
Abstract
Abstract
Purpose
The aim of the present study was to investigate the functional effects on gait parameters of serial ankle casts for patients with idiopathic toe walking (ITW), in comparison with an unremarkable control group.
Methods
A prospective trial with a pre-test–post-test control group design included ten patients with ITW and ten healthy matched children. Children with ITW underwent serial casting to stretch the plantar flexors, with two 14-day periods with walking plaster casts set at the maximum available ankle dorsiflexion. Both groups were assessed clinically and using a functional gait analysis before and after serial casting, as well as at a six-month follow-up visit.
Results
The normalized plantar heel force increased from 5% pre-interventionally to 79% at the follow-up. The upper ankle-joint angle and the base angle also demonstrated significant changes. Normalized compound action potentials of the medial heads of the gastrocnemius were reduced by 70%. None of these parameters demonstrated any significant differences at the follow-up examination in comparison with the healthy control group. Variations in the displacement of the knee joint on the sagittal plane and of the center of gravity in the transverse plane did not show any significant differences in comparison with the control group.
Conclusion
The reduction of muscle tone and lengthening of the ankle plantar flexors led to persistent increased active ankle dorsiflexion with significant long-term improvement of functional kinematic parameters. No significant difference in the gait analysis was found between the ITW group and healthy children six months after treatment.
Level of Evidence
Level II - Therapeutic
Introduction
Toe walking is a frequent clinical finding in healthy children under the age of three years, and is also a pathological pattern in neuromuscular diseases and structural deformities. 1 The condition is defined as an inability to generate a heel strike during the initial contact phase of the gait cycle, in combination with an absence of full foot contact during the entire standing phase. 2 This is caused by a marked imbalance between the flexor and extensor muscles of the distal lower limb in children with neuromuscular disorders. 2 However, no apparent cause can be identified in 5% of the healthy children. 3 Idiopathic toe walking (ITW) is therefore regarded as a habitual pattern. 4 Transient imbalances in muscle tone, especially in the triceps surae, are thought to play a critical role in the development of ITW. Electromyographic studies have shown pathological innervation patterns in the gastrocnemius–soleus muscle complex, similar to those seen in children with spastic cerebral palsy. 5 If spontaneous correction of the muscular imbalance does not occur, shortening of the plantar muscles with a decreased range of movement (ROM) in the ankle joint becomes structurally manifest and the ITW gait persists.6,7 This leads to severe postural problems that are objectively measurable as a pathological gait pattern.8–12 During adolescence and adulthood, impaired athletic performance can then result in severe social problems for the children affected.
A number of noninvasive and invasive treatment options have been proposed, with the primary aim of increasing the range of ankle dorsiflexion. 2 Treatment strategies include physical therapy, orthopaedic footwear, serial casting, orthoses, botulinum toxin type A (BTX-A) and soft-tissue surgery, depending on the severity of the ITW. However, no consensus has been achieved on the criteria for using a particular type of treatment. In children with mild or moderate ITW, physical therapy alone is sufficient to increase the extensibility of myogenic and fibrous structures through repetitive overstepping of the muscular tension in the shortened plantar muscles. Wearing a day- or night-time orthosis can additionally provide a passive stretching stimulus. Surgical intervention is restricted to children with the most severe equinus contractures. Positive effects have also been reported for serial casting, as well as BTX-A. Although all of these treatments are widely used in clinical practice, the number and quality of publications investigating them is still limited. In a systematic review of the literature, Van Kuijk et al showed that there is preliminary evidence for beneficial effects of serial casting and surgery on passive ankle dorsiflexion, as well as on walking kinetics and kinematics, although normalization does not appear to occur. 2
The purpose of this study was, therefore, to use gait analysis to analyze the ITW pattern after serial casting treatment. The two study objectives were: firstly, to demonstrate improvement in the plantar heel force; and secondly, to describe changes in kinematics and kinetics during gait that occur after serial casting. Pathological ITW parameters after treatment were for the first time compared with the findings in a healthy control group.
Materials and methods
Study design and inclusion/exclusion criteria
In this prospective study, a pre-test–post-test control group design was used, and the study was approved by the local ethics committee (registration number EK 560 220 10). Ten patients who had been diagnosed with an ITW gait and ten children with an unremarkable gait were recruited in the Department of Pediatric Orthopaedics at Dresden University Hospital between June 2010 and September 2012 and were matched for age, sex and body mass index. In our center, ITW is defined as persons walking on their toes with no sign of an upper motor neuron lesion or other neurological problem that could be detected, including no signs of spasticity as evidenced by clonus or increased tone.
The inclusion criteria were: children diagnosed with ITW in a multidisciplinary assessment, for the interventional group; children without walking abnormalities, for the control group; children between the ages of five and 15 years; written informed consent. The exclusion criteria were: children with ITW due to an underlying neuromuscular medical condition; children with walking abnormalities due to malformations of the foot; children with an ITW gait who had undergone previous treatment, including orthosis, serial casting, BTX-A treatment or soft-tissue surgery.
Casting
After written informed consent had been received for the cast treatment and study enrolment, a below-knee cast was applied by a single paediatric orthopaedist (FT) in all of the patients in the ITW group. A stockinette as well as under-cast padding was used to cover both limbs. Fiberglass casting material (Cellacast®Xtra, Lohmann & Rauscher International, Rengsdorf, Germany) was used to apply a walking plaster cast on both sides, with maximum passive dorsiflexion with neutral hindfoot alignment while the children were lying in a prone position with 90° knee flexion. A plaster boot was provided to protect the cast and the children were encouraged to stand and walk. Participation in their usual activities was possible for all of the patients. The casts were changed after 14 days, with reassessment of the passive ankle dorsiflexion range. Casting was stopped in nine of the ten patients after two 14-day applications because the target amount of dorsiflexion, defined as 20°, had been achieved. In one patient, the casting procedure was repeated for a further 14-day period. Applying rigid ankle–foot orthoses at night with 10° dorsiflexion, daily exercises stretching calf muscles and physical therapy prevented renewed deterioration due to increased tightness or shortening of the gastrocnemius–soleus muscle complex.
Investigations
All enrolled participants were assessed pre-interventionally (V1) and post-interventionally after the end of serial casting (V2), as well as at a six-month follow-up visit (V3).
Gait analysis
The ground reaction forces effective under the heels during free walking were measured using instruments for gait analysis. For this purpose, flexible and highly sensitive measurement soles were inserted into the patients’ shoes. Resistive measurements of the distribution of plantar pressure were carried out while the patients walked for a distance of 8 m. The F-Scan in-shoe analysis system (Tekscan Inc., Boston, Massachusetts) was used for the analysis. The spatial resolution of the pressure measurements was 0.5 × 0.5 cm2, with a 50-Hz sampling rate. The data were analyzed using the system's software programme (FastScan, Tekscan Inc.). The effective plantar forces per sensor area in the heel area were added together and the resulting maximum forces on the loading response were then calculated. The maximum forces acting in the ball area during terminal stance were then used for normalization (F_norm). The same shoes were always used for measurement.
Measurements of the angle–time characteristics in the upper ankle joint, as well as between the sole of the foot and the floor, were carried out during free barefoot walking. For this purpose, small infrared markers were attached to the following points on the body: at Nietert's compromise pivot axis/fulcrum member at the knee joint; at the lateral malleolus; at the calcaneus/heel bone at a distance of 0.5 cm from the floor perpendicular to the lateral malleolus; and at metatarsal bone V. Data logging and evaluation were carried out using the AS202 motion analysis system (Steinbichler Austria GmbH, Innsbruck, Austria). On the basis of the angle–time characteristics, the effective angle values in the loading response at the moment of touchdown were measured and used for interpretation.
Stability tests
Variations in the centre of gravity (CoG) on the transverse plane were measured with the patients barefoot, within a time interval of 20 seconds, using an ADDON force plate and associated software (ADDON Elektronik System GmbH, Krailing, Germany). The radii of circles (R_CoG) containing 95% (sd 2%) of the measured data points were evaluated. The displacements of the knee joint on the sagittal plane (dx_knee) were also measured using the same movement analysis system. The double sds of the displacements measured were analyzed.
Kinematic electromyography
The compound action potentials of the medial heads of the left and right gastrocnemius muscles were measured during free barefoot walking with bipolar surface electrodes relative to a reference point. The measurements were made telemetrically over a walking distance of 8 m with the aid of the TeleMyo telemetry system (Noraxon USA Inc., Scottsdale, Arizona). The measured cycles were then rectified, smoothed and normalized relative to the step duration. As a result of the normalization of the action potentials, with mean values during single-leg ball-standing (EMG_Norm), effects on the absolute values among the discrete measurement points (distance and positioning of electrodes, skin conductivity) were eliminated. For this purpose, markers were placed using mouse clicks on the left and right foot touchdowns. The normalized mean values for the compound action potential were evaluated within a time window of 0% to 10% of the step duration. The gastrocnemius muscle shows negligible activity within this time window during physiological walking.
Statistical analysis
SAS version 9.2 (SAS Institute, Cary, North Carolina) was used for all statistical calculations. Pairwise comparisons of all primary and secondary outcome measures and gait parameters were carried out, using nonparametric tests for dependent variables in within-group comparisons and nonparametric tests for independent variables in between-group comparisons. For all statistical tests, significance was set at p < 0.05. As there were no significant differences between the left and right legs in the gait analysis, the average value for both legs was used for analysis.
The primary clinical end-point of the study was defined as intra-individual changes in the normalized plantar heel force between the values measured six months after casting (V3) and the values measured before casting (V1). Nonparametric tests for dependent variables in this within-group comparison were used to compare intra-individual changes in the primary dependent variable between the time points. The alpha level was set at p < 0.05. Parameters are described using medians, quartiles and interquartile ranges (IQRs).
Results
Complete data acquisition was achieved in ten patients diagnosed with an ITW gait and ten children with an unremarkable gait as a healthy control group. The two groups were comparable with regards to anthropometric data (body mass index: p = 1.0; body height: p = 1.0; body weight: p = 0.9). At baseline, the disease group differed significantly in all gait parameters from the control group, except for variation in the CoG. Table 1 summarizes the average values and sd of the absolute values for gait parameters at each measurement time point. Table 2 lists the differences between the findings at V1 and V3. Figure 1 shows the Cohen's d effect sizes; effects were calculated between the time points before serial casting (V1) and six months after serial casting (V3).
Results in the interventional group and control group
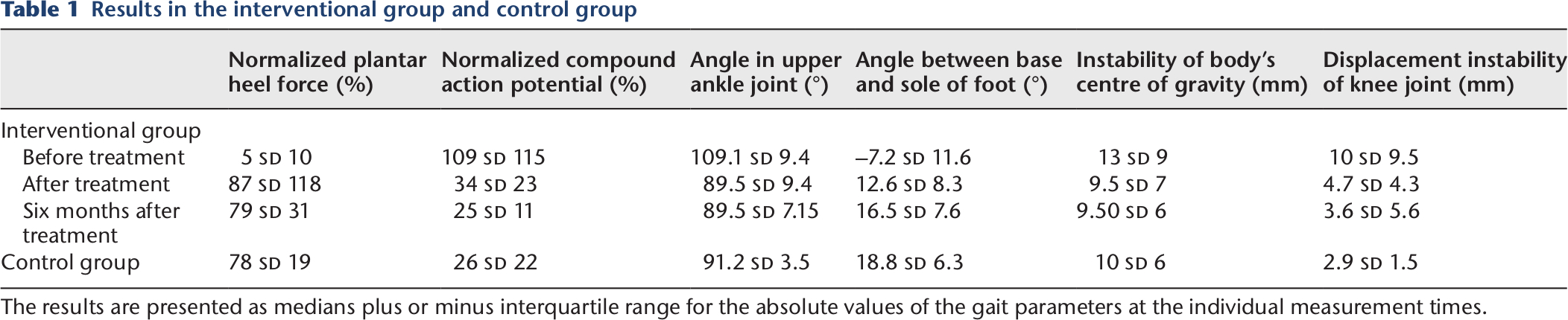
The results are presented as medians plus or minus interquartile range for the absolute values of the gait parameters at the individual measurement times.
Results before and after treatment

Results are presented as medians plus or minus interquartile range for the differences between the time before and after six months of serial casting in the interventional group
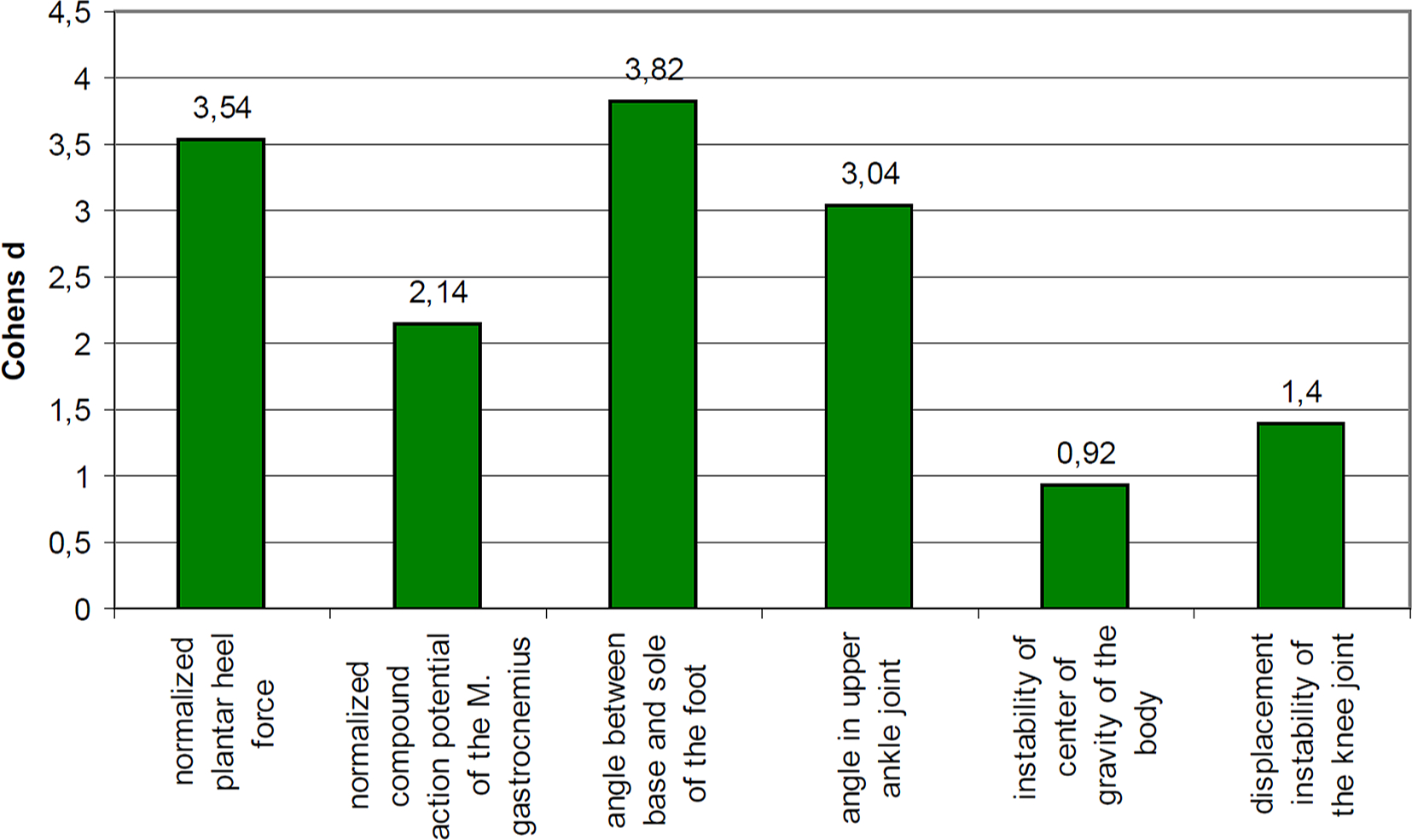
Cohen's d effect size. The effects calculated between the measurement time before serial cast treatment (
Primary clinical end-point
The normalized plantar heel force F_Norm increased significantly from F_Norm = 5% (IQR = 10%) at V1 by 82% (IQR = 124%) to F_Norm = 79% (IQR = 31%) at V3. In comparison with the control group, children with ITW demonstrated a significantly lower F_Norm at V1. After serial casting, this difference was no longer evident at V2 and V3 (Fig. 2).
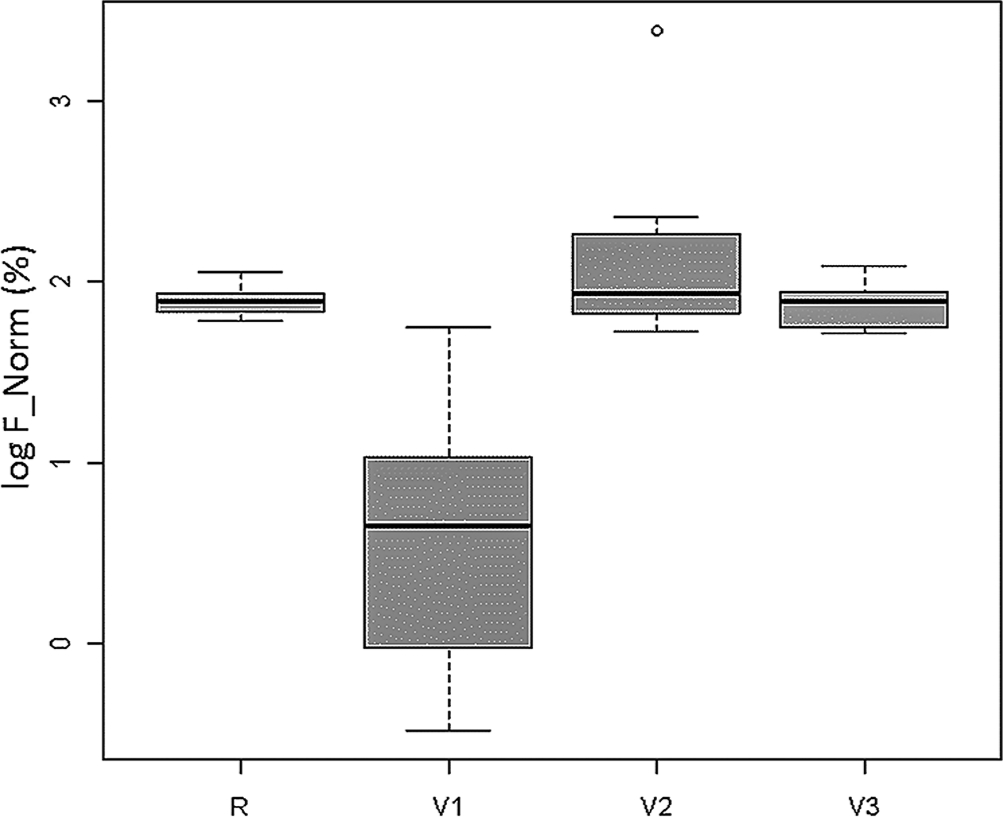
Primary outcome. Box plots with medians, interquartile range and range for the normalized plantar heel force (log F_Norm) in the control group (
Secondary clinical end-points: Kinematic electromyography
Serial casting reduced the normalized compound action potentials of the medial heads of the gastrocnemius significantly from EMG_Norm = 109% (IQR = 115%) at V1 by 70% (IQR = 113%) to EMG_Norm = 25% (IQR = 11%) at V3. EMG_Norm in the healthy control group differed significantly in comparison with the ITW group at V1 (p = 0.0014), but not at V2 or V3 (Fig. 3a).
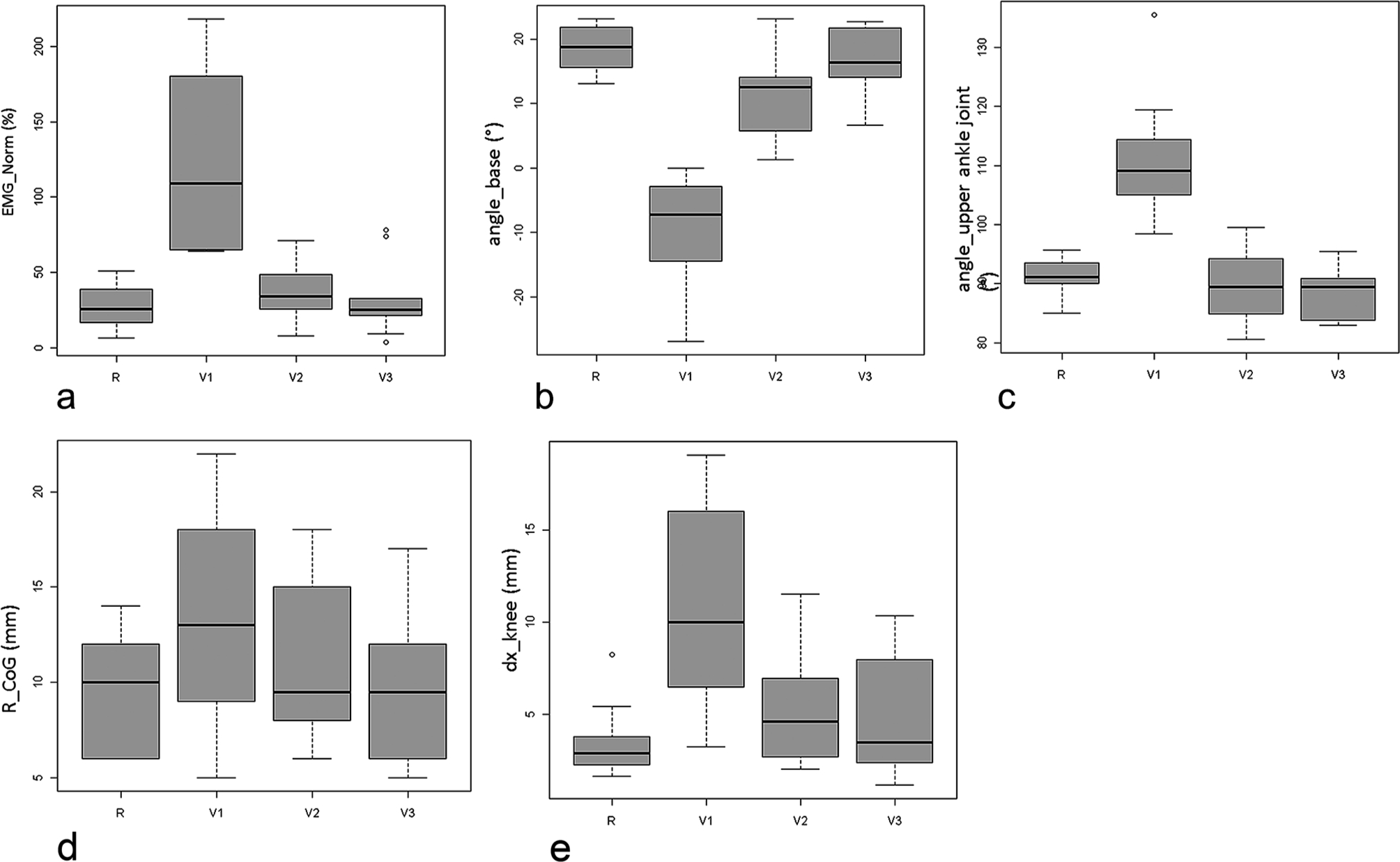
Secondary outcomes. Box plots with medians, interquartile range and range for: a) the normalized compound action potential of the medial head of the gastrocnemius (EMG_Norm);
Secondary clinical end-points: Base angle
The angle between the base and sole of the foot (angle_base) changed by a significant amount, at 22.4° (IQR = 10.5°), from angle_base = –7.2° (IQR = 11.06°) (pes equinus, ball strike) at V1 to angle_base = +16.5° ((IQR = 7.6°) (heel strike) at V3. The base angle differed significantly from the control group at V1 as well as V2, but not at V3 (Fig. 3b).
Secondary clinical end-points: Upper ankle-joint angle (angle_UAJ)
Angle_UAJ also decreased significantly from angle_UAJ = 109.1° (IQR = 9.4°) at V1 by 23.5° (IQR = 8.5°) to angle_UAJ = 89.5° (IQR = 7.2°) at V3. The significant difference in the UAJ angle between the ITW group and the control group disappeared between V1 and V2 (Fig. 3c).
Secondary clinical end-points: Variation in the CoG on the transverse plane
The radii were reduced from R_CoG = 13.0 mm (IQR = 9.0 mm) before the intervention by 3.0 mm (IQR = 7.0 mm) to R_CoG = 9.5 mm (IQR = 6.0 mm) at V3. This difference was not statistically significant. In comparison with the control group, the CoG in the transverse plane did not differ from the reference group at any time point (Fig. 3d).
Secondary clinical end-points: Variation in the displacement of the knee joint on the sagittal plane
The variation in the displacement of the knee joint on the sagittal plane declined significantly from dx_knee = 10.0 mm (IQR = 9.5 mm) before the intervention to dx_knee = 3.6 mm (IQR = 5.6 mm) after treatment. The variation in the displacement of the knee joint on the sagittal plane differed significantly from the ITW group only at V1 (Fig. 3e).
Discussion
This study evaluated the effects of serial casting on plantar heel force and on lower limb kinematics and kinetics during gait in children with ITW in comparison with a healthy control group.
It has been shown that serial casting inhibits overactivity in the ankle plantar flexors.13–20 In addition, the components of the musculotendinous unit are lengthened. These results are achieved by casting the foot and ankle in a neutral position for a period of two weeks. At each change of cast, the ankle is positioned with increased amounts of dorsiflexion, progressively stretching the triceps surae musculature until the desired ROM at the ankle is achieved. Previous studies have observed increased ankle dorsiflexion as well as improved gait after this form of treatment for ITW. 21 However, in an analysis of 226 patients treated in six studies, a literature review by van Bemmel et al 22 reported persistent toe walking after treatment in 52.1% of the children after a weighted mean follow-up period of 3.5 years. Van Kuijk et al 2 also reported that there was no normalization of the ITW gait pattern in comparison with healthy children after successful treatment.
The present study showed that after cast treatment, there was a highly significant improvement in the plantar heel force as well as a reduced action potential in the gastrocnemius, as a sign of reduced stiffness. These results are in agreement with the findings of earlier studies. In contrast to the literature, complete normalization of the ITW gait in comparison with the healthy control group was observed shortly after treatment, as well as at the final follow-up examination. This result is all the more remarkable since most studies in the literature have only included historical data from laboratory databases of healthy control individuals.23–26
A wide range of outcome measurements have been used in ITW studies. 2 Earlier studies mainly relied on maximum passive ankle dorsiflexion, qualitative visual gait observation and electromyography, but more recent studies have used comprehensive gait analysis.24–26 Measuring the passive range of movement (ROM) provides information about the maximum ROM in a joint, but the standardization of the external force used to calculate passive ROM is debatable. 27 Van Bemmel et al 22 described a mean increase in passive ankle dorsiflexion of 3.1° after cast treatment. After a systematic review of literature, Van Kuijk et al 2 also reported impairment of the passive ankle ROM immediately after the end of serial casting lasting until two years in the studies analyzed in their review.23,28–30 However, these results appeared to persist for a relatively short time. 2 Studies included in the review that had longer follow-up periods of between two and 21.3 years did not find any improvement in the passive ankle ROM at the final follow-up examinations.31,32 In the present study, it was decided to assess active ROM as an expression of the functional capacity of the children's joint status. The treatment results also showed a significant improvement in ankle dorsiflexion, which continued up to the final follow-up examination. At this time point, no difference from healthy children was evident.
The literature includes heterogeneous results for other ITW outcome measurements in gait analyses. In a prospectively collected gait analysis with data for 133 children with ITW gaits, Alvarez et al 1 identified only few identifiable and consistent adaptive mechanisms in other joints, particularly the knee joint. Westberry et al 11 found normal knee kinematic profiles in ITW, whereas Armand et al 8 described excessive knee flexion in all three ITW groups. 8 It was unclear whether this finding was either the cause or a consequence of toe walking. 8 The results of the present study show clearly altered sagittal plane findings in comparison with healthy children with a normal gait. As in surgical studies,25,33 the patients in this study showed reduced displacement of the knee joint on the sagittal plane. These results also represented normalization relative to healthy children.
Study limitations
This study has several limitations that need to be taken into account when interpreting the results. Gait analysis entails measurement, analysis and assessment of the biomechanical features associated with walking. 34 This method has previously been shown to provide an accurate and reliable diagnostic tool for differentiating between an ITW gait and a normal gait. 34 However, it is questionable whether gait analysis represents the child's most common walking performance. It is known that children show less toe walking when they know they are being observed, using cognitive compensation, than when they are concentrating in free play situations. 35 It has also been reported that children with ITW may adopt both a toe and a heel contact pattern during the same gait analysis. 2 Observation of toe walking by parents and by physical therapists can supplement a child's walking performance in the normal environment. 2 In their ITW study, Sätilä et al 35 included not only a report from the parents, but also a one-hour evaluation by a researcher as well as blinded-rater evaluation of a 15-minute performance. This approach ensures that different points of view regarding varying ITW performance are evaluated.
A number of studies have carried out quantitative evaluation of toe-walking patterns using gait analysis data. 8 Alvarez et al 1 developed a classification for ITW to differentiate ITW from patients with other conditions, as well as to make it easier to grade the severity of the condition. ITW gait was classified into mild, moderate and severe forms using criteria such as the presence of a first rocker, presence of an early third ankle rocker and predominant early ankle moment. In an evaluation of 133 study participants, these three types demonstrated significant differences with regard to the ankle ROM, sagittal joint power and electromyography evaluation. 1 However, as the ITW patients in the present study did not show any significant differences during gait analysis, classification was not necessary.
Using instrumental gait analysis is also limited to the assessment of comfortable, self-selected walking speeds. 36 Velocity is known to have a significant influence on kinematic parameters. 37 In future studies, various velocities should be tested in order to evaluate this effect. Fanchiang et al 36 have also shown that there are terrain-specific gait patterns with specific characteristics for velocity, cadence and step length.
Conclusion
This study shows that cast treatment has positive effects in ITW patients. For the first time, it was found that ITW treatment leads to complete gait normalization in comparison with a healthy control group. The cast treatment was also well tolerated and was not associated with any side effects.
Footnotes
Acknowledgements
The authors acknowledge support by the Open Access Publication Funds of the SLUB/TU Dresden.
JM, GR: statistical data analysis and creation of graphics.
All authors were actively involved in the interpretation of data and drafting and critical revision of the manuscript. Each author approved the final version to be submitted.