
Abstract
Objective
This systematic review and meta-analysis aimed to evaluate the efficacy of regenerative endodontic procedures compared with conventional root canal treatment procedures in mature permanent teeth with periapical lesions.
Methods
This systematic review and meta-analysis were conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Randomized controlled trials that were included in the study compared regenerative endodontic procedures with traditional root canal treatment procedures in mature permanent teeth with irreversible pulpitis. The Risk of Bias 2 tool was used for quality assessment, and the certainty of the evidence was evaluated using the GRADE approach. Meta-analysis was performed using the RevMan Web software, using odds ratios for dichotomous outcomes and mean differences for continuous outcomes, with a random-effects model applied. Heterogeneity was assessed using the I2 statistic, and publication bias was evaluated using funnel plots and Egger's test.
Results
The analysis included five studies encompassing diverse regenerative strategies. Overall, regenerative endodontic procedures demonstrated comparable or superior clinical and radiographic healing outcomes relative to conventional treatments. Notably, certain regenerative approaches showed greater potential for restoring pulp vitality and reducing early postoperative pain. However, the quality of evidence was moderate, constrained by small sample sizes, methodological heterogeneity, and blinding challenges.
Conclusion
Current evidence suggests that regenerative endodontic procedures are promising alternatives to conventional root canal treatment procedures for mature teeth with periapical lesions. Despite these encouraging findings, further high-quality, multicenter trials with standardized protocols and extended follow-up periods are necessary to confirm the results and establish the long-term benefits and cost-effectiveness of regenerative endodontics.
Keywords
Introduction
Endodontic treatment is critical for preserving the function and structure of teeth affected by pulpal and periapical diseases. Traditionally, root canal treatment procedure (RCTP) has been the gold standard for managing irreversible pulpitis and pulpal necrosis in mature permanent teeth. RCTP is a well-established procedure with predictable clinical success.1,2 However, one major drawback is the loss of pulpal vitality. This loss can impair proprioception and weaken the tooth's structural integrity over time, increasing the risk of fracture.3–5
Regenerative endodontic procedures (REPs) have emerged as a viable alternative treatment for restoring the biological function of the pulp–dentin complex through tissue regeneration. These procedures use a combination of stem cells, scaffold materials, and growth factors to promote pulp tissue revascularization and dentin formation.6,7 Initially introduced for treating immature permanent teeth with open apices, REPs have shown promising results, including continued root development, increased dentin deposition, and improved periapical healing.8,9 More recently, researchers have explored the potential of REPs in mature permanent teeth, with studies suggesting that they facilitate revascularization, partial tissue regeneration, and the recovery of vitality, even in cases with fully formed roots.10,11
Despite advancements in REPs, their clinical effectiveness compared with conventional RCTPs in mature permanent teeth remains a topic of debate. Although REPs have the potential to preserve or restore pulp vitality, specific challenges have been noted, including unpredictable tissue regeneration, risk of root discoloration, and challenges in achieving complete infection control.12,13 Moreover, the long-term success and functional outcomes of REPs compared with traditional RCTPs remain poorly established.14,15
Recent systematic reviews and meta-analyses by El Ashiry et al., 16 Tong et al., 17 and Lin et al. 18 have evaluated REPs versus traditional RCTPs, mainly focusing on immature teeth or mixed samples. However, these reviews show variability in study inclusion and outcome measures, and none specifically focused on mature permanent teeth with periapical pathology. Our review addresses this gap by applying stricter inclusion criteria, using an updated search strategy, and focusing exclusively on mature teeth with periapical lesions to provide more explicit clinical guidance.
As interest in biologically based endodontic therapies grows, a comprehensive evaluation of treatment outcomes is essential. This systematic review and meta-analysis aimed to assess and compare clinical success, periapical healing, long-term functionality, and potential complications associated with REPs and RCTPs in mature permanent teeth, including cases diagnosed with pulp necrosis and irreversible pulpitis and those requiring nonsurgical endodontic retreatment, thereby providing targeted clinical guidance. The findings will provide valuable insights into the existing body of research and support evidence-based decision-making in endodontic treatment planning.
Materials and methodology
Protocol and reporting
The systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1).

PRISMA flow diagram of study selection for systematic review. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Research question
What are the comparative clinical outcomes and success rates of REPs vs. traditional root canal therapy for pulp treatment?
Population (P): Patients with mature permanent teeth requiring endodontic treatment.
Intervention (I): REPs.
Comparison (C): Traditional RCTPs.
Outcome (O): Clinical success rates, periapical healing, functional longevity, and complications.
Inclusion criteria
Peer-reviewed studies published in English; randomized controlled trials (RCTs) directly comparing REPs vs. nonsurgical RCTPs in mature permanent teeth; studies involving mature permanent teeth diagnosed with pulp necrosis, irreversible pulpitis, or requiring nonsurgical retreatment with periapical pathology; studies reporting clinical success rates, periapical healing, tooth survival, long-term outcomes, or pulp vitality; and studies with at least 6 months of follow-up post-treatment.
Exclusion criteria
Non-English articles without accessible full-text translations, case reports, case series, narrative reviews, opinion papers, in vitro studies, and animal studies, studies conducted on immature teeth or nonhuman subjects, studies not directly comparing REPs vs. RCTPs, studies not reporting relevant outcomes (success rates, periapical healing, tooth survival, pulp vitality, or long-term clinical outcomes), studies focusing exclusively on surgical endodontic treatment without nonsurgical comparison.
Databases searched
Databases included are PubMed, Cochrane Library, Scopus, Google Scholar, Dimensions, and Science Direct.
Search strategy
PubMed—(“regenerative endodontics” OR “regenerative endodontic therapy”) AND (“root canal therapy” OR “apexification”) AND (“treatment outcome” OR “success rates”).
Cochrane Library—(“regenerative endodontics” OR “regenerative endodontic therapy”) AND (“traditional root canal therapy” OR “apexification”) AND (“clinical outcomes” OR “success rates”).
Google Scholar—(“regenerative endodontics” OR “regenerative endodontic therapy”) AND (“root canal therapy” OR “apexification”) AND (“treatment outcome” OR “success rates”).
Dimensions—(“Type 2 Diabetes Mellitus” OR “T2DM” OR “Diabetes Mellitus, Type 2”) AND (“Dental Implant” OR “Oral Implant” OR “Osseointegrated Implant”) AND (“Microbiome” OR “Microflora” OR “Microbial Community” OR “Oral Microbiota”).
ScienceDirect—(“regenerative endodontics” OR “regenerative endodontic therapy”) AND (“root canal therapy” OR “apexification”) AND (“treatment outcome” OR “success rates”
Scopus—(TITLE-ABS-KEY (“regenerative endodontics” OR “regenerative endodontic therapy”)) AND (TITLE-ABS-KEY(“root canal therapy” OR apexification)) AND
(TITLE-ABS-KEY(“treatment outcome” OR “success rate” OR “clinical outcome”)).
Identification and selection of studies
The PRISMA flow diagram illustrates the study selection process for the systematic review. Out of 2721 records initially identified, 1987 were removed before screening due to duplicates, ineligibility, or other reasons. After screening 734 records, 57 full-text reports were sought for retrieval, of which 19 could not be accessed. Among the 38 reports assessed for eligibility, 33 were excluded because they included immature teeth, did not use an RCT design, or lacked a direct comparison between REPs and traditional RCTPs. Ultimately, five studies met all inclusion criteria and were included in the qualitative and quantitative synthesis (Table 119–23, Figure 1).
Characteristics of included studies.

CRCT: conventional root canal treatment; EPT: electric pulp testing; LDF: laser Doppler flowmetry; NS-RCR: nonsurgical root canal retreatment; PAI: periapical index; PPP: platelet-poor plasma; PRP: platelet-rich plasma; RCT: randomized controlled trial; REPs: regenerative endodontic procedures; NRS: numerical rating scale.
Data extraction
Data were independently extracted, reviewed, and assessed thoroughly by two authors, and a third reviewer helped resolve any discrepancies between the two data reviewers. A standardized data extraction form was used to collect information on the following: study characteristics (author, year, design, and population size), demographics and clinical details (age, tooth type, and pulp status), interventions (procedure details and materials used), and outcomes (clinical, radiographic, biological, and patient-reported).
Risk of Bias assessment: The Risk of Bias 2 (RoB2) tool, developed by the Cochrane Collaboration, was used with RevMan Web to evaluate the methodological quality of the included RCTs. The assessment categorizes studies as having low risk of bias, unclear risk of bias, or high risk of bias. The assessment consists of the following domains:
Selection bias domain (random sequence generation and allocation concealment): Random sequence generation showed low risk of bias across all studies (100%), indicating proper randomization methods. Allocation concealment was generally low risk but unclear in about ∼25% of the studies, as not all authors provided sufficient details regarding treatment assignment concealment.
Performance bias domain (blinding of participants and personnel): Most studies demonstrated low risk of bias; however, one study had unclear risk (∼20%) due to insufficient reporting of blinding procedures.
Detection bias domain (blinding of outcome assessment): All included studies demonstrated low risk of bias, indicating that outcome assessors were adequately blinded.
Attrition bias domain (incomplete outcome data): No significant dropout or missing data were reported, with all studies assessed as low risk of bias.
Reporting bias domain (selective reporting): All studies were rated as low risk of bias, as all prespecified outcomes were reported.
Other bias: No other sources of bias were identified, and all studies were considered low risk in this domain.
Overall, the methodological quality of the included studies was high, with most domains demonstrating low risk of bias. The primary concerns were related to allocation concealment and performance bias, as a minority of studies lacked sufficient methodological detail in these areas.
Data synthesis
Qualitative synthesis
A narrative synthesis was conducted for studies with high heterogeneity or insufficient data for pooling. Quantitative synthesis: A meta-analysis was performed using the RevMan software when pooling of data was feasible. Effect measures included risk ratios or odds ratios (OR) for categorical outcomes (e.g. success rates), and mean differences or standardized mean differences for continuous outcomes (e.g. pain scores).
Heterogeneity was assessed using Cochran’s Q test and I2 statistic (low: <25%, moderate: 25%–50%, high: >75%). A random-effects model was applied when significant heterogeneity was detected.
Publication bias
Funnel plots and Egger’s test were used to assess publication bias.
Sensitivity analyses were conducted by excluding high-risk studies to assess the robustness of the findings.
Ethical considerations
As this was a secondary analysis of existing literature, no ethical approval was required. This current systematic review was registered in PROSPERO on 1 July 2024 (registration number CRD42024564202).
Reporting
Results were presented in accordance with PRISMA guidelines, including a detailed summary of findings and their implications for clinical practice.
Results
All the included studies were RCTs comparing various REPs with conventional RCTPs in mature teeth exhibiting periapical lesions (Table 1).
Elheeny et al. 19 and Arslan et al. 20 compared traditional REPs with nonsurgical or conventional endodontic treatments, reporting reduced periapical radiolucency and improved pulp sensibility. Jha et al. 21 evaluated the Seal Bio technique—a regenerative method that aims to create a biological seal—and found that it reduced treatment time while achieving comparable clinical healing to obturation techniques. Ahmed et al. 22 assessed platelet-rich plasma (PRP) for revascularization, comparing postoperative pain and lesion healing with standard endodontic treatment. Brizuela et al. 23 used encapsulated human umbilical cord mesenchymal stem cells within a plasma-derived biomaterial. The study assessed outcomes using cone-beam computed tomography (CBCT) and laser Doppler flowmetry (LDF) to monitor lesion size reduction and pulp blood flow changes over time.
Patient characteristics and methodological rigor
The reviewed trials focused on patients with mature permanent teeth diagnosed with irreversible pulpitis. The studies included participants from early adolescence to middle age, ensuring broad clinical applicability. To improve reliability, many studies adhered to established reporting guidelines such as Consolidated Standards of Reporting Trials (CONSORT) and Preferred Reporting Items for RAndomized Trials in Endodontics (PRIRATE). Where possible, blinding techniques were used to reduce bias. In the cell-based trial by Brizuela et al., 23 triple blinding and standardized imaging assessments ensured a high degree of methodological rigor.
Clinical and radiographic outcomes
Radiographic healing
All studies reported a significant reduction in lesion size over time. For instance, Elheeny et al. 19 and Ahmed et al. 22 reported substantial decreases in periapical radiolucency, whereas Brizuela et al. 23 demonstrated measurable lesion reduction on CBCT, with a greater anteroposterior reduction in the REP group. Improvement in pulp sensitivity and vitality was reported as a secondary outcome in several studies. Arslan et al. 20 and Brizuela et al. 23 documented increased responses on thermal and electrical tests during follow-up periods, with Brizuela et al. 23 further quantifying improvements using LDF (Table 2).
Summary of outcomes of the REPs vs. CRCT.

CRCT: conventional root canal treatment; EPT: electric pulp testing; LDF: laser Doppler flowmetry; NS-RCR: nonsurgical root canal retreatment; PAI: periapical index; PRP: platelet-rich plasma; REPs: regenerative endodontic procedures.
Postoperative pain
Although overall pain scores were similar between regenerative and conventional treatments, Ahmed et al. 22 reported that at certain time points (e.g. 12 h post-treatment), the PRP revascularization group had significantly lower pain scores, suggesting a potential benefit in immediate postoperative comfort.
Safety and adverse events
Safety outcomes were consistently favorable across all trials. None of the studies reported severe adverse events such as root fractures or significant inflammatory responses. In Brizuela et al.’s 23 trial, a 12-month follow-up showed 100% tooth survival without significant adverse effects, supporting the safety of cell-based approaches in regenerative endodontics.
Qualitative synthesis and clinical implications
The qualitative analysis revealed that regenerative endodontic approaches—ranging from traditional blood clot induction and PRP revascularization to SealBio and novel cell-based strategies—are feasible alternatives to conventional RCTPs. Key qualitative observations highlight efficacy: most regenerative methods achieve clinical and radiographic healing comparable to conventional treatments, with some techniques (e.g. REPs in the cell-based trial) demonstrating enhanced pulp vitality and a reduction in lesion size (Table 319–23).
Study-specific success rates and healing outcomes.

PAI: periapical index; REPs: regenerative endodontic procedures.
Patient comfort
Although overall postoperative pain is similar between treatment modalities, specific techniques (such as PRP revascularization) may reduce early postoperative discomfort.
Innovation and future directions
Incorporating stem cells and plasma-derived scaffolds (as in the Brizuela et al. 23 trial) represents an exciting frontier in endodontics. These approaches aim not only to resolve periapical pathology but also to promote pulp–dentin regeneration. However, heterogeneity in protocols and outcome measures across studies highlights the need for standardized, long-term trials to consolidate these findings. Overall, qualitative evidence supports regenerative endodontics as a safe and effective alternative to conventional treatments, with the potential to enhance pulp vitality and healing outcomes in mature teeth with periapical lesions.
Assessment of certainty of evidence using GRADE analysis
Risk of bias
The study-wise risk-of-bias assessment for the included trials comparing traditional RCTPs and REPs in mature permanent teeth is summarized in Table 4.19–23 Most studies demonstrated a low risk of bias across all assessed domains. However, the study by Jha et al. 21 showed an unclear risk in randomization, deviations from intended interventions, and overall risk of bias due to limited methodological detail (Figure 2).
Risk‐of‐bias assessment table synthesizing qualitative judgments for the five included studies based on their reported methodology and outcomes.

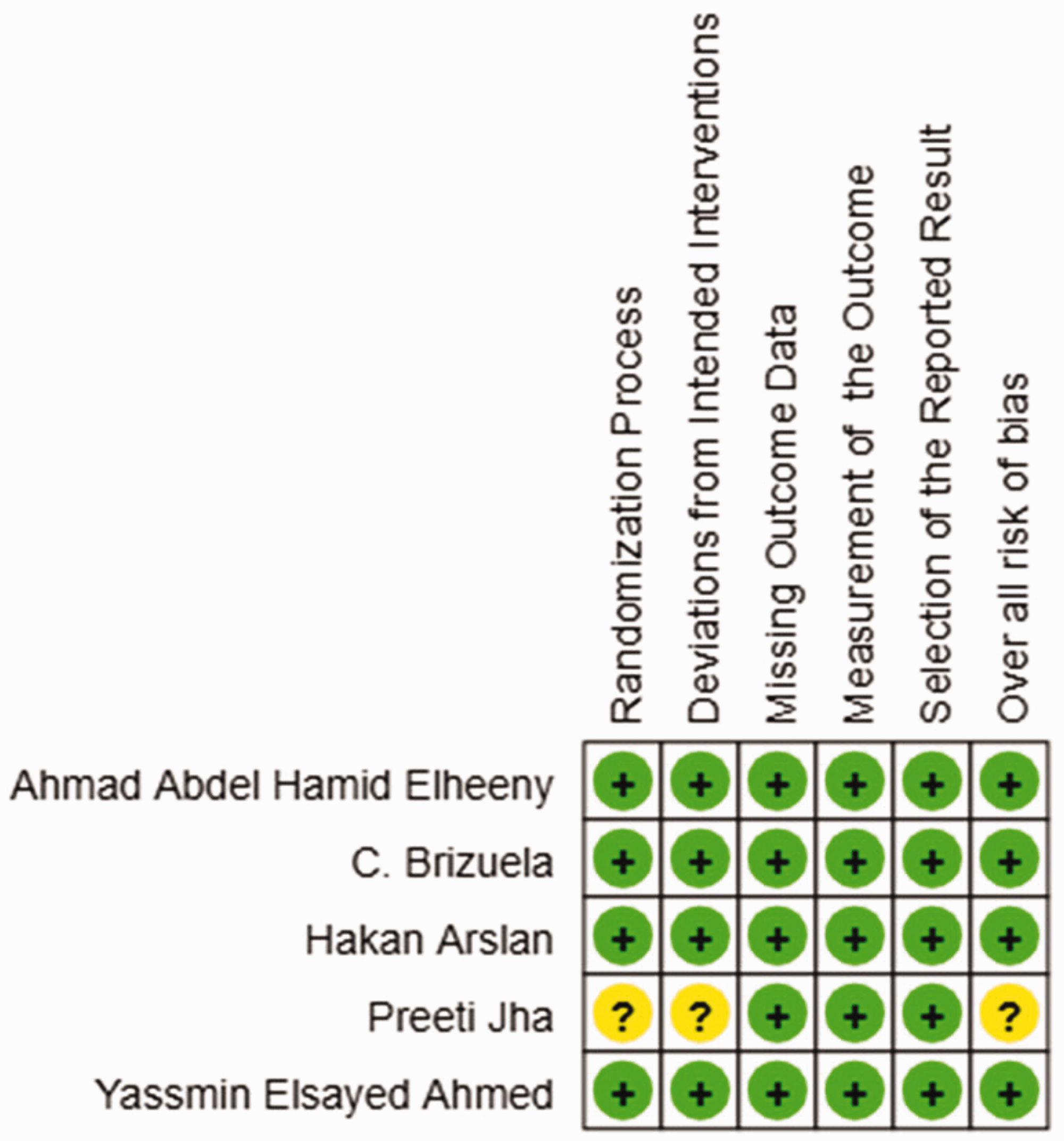
Study-wise risk of bias assessment for studies comparing traditional RCTPs and REPs in mature permanent teeth. RCTP: root canal treatment procedure; REPs: regenerative endodontic procedures.
The risk-of-bias assessment for studies comparing traditional RCTPs and REPs in mature permanent teeth was evaluated using the Risk of Bias 2 (RoB 2) tool. Most domains, including missing outcome data, outcome measurement, and selection of the reported results, showed a low risk of bias. However, some studies showed an unclear risk in randomization and deviations from intended interventions, primarily due to insufficient methodological detail. Overall, the included studies demonstrated a low risk of bias according to the RoB 2 tool, supporting the reliability of the meta-analysis findings (Figure 3).

Overall risk of bias assessment for studies comparing traditional RCTPs and REPs in mature permanent teeth. RCTP: root canal treatment procedure; REPs: regenerative endodontic procedures.
Inconsistency
Across studies, the direction of effect (improvement in radiographic healing, pulp vitality, pain, and tooth survival) was generally consistent, although some variability was observed in the magnitude of effects—particularly for pulp vitality outcomes.
Indirectness
The populations, interventions, and outcomes studied directly addressed the clinical questions regarding regenerative vs. conventional endodontic treatment in mature teeth with periapical lesions; therefore, indirectness was low.
Imprecision
Several studies had modest sample sizes, limiting the precision of effect estimates and raising moderate concerns regarding imprecision across outcomes.
Publication bias
A funnel plot assessing publication bias for studies comparing success rates between traditional RCTPs and REPs in mature permanent teeth showed a symmetrical distribution of studies around the central line, suggesting a low likelihood of publication bias (Figure 4, Table 5).

Funnel plot for publication bias assessment comparing success rates between traditional RCTPs and REPs in mature permanent teeth. RCTP: root canal treatment procedure; REPs: regenerative endodontic procedures.
Publication bias assessment.
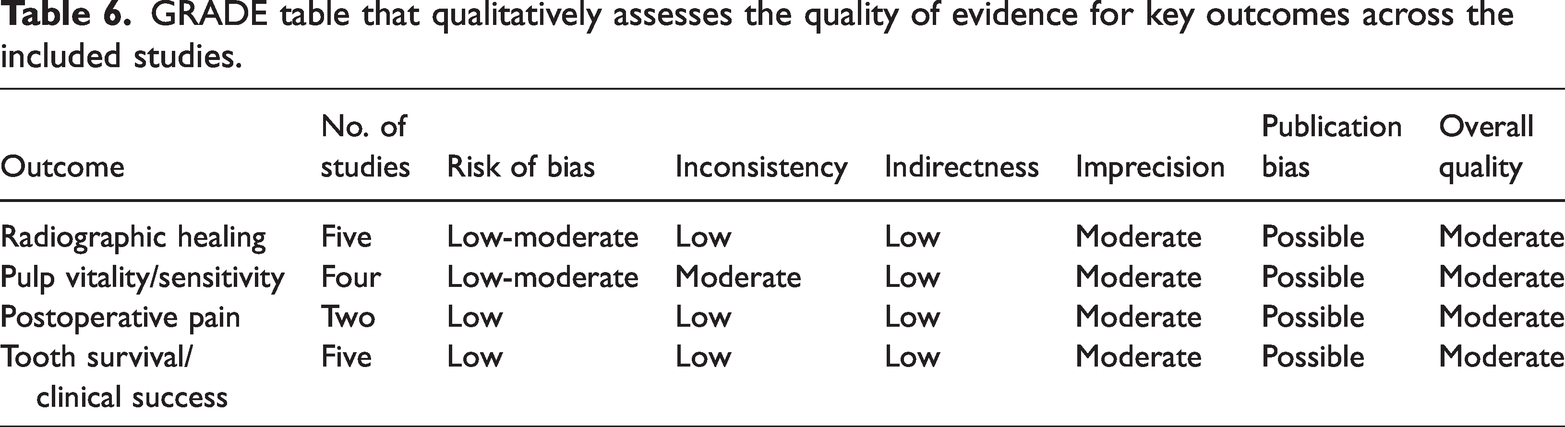
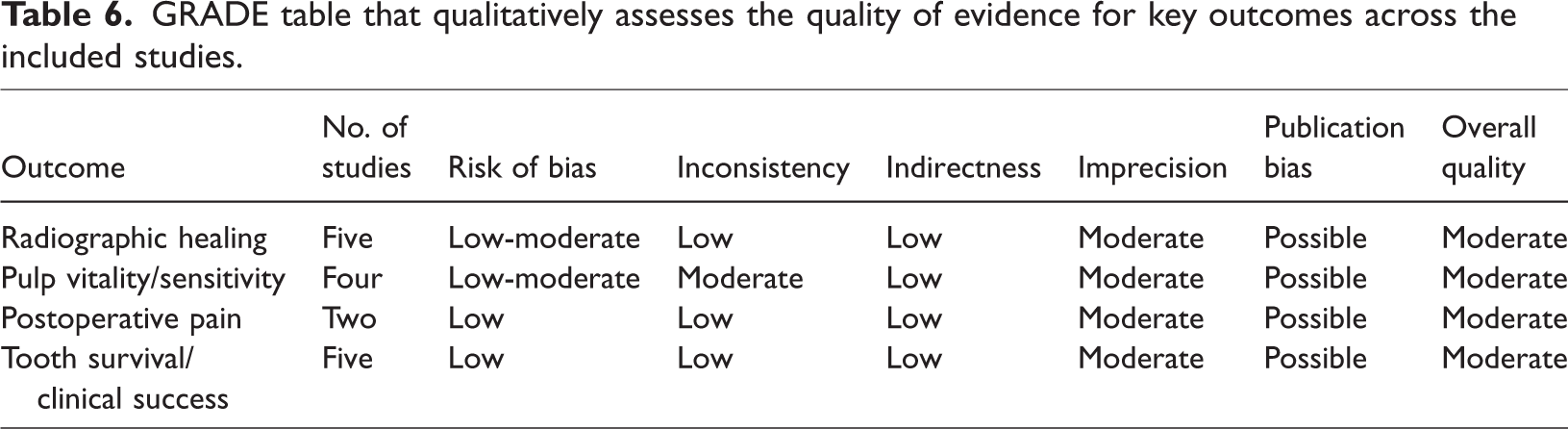
The GRADE assessment indicated that the overall quality of evidence across key outcomes—radiographic healing, pulp vitality, postoperative pain, and tooth survival—was moderate. At the same time, risk of bias and inconsistency were generally low to moderate, but imprecision due to small sample sizes and possible publication bias slightly lowered confidence in the results (Table 6). This suggests that although REPs and traditional RCTPs show comparable effectiveness, further high-quality studies are needed to strengthen the evidence base.
GRADE table that qualitatively assesses the quality of evidence for key outcomes across the included studies.
Quantitative analysis
At 12 months, REPs and traditional RCTPs in mature permanent teeth have demonstrated comparable success rates. The pooled odds ratio was 0.57 (95% CI: 0.26–1.25), indicating no statistically significant difference. Heterogeneity is low (I2 = 0%), suggesting consistent findings across studies (Figure 5).

Forest plot comparing success rates at 12 months between traditional RCTPs and REPs in mature permanent teeth. RCTP: root canal treatment procedure; REPs: regenerative endodontic procedures.
Discussion
This systematic review and meta-analysis synthesized evidence from five RCTs that compared REPs and conventional root canal therapy in mature permanent teeth with periapical lesions. The regenerative techniques assessed included blood clot–based REPs, PRP revascularization, the SealBio technique, and an innovative cell–based approach utilizing encapsulated human umbilical cord mesenchymal stem cells (UC-MSCs) within a platelet-poor plasma (PPP) scaffold. These strategies demonstrated successful clinical and radiographic outcomes, highlighting their potential as viable alternatives to traditional nonsurgical RCTPs.
Although REPs demonstrate potential for periapical healing in mature teeth, the ability to consistently restore pulp vitality remains uncertain and biologically constrained by the fully developed root structure. Elheeny et al. 19 reported 93.9% success at 12 months for REPs, with 55% of teeth in the REP group regaining pulp sensibility. Similarly, Arslan et al. 20 found a higher rate of positive pulp response of 92.3% in REPs, supporting the potential of regenerative techniques to re-establish pulp vitality. These findings align with previous evidence supporting the role of REPs in regenerating the pulp–dentin complex. 21
This review also observed patient-centered outcomes related to postoperative pain. As reported by Ahmed et al., 22 the PRP group reported lower postoperative pain at 12 h. PRP revascularization and conventional nonsurgical RCTPs reduced periapical lesion size. The reduced discomfort can enhance patient satisfaction. Jha et al. 21 reported that the SealBio technique minimized chairside time and provided good healing outcomes comparable to conventional obturation, offering benefits in clinical practice.
All five included studies examined nonvital teeth with periapical lesions. Effective root canal disinfection is challenging due to high microbial loads; however, proper disinfection significantly improves outcomes. In all studies except for Brizuela et al., 23 disinfection followed a two-step protocol: 1%–2.5% sodium hypochlorite irrigation, followed by a final rinse with 17% ethylenediaminetetraacetic acid (EDTA). EDTA as a final rinse solution enhances apical papilla stem cell survival, 24 mitigates sodium hypochlorite’s adverse effects, releases growth factors, and supports cellular differentiation. 24 All four studies except Brizuela et al. 23 examined single-root, single-canaled teeth. The intracanal medicaments varied across studies. Elheeny et al. 19 and Ahmed et al. 22 applied double antibiotic paste; Jha et al. 21 and Arslan et al. 20 used triple antibiotic paste; and Brizuela et al. 23 used calcium hydroxide. Triple antibiotic paste is the preferred choice of intracanal medicament for its potent antimicrobial effects.25–27
Adequate coronal restoration is crucial for determining the outcome of conventional RCTPs and regenerative procedures, as failures are attributed to inadequate coronal seal.27–29 Only Arslan et al. 20 reported the coronal restoration status.
All studies except for Ahmed et al. 22 and Brizuela et al. 23 used blood clot induction as the regenerative endodontic protocol. Ahmed et al. 22 combined PRP scaffolding with induced apical bleeding. Brizuela et al. 23 introduced an innovative cell–based approach using encapsulated UC-MSCs within a PPP scaffold, which significantly improved pulp vitality at the 12-month follow-up. Advanced imaging techniques, including CBCT and LDF, confirmed increased pulp perfusion and reduced periapical lesion. These results align with emerging tissue-engineering strategies for stem cell–based methods in functional pulp tissue regeneration.30,31
Despite promising results, limitations include studies with small sample sizes and heterogeneous regenerative protocols, which affect the precision of outcome estimates. Blinding challenges, particularly across varied treatment methods, may introduce bias in outcome assessments. Publication bias is possible, as studies reporting unfavorable outcomes or negative/inconclusive results may be underrepresented in the literature.
Exclusion of the LILACS database may contribute to potential selection bias. Across all studies, treatment outcomes did not vary according to the intracanal medicament used.
Future research should prioritize the standardization of regenerative endodontic protocols and include larger, multicenter trials with extended follow-up to verify these preliminary findings. Integration of advanced diagnostics, including CBCT and LDF, is essential for accurately assessing tissue regeneration and perfusion. Comparative studies evaluating cost-effectiveness and patient-reported outcomes are needed to determine the overall clinical utility of these regenerative approaches.
Evidence indicates that REPs—via traditional methods, PRP revascularization, SealBio, or innovative cell–based approaches—provide outcomes comparable or superior to conventional RCTPs for mature teeth with periapical lesions. Although the quality of evidence is moderate, these regenerative techniques hold promise for enhancing pulp vitality and overall tooth function, warranting further large-scale investigations.
Conclusion
Current evidence from RCTs indicates that REPs are promising alternatives to conventional RCTPs for managing mature permanent teeth with periapical lesions. Across various regenerative strategies—including traditional blood clot–based methods, PRP-assisted revascularization, the SealBio technique, and innovative cell–based approaches with encapsulated human umbilical cord mesenchymal stem cells—clinical and radiographic outcomes are generally comparable to, and in some cases may even surpass, those achieved using conventional therapy. These regenerative techniques effectively reduce periapical radiolucency in mature teeth. Although some studies report potential pulp vitality responses, their biological significance and consistency in mature teeth remain uncertain and require further validation. High-quality, multicenter trials with standardized protocols and extended follow-up periods are needed to validate these findings further and optimize clinical regenerative endodontic protocols.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deanship of Scientific Research and graduate studies at King Khalid University for supporting this work through Large group Project RGP-2/123/46.
Author contributions
A.M., V.P., S.S., B.S., and M.I.K. conceptualized the study and contributed to the methodology, formal analysis, investigation, and data curation. A.M., V.P., and M.I.K. contributed to writing—original draft and visualization. S.S., B.S., N.A.A., M.A.K., M.A., and M.I.K. contributed to validation, formal analysis, writing—review & editing. A.M. and M.I.K. contributed to supervision and project administration.
Data availability statement
This systematic review was conducted using data from previously published studies that are publicly available through recognized academic databases. No new data were created during this study.
Declarations of conflict of interest
All the authors deny any conflict of interest.
Funding
None.