
Abstract
Abstract
Purpose
The presence of a clubfoot is often found prenatally and some families seek counselling with a specialist. The purpose of this study was to compare the parental anxiety levels in families that: a) knew prenatally and had prenatal counselling; b) knew prenatally but did not seek prenatal counselling; and c) did not know until after delivery.
Methods
This prospective cohort study evaluated the anxiety of parents as they presented to the paediatric orthopaedic clinic with their newborn with a foot disorder (prior to the diagnostic confirmation of clubfoot). Each family filled out the ‘Pre-visit orthopaedic surgeon questionnaire’ and then after the initial visit with the orthopaedic surgeon (confirming the clubfoot diagnosis) the family filled out the ‘Immediately post-visit orthopaedic surgeon questionnaire’. Through these questionnaires, anxiety level was assessed prior to meeting postnatally with the paediatric orthopaedic specialist, as well as after the meeting and compared across groups.
Results
A total of 121 parents completed questionnaires: 71% (86/121) confirmed clubfoot; 69% of families (59/86) received prenatal counselling (Group A); 16% (14/86) knew prenatally but had no counselling (Group B); and 15% (13/86) found out at birth (Group C). There was no difference in anxiety levels across groups before (p = 0.78) or after (p = 0.57) meeting with the paediatric orthopaedic surgeon; however, overall anxiety reduced significantly (p < 0.001).
Conclusion
We found no difference in the anxiety levels of across the three groups. Prenatal counselling for parents of children with likely clubfoot may not decrease parental anxiety, but nonetheless is very appreciated by the families who receive it.
Level of Evidence
Prognostic Level II
Introduction
With increased prenatal screening, foot and musculoskeletal anomalies are often found on routine obstetric ultrasound. The rate of prenatal detection is increasing as sonographic technology improves,1,2 however, some anomalies are not found prenatally and are a surprise to the family at the time of delivery. For those that are found prenatally, the option for prenatal counselling with a paediatric orthopaedic surgeon who specializes in childhood foot disorders may be offered.3,4 Some choose to pursue this and others decline. The benefits of this prenatal counselling are difficult to measure and are typically related to parental anxiety about the diagnosis and treatment, however, it has been challenging to measure this impact.
Radler et al 2 found that clubfoot is detected prenatally in the United States about 60% of the time, but that the detection rate was increasing. They also found that mothers in the United States strongly preferred to know about their child's likely foot deformity prenatally. When a foetus is found to have a foot in the clubfoot position prenatally, this correlates to a true clubfoot postnatally approximately 70% of the time.5,6 When a possible clubfoot is discovered prenatally, a thorough anatomic ultrasound screen is indicated, 7 as clubfoot can be associated with other anomalies in up to 67% of cases.1,4,8 When a foetus is found with a foot in the clubfoot position, many advocate for prenatal counselling.3,4,9,10
Several studies have shown the diagnosis of clubfoot may have a negative impact on the psychological wellbeing of the mother and family.11–13 Notably, Coppola et al 11 compared mothers of normal babies with those born with congenital clubfoot and found there was a significant negative impact on stress and depressive symptoms in the mothers of children with congenital clubfoot. Among other theories, the negative impact on the mother's psychosocial wellbeing was postulated to be related to the finding of a congenital malformation that disturbed the parents’ expectation of a ‘perfect’ child; this has also been noted in other studies including those on cleft lip and palate and upper extremity malformations.11,12 In families where the suspicion of clubfoot is noted prenatally, and for those who had the opportunity to meet and discuss treatment and outcomes of congenital clubfoot with a paediatric orthopaedic surgeon who specializes in clubfoot, it is possible that this early discussion may mitigate some of the anxiety and depressive symptoms found in these mothers.
The purpose of this study was to compare the self-reported anxiety of parents who presented to the orthopaedic clinic with a newborn foot anomaly (prior to the confirmed diagnosis of clubfoot) that was suspected prenatally and had prenatal counselling, with those who suspected the possible deformity and did not have prenatal counselling, with those who did not discover the possible deformity until the delivery of the child.
Materials and methods
We performed a prospective study of families presenting to a tertiary-care paediatric orthopaedic surgery clinic after referral of their newborn (< 30 days old) due to the presence of a foot deformity. While we were interested in parental anxiety due to clubfoot, we had to approach all families with possible foot deformity prior to the confirmation of clubfoot diagnosis in order to obtain their anxiety levels unbiased by the physician visit. Some of these families had prenatal suspicion of clubfoot, and for those families some of them met prenatally with a member of our paediatric orthopaedic team who specializes in clubfoot treatment. We have three paediatric orthopaedists who counsel families found prenatally to have possible clubfoot, and the counselling sessions vary by physician but typically cover aetiology, diagnosis, treatment and expected outcomes of idiopathic clubfoot. Included in that counselling session are props including clubfoot model, foot abduction brace and patient photo book; families are provided with an informational handout.
Institutional review board approval was obtained from our institution prior to initiation of this study. Families were approached by the research staff prior to meeting the paediatric orthopaedic surgeon or associates (including residents, fellows or advanced practice providers). Families were excluded if they presented with a child older than 30 days, met with an orthopaedic provider in the newborn nursery or had multiple known congenital anomalies. Families who entered into the study but whose child was found subsequently to not have a clubfoot were not included in further analysis about levels of anxiety.
If the families agreed to participate in the study, after informed consent was signed, they were asked to fill out a ‘Pre-visit orthopaedic surgeon questionnaire’. This was a questionnaire constructed by our team for the purposes of this study (Appendix 1). This noted any prenatal diagnosis received, any counselling received and the source of information obtained prenatally. Families also recorded levels of anxiety regarding their child's foot deformity. Immediately after the families met with the paediatric orthopaedic surgeon and the diagnosis of clubfoot was confirmed, they were asked to fill out an ‘Immediately post-visit orthopaedic surgeon questionnaire’ (Appendix 2).
Families whose child had a clubfoot deformity were stratified into those whose clubfoot was detected prenatally and were offered and received prenatal counselling (Group A), those whose clubfoot was detected prenatally but did not have prenatal counselling (either offered and declined, or not offered) (Group B) and those who did not find out about their child's deformity until birth (Group C).
Calculation of sample size and power analysis were done using Monte Carlo simulation and resampling. This was implemented to estimate a minimum required sample size to achieve the goals of this study. We anticipated that parents without prenatal counselling would score around 4 or 5 points on the 1 to 7 Likert anxiety scale while parents who utilized prenatal counselling would score 2 or 3, varying also by when they learned of their child's deformity (prenatally versus at birth). In order to detect a one- to two-point shift in median anxiety score across three groups using a nonparametric Kruskal-Wallis test, we would require at least 51 subjects (approximately 17 per group) to achieve 80% power with alpha set to 0.05. Multiple unimodal sampling distributions were developed to represent possible anxiety score outcomes for each of the three study groups, all with at least a one-point shift in median score. A total of 500 samples were computed for each set of possible distributions and were tested using every sample size between ten and 100, inclusive. The minimum necessary sample to consistently achieve 80% power for the Kruskal-Wallis test was reported.
Anxiety scores between those who received prenatal counselling (Group A), those who did not receive prenatal counselling but found out prenatally about their child's deformity (Group B) and those who did not receive prenatal counselling but found out at birth about their child's deformity (Group C) were summarized by median and interquartile range (IQR; 25th to 75th percentile). Parental, counselling and diagnosis characteristics were summarized for the cohort and by group. Comparisons in anxiety across groups were conducted using the nonparametric Kruskal-Wallis test. Comparisons of anxiety scores before and after meeting with the orthopaedic surgeon were analyzed using a Wilcoxon signed-rank test for paired data. All tests were two-sided and p-values < 0.05 were considered significant.
Results
A total of 121 parents completed questionnaires regarding newborn foot disorder; 86 of these (71%) were confirmed as clubfoot. The majority of the cohort (70/121, 58%) received prenatal counselling after learning of a suspected limb anomaly (Group A), while 16% (19/121) did not receive prenatal counselling but found out prenatally about their child's deformity (Group B) and 26% (32/121) found out at birth about their child's deformity (Group C). True clubfoot was diagnosed in 84% of Group A, 74% of Group B and 41% of Group C. The families whose children were determined not to have clubfoot were then eliminated from further analysis. For the clubfoot only cohort, the majority of the families (59/86, 69%) received prenatal counselling after learning of a suspected clubfoot prenatally (Group A), while 16% (14/86) did not receive prenatal counselling but found out prenatally about their child's deformity (Group B) and 15% (13/86) found out at birth about their child's deformity (Group C). Demographic data and timing of diagnosis of likely clubfoot are noted in Table 1. A response summary to questionnaires by group is detailed in Table 2. In all, 83% (48/58) of parents in Group A reported that they found the prenatal counselling very informative (median response 7; IQR 7 to 7).
Diagnosis characteristics by group for patients diagnosed as having congenital clubfoot (n = 86)
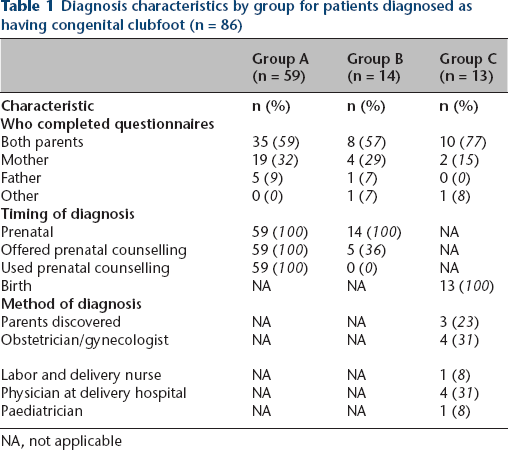
NA, not applicable
Questionnaire responses by group from pre- and post-meeting with the orthopaedic physician
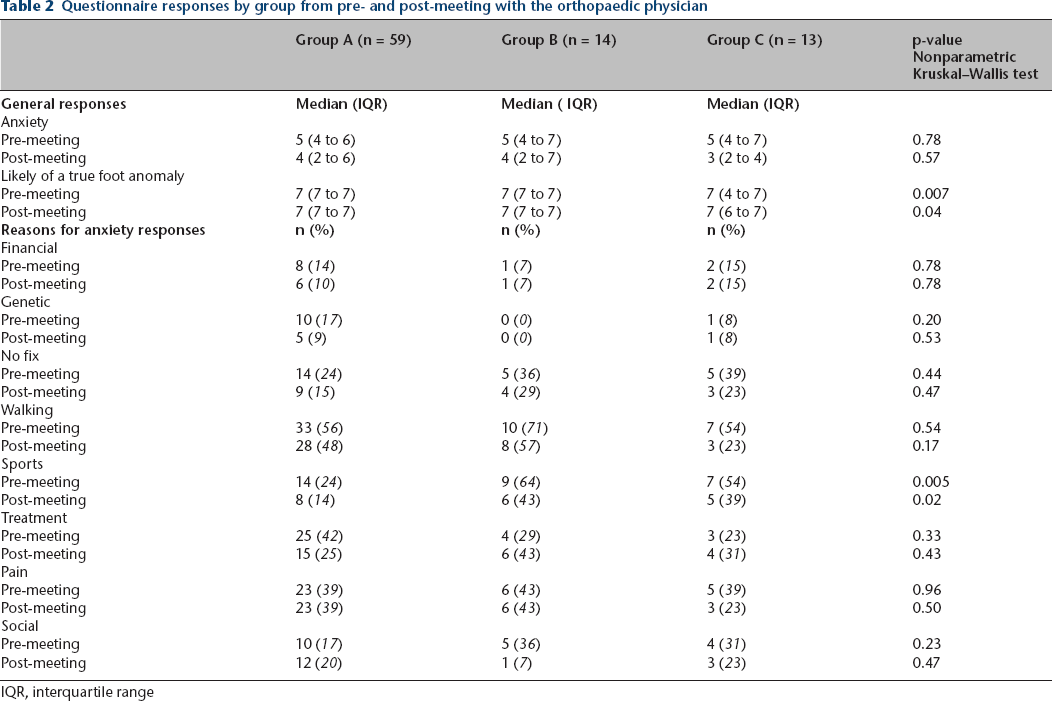
IQR, interquartile range
There was no difference in anxiety scores prior to meeting with an orthopaedic surgeon across all three groups (median 5 (IQR 4–7); p = 0.78) and variation was minimal after meeting with a surgeon (median Group A 4 (IQR 2–6); Group B 4 (IQR 2–7); Group C 3 (IQR 2–4); p = 0.57) (Fig. 1). However, anxiety scores for the cohort changed significantly from a median of 5 (IQR 4 to 7) prior to meeting with the orthopaedic surgeon to a median of 4 (IQR 2 to 6) after meeting with the orthopaedic surgeon (p < 0.001) (Fig. 1). Parents who learned of a potential deformity prenatally (Group A and Group B) experienced a one point decrease in median anxiety level from before to after their meeting with the orthopaedic surgeon; whereas parents who found out at birth, experienced a two point decrease in median anxiety level from before to after their meeting with the orthopaedic surgeon (p < 0.001). In all, 83% (48/58) of parents in Group A reported that they found the prenatal counselling very informative (median response 7; IQR 7 to 7).
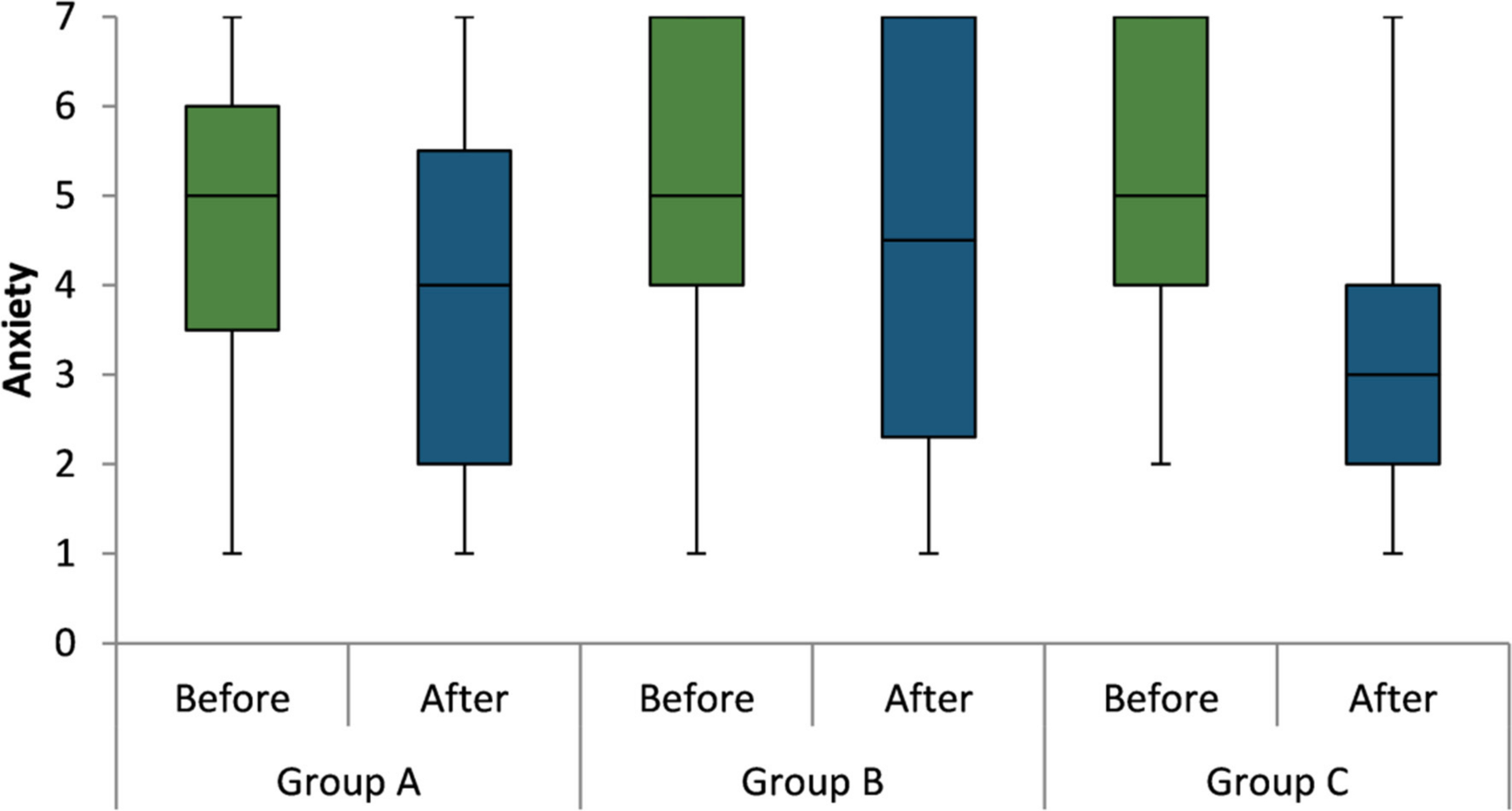
Boxplots of anxiety level before and after meeting with the orthopaedic surgeon for each group. Group A received prenatal counselling after learning of a suspected clubfoot prenatally, Group B did not receive prenatal counselling but found out prenatally about their child's deformity and Group C found out at birth about their child's deformity. The boxes represent the 25th, 50th and 75th percentiles while the I-bars represent the minimum and maximum values.
All families were asked if they pursued ‘information about your child's foot problem other than from a health care provider?’ They were asked to check all that applied (Appendix 1). In all, 87% (75/86) reported seeking information from the internet. Additionally, 35% (30/86) reported asking friends or family about information, 16% (14/86) sought information from textbooks and 2% obtained information from other sources (including books, a paediatrician, doctors and nurses in the delivery room, parent with clubfoot and outside orthopaedist). In total, 93% (80/86) sought outside information regarding their child's foot anomaly.
Discussion
Discovering a newborn child has a congenital anomaly can cause considerable parental anxiety. 14 This anxiety can impact the psychological wellbeing of the mother of a newborn child which may have an impact on the bonding with that child. 11 Some data suggests that maternal anxiety can contribute to subsequent hyperactivity in the child. 15 Clubfoot is a congenital deformity that is formed early in gestation and often detected prenatally as early as 13 weeks. 1 It is discovered on the 18 to 20 week screening ultrasound about 60% to 70% of the time, with some location and socioeconomic variability.2,16 While clubfoot can be suspected prenatally, the true diagnosis is not made until after delivery. Because the suspicion of clubfoot can cause substantial parental anxiety, parents who are given information about the possible diagnosis prenatally 2 often have access to prenatal counselling regarding the nature of the diagnosis and treatment options which they appreciate. 3 Some families choose to pursue prenatal counselling while others choose to pursue their own method of obtaining information, such as the internet or discussion with other providers or acquaintances. There also are some families who do not discover the foot anomaly until birth.
This study shows that, when faced with a newborn child with a congenital foot anomaly, the parental anxiety is quite high, regardless of whether or not they received prenatal counselling and information from a paediatric orthopaedic surgeon. We found no difference in the amount of parental anxiety at presentation to the paediatric orthopaedists with a newborn found to have a clubfoot between families who found out prenatally and had prenatal counselling versus those who found out prenatally but did not have prenatal counselling versus those who initially discovered the clubfoot postnatally. This was, admittedly, a surprising result as we felt that those with more prenatal counselling would be less anxious as this was our understanding from having met these families during these encounters. However, a clubfoot diagnosis can be problematic in some children, even when well treated, and an appreciation of the severity and potential implications of the clubfoot diagnosis must be reflected in the increased anxiety seen in all families at initial presentation. Additionally, families who found out about the likely clubfoot prenatally and chose to pursue prenatal counselling may have been, by nature, more anxious than those families who chose to wait until after delivery to meet with the paediatric orthopaedic surgeon. Other authors have reported on how families need to adjust to the loss of their ‘perfect child’ and how this creates some coping difficulty.11,12 We found that many families were concerned about long-term issues of sports participation and possible ongong pain; in addition to treatment with casting and bracing we now address these issues more in the prenatal counselling that we perform. Additionally, most families (93%) chose to seek information from other sources, primarily the internet but also books and other friends or family members.
It is comforting that after meeting postnatally with the paediatric orthopaedic surgeon the levels of anxiety decreased in all families (p < 0.0001). Furthermore, families who met prenatally with the paediatric orthopaedic surgeon reported that the meeting was very informative (median response 7, on a Likert scale of 1 to 7); 83% of those who had prenatal counselling reported they found it very helpful. Other authors have noted decreased anxiety after meeting with physicians for prenatal conditions. In a systemic review, Marokakis et al 14 found that parental anxiety after prenatal counselling significantly decreased after the counselling was given. This review was for a multitude of diagnoses and not just congenital clubfoot.
While this was a prospective study, it nonetheless has some inherent weaknesses. The source of the anxiety was difficult to determine, as these families were concurrently dealing with the difficulties of a newborn which may include the sleep deprivation and anxiety that comes with newly born children. We were not able to control for the baseline anxiety of the families and have this distributed equally across all groups. However, while we did not find a difference in the anxiety levels of families who received prenatal counselling and those who did not, it is unlikely to be a lack of power, as these numbers were really quite similar and extending the study would likely continue to not show a difference. Finally, our Likert scale was limited to a 1 to 7 point scale, and perhaps suffered from ceiling effects that would have been more delineated with a broader scale.
Conclusion
What is already known about this topic?
Discovering a newborn child has congenital anomaly, including clubfoot, can cause considerable parental anxiety that can impact the psychological wellbeing of the mother and father.
Clubfoot is a congenital deformity that is formed early in gestation, and can be suspected prenatally in 60% to 70% of cases, however, the true diagnosis is not made until after delivery.
Prenatal suspicion of clubfoot can cause considerable parental anxiety but parents still appreciate having this information.
What does this study add to this knowledge?
Parental anxiety level is high when faced with a newborn with a foot anomaly, particularly clubfoot.
We found no difference in the levels of parental anxiety between families who discovered the likely clubfoot prenatally and had prenatal counselling (Group A), those who discovered prenatally but did not have prenatal counselling (Group B) and those who discovered the clubfoot postnatally (Group C).
After meeting postnatally with the paediatric orthopaedic surgeon, levels of anxiety decreased in all families of children with clubfoot
While prenatal counselling did not decrease parental anxiety in applicable families, 83% of those who did receive prenatal counselling reported they found it very helpful. Prenatal counselling may not decrease parental anxiety but nonetheless is very appreciated by the families who receive it.
Footnotes
PEM: Statistical analysis and interpretation, Study design, Manuscript preparation.
CJM: Study design, Data acquisition, Manuscript review.
JRK: Study design, Interpretation, Manuscript review.
Pre-visit orthopaedic surgeon questionnaire
We are trying to determine the benefit of prenatal (before birth) counseling on parental anxiety regarding newborn foot anomalies. This will not in any way affect the care of your child, but instead will help us better understand how we can assist you and future parents. Your responses will be kept confidential and your attending physician will not see your answers to these questions. Please fill out this questionnaire as honestly as possible. Thank you.
Immediately post-visit orthopaedic surgeon questionnaire
We are trying to determine the benefit of prenatal (before birth) counseling on parental anxiety regarding newborn foot anomalies. This will not in any way affect the care of your child, but instead will help us better understand how we can assist you and future parents. Your responses will be kept confidential and your attending physician will not see your answers to these questions. Please fill out this questionnaire as honestly as possible. Thank you.