral image demonstrates starting point and trajectory of this hypodermic needle. The surgeon can then choose more precisely where to start the first K-wire, and which direction to aim in the sagittal plane (Figs 2a and 2b), allowing for appropriate adjustments to be made with reference to the needle. For example, if the hypodermic needle is placed anteriorly with an anterior trajectory, the surgeon can then choose a posterior starting point and diverge from the hypodermic needle. The K-wire can then be placed on the anteroposterior fluoroscopic image, with confidence and understanding of placement in the sagittal plane.
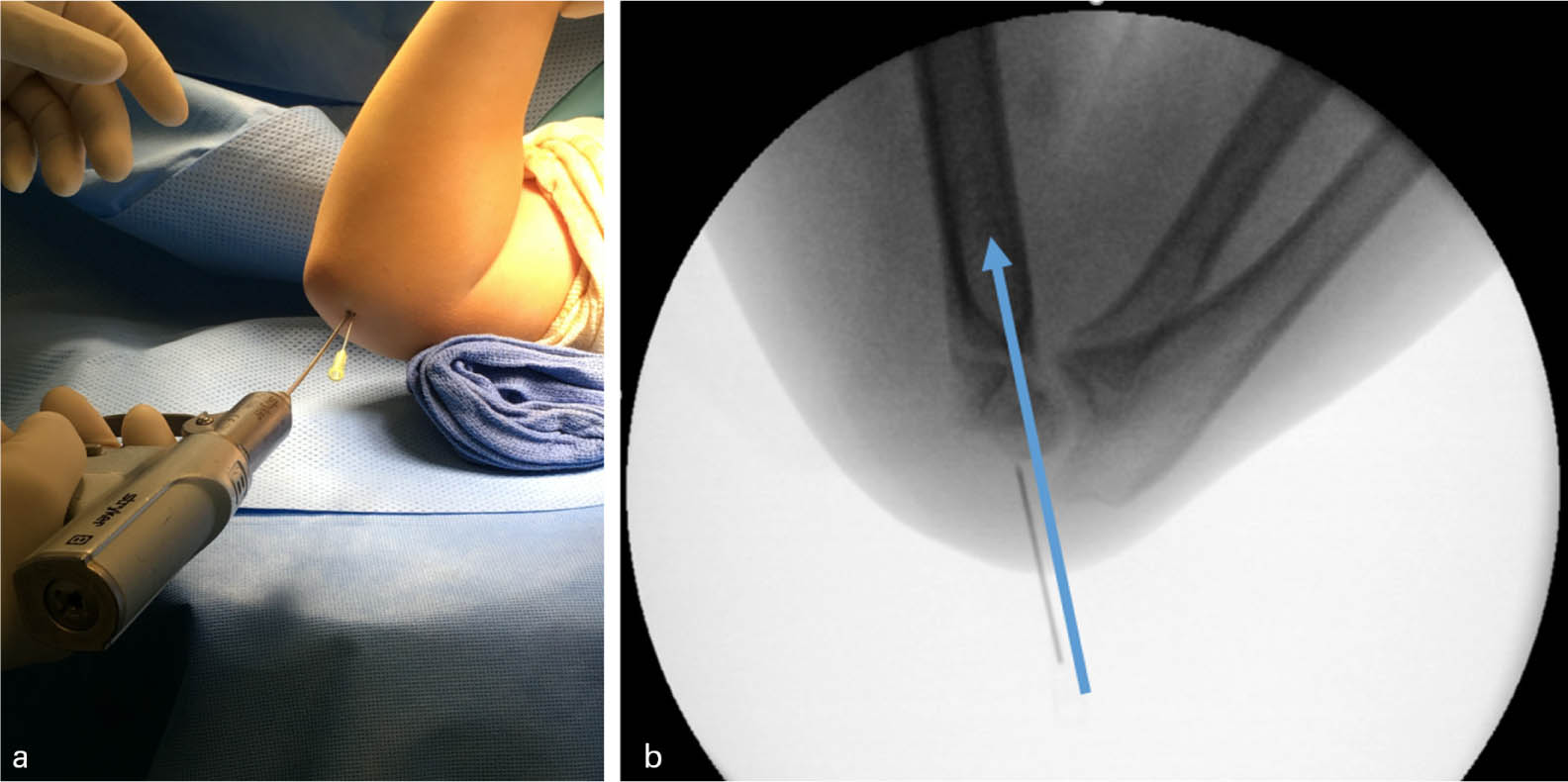
Initial percutaneous K-wire can be placed with reference to previously placed percutaneous hypodermic needle to establish start point (A), and lateral plane pin trajectory can then be decided with reference to the previously placed hypodermic needle (B) without the need for additional intraoperative fluoroscopic images.
After the placement of the first successful wire, the hypodermic needle is removed by hand. That first wire can then be used as the reference guide – in a similar fashion to the hypodermic needle for the first wire – to guide placement of the second, and if needed, third wires.
This technique has been utilized by residents and fellows at our institution over the course of several years to simplify the 3D spatial awareness and triangulation of K-wire placement. Both junior and senior staff have been introduced to this technique through rotating trainees, and have found the technique to be a useful adjunct in addition to personal teaching styles.
Out of high concern for safety, it is worth noting that this hypodermic needle technique should only be performed on the lateral side of the elbow. The proximity of the medial sided neurological structures makes blind passage of a hypodermic needle hazardous.
Discussion
The standard treatment for displaced supracondylar humerus fractures is closed reduction and percutaneous pinning (CRPP) with fluoroscopic assistance. Accurate pin placement is essential to achieve mechanical stability and avoid loss of reduction.3–5 Radiation exposure may be increased for displaced and unstable fracture patterns for both the patient and operating room staff. Multiple authors6–7 have reported a wide range of fluoroscopy times ranging from 30.7 seconds to 126 seconds during CRPP of supracondylar humerus fractures. Additionally, Hsu et al 8 showed that when the image intensifier serves as the operative table, the radiation exposure was significantly higher for the patient's operative arm and the surgeon's neck.
This simple technique is helpful for the less experienced surgeon, or even the more experienced surgeon training residents and fellows. The spatial understanding of the swollen paediatric elbow with its diminutive anatomy is difficult. Placement of wires can be difficult for novice surgeons and trainees, especially when a reduction is unstable and superficial landmarks are not easily palpable. This technique seeks to reduce the number of false passes allowing the provider placing the pins to understand the direction of their drilled wires in two planes.
We find this technique allows for both the surgeon managing the reduction and the operator drilling the wire to communicate about the correct direction of the K-wires to stabilize the fracture. The lateral fluoroscopic image showing the location of the hypodermic needle allows both providers to agree on the direction and location of the first K-wire starting point, while watching the pin insertion on the anteroposterior image.
Operative treatment of unstable supracondylar humerus fractures can become demanding, especially when multiple wire passes are needed. We find that this technique minimizes the number of wire passes. The skill of percutaneous K-wire fixation after closed reduction of supracondylar fractures can be taught in a reproducible fashion.
Footnotes
BJS: Study design/technique description, Manuscript preparation.
SM: Study design/technique description, Manuscript preparation.
EC: Manuscript preparation.
CJM: Study design/technique description, Manuscript preparation, Figure preparation.