
Abstract
Abstract
Purpose
Children with multiple hereditary exostoses (MHE) have numerous osteochondromas, with the most prominent lesions typically over the appendicular skeleton. A recent report noted a high rate of intracanal lesions in this patient population and recommended preventative spinal screening with magnetic resonance imaging (MRI) or computed tomography (CT). We sought to evaluate the prevalence of spinal stenosis from intracanal osteochondromas at our pediatric orthopedic center in order to evaluate if routine screening is warranted.
Methods
All pediatric patients treated for MHE were retrospectively identified. Records were reviewed to determine demographics, previous orthopedic surgery, and indication and results of axial spine imaging (CT or MRI). Imaging studies were reviewed to evaluate the presence of intracanal and compressive spinal lesions.
Results
Between 1990 and 2011, axial imaging was performed in nine patients with MHE due to concerns of pain, weakness, and/or dizziness. These patients had moderate disease involvement, with a mean of 4.9 previous orthopedic surgeries to address skeletal osteochondromas. Two patients with MHE had cervical spinal stenosis secondary to intracanal osteochondromas. Both children successfully underwent spinal decompression. Thus, of our MHE population undergoing axial imaging, 22 % were noted to have intracanal lesions.
Conclusions
Our experience reveals a >20 % rate of compressive intracanal osteochondromas in MHE patients undergoing spinal imaging. These two patients represent 5 % of the MHE patients treated at our center. These lesions may be slow growing, and significant consequences can occur if not identified promptly. Thus, we confer that routine axial screening of the spinal canal may be warranted in these children.
Introduction
Multiple hereditary exostoses (MHE) is a skeletal dysplasia resulting in multiple cartilage-capped lesions. It is a genetic disorder inherited in an autosomal dominant fashion with incomplete penetrance in females [1, 2]. Although osteochondromas have a predilection for the metaphyses of long bones, the axial skeleton and vertebral column can also be involved [3–8].
There are numerous published reports of spinal cord impingement and neurologic compromise from intracanal osteochondromas [6, 9]. In most series, patients present with pain, weakness, or other significant neurologic findings [4, 8–23]. Roach et al. found that 12 out of 44 patients screened had lesions encroaching into the spinal canal and, thus, recommended routine magnetic resonance imaging (MRI) or computed tomography (CT) screening of the neuroaxis in patients with MHE to detect compressive lesions prior to the onset of neurologic deficits [6, 9]. However, the prevalence of asymptomatic compressive intracanal lesions in patients with MHE has not been confirmed at other centers [6]. Thus, we undertook a retrospective review to determine the prevalence of intracanal osteochondromas in children with MHE imaged at our center.
Materials and methods
A retrospective chart review was undertaken at a dedicated pediatric orthopedic hospital. The diagnostic registry was searched to identify all patients treated for a diagnosis of MHE between 1990 and 2011. Patients with solitary osteochondromas were excluded from this study, as were patients greater than 20 years of age. Records were reviewed for demographics, previous surgeries, and indication for axial imaging. A search of diagnostic codes yielded 67 possible patients. Of those, 44 were found to have a confirmed diagnosis of MHE. Nine patients had undergone axial imaging. All imaging studies were reviewed to determine the presence of an intracanal osteochondroma, associated neurologic symptoms and physical examination findings, and treatment course. Institutional review board approval was obtained for all aspects of this study.
Results
During the study period, axial imaging was performed in nine patients with MHE for a variety of indications, including back pain, routine screening, leg pain, spasticity, and headache (Table 1). The mean age at the time of scanning was 16.1 years (range 9–20 years). During the study period, the nine patients had undergone a mean of 4.9 orthopedic surgeries (range 2–10) under general anesthesia at our center.
Summary of patients undergoing axial imaging
Two patients with MHE with minimal symptoms were found to have cervical spine stenosis secondary to intracanal osteochondromas. Both children successfully underwent spinal decompression. Thus, of our MHE population, 20.5 % (9 of 44 patients) had symptoms that warranted axial imaging and 4.5 % (2 of 44 patients) were noted to have intracanal lesions.
The first patient was a 15-year-old female with known history of MHE who presented with right hip pain and sudden give-way on her right lower extremity, resulting in frequent falls. She had had multiple previous symptomatic osteochondromas resected from her lower extremities. She had missed a significant amount of school. She had no history of headaches or neck or back pain. On examination, she walked with a stable gait with no limp. She had 3+ knee jerk and ankle jerk, and downgoing toes bilaterally with no clonus. Sensation was intact to light touch throughout. She had 5/5 strength in her bilateral upper and lower extremities. While prone, right hip internal rotation was to 10°, compared to 35° on the left side. External rotation was 60° bilaterally. The patient had no pain with flexion internal rotation on the right hip. Hip flexion was to 120° bilaterally. Pain in the right hip was reproduced with extension and external rotation, with pain radiating down the leg. The spine appeared straight, with no evidence of scoliosis. There were no limitations in cervical, thoracic, or lumbar spine range of motion and no tenderness to palpation throughout her cervical, thoracic, or lumbar spine. Radiographs revealed two large osteochondromas in the right proximal femur, which were thought to be impinging on soft tissues or neurovascular structures. Due to concern about the atypical presentation and her history of MHE, she underwent MRI screening of her entire spine. This revealed several osteochondromas, including a large compressive lesion extending from the lamina at C5. This resulted in significant cord compression, with increased T2 signal on MRI (Fig. 1). She underwent emergent C5–C6 laminectomy. She recovered well with no complications, although her hip symptoms persisted. She underwent surgical hip dislocation with removal of two proximal femoral osteochondromas. She tolerated this procedure well, and her hip and leg symptoms have subsequently resolved.
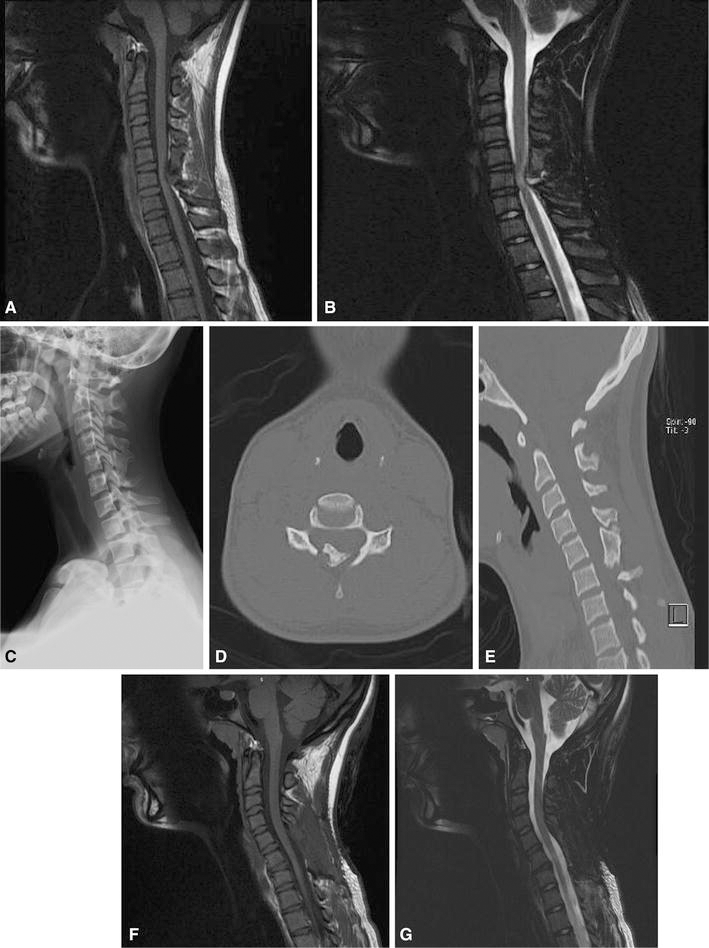
A 15-year-old female with multiple hereditary exostoses (MHE) presented with hip and posterior leg pain. Magnetic resonance imaging (MRI) screening of the entire spine was undertaken, given concern for radicular-type symptoms.
The second patient underwent distal femoral osteotomy at age 15 years. Postoperatively, she complained of headaches. She subsequently did well in her postoperative course. She returned six months later with worsening headaches. The recorded physical examination at that visit was unremarkable, with no evidence of neurologic deficit. CT of her brain was obtained, which was unremarkable. MRI screening of her cervical spine was subsequently obtained, which revealed a compressive lesion at C2 (Fig. 2). She underwent urgent laminectomy with complete resolution of her headaches and no change in her neurologic function.
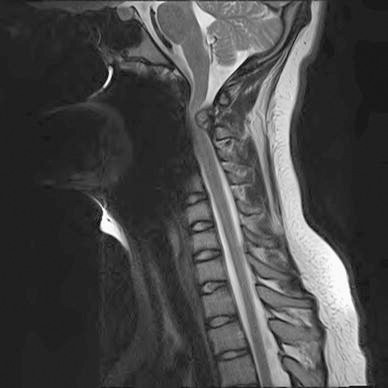
Another 15-year-old female presenting with severe headaches, who initially underwent CT head imaging, which was unremarkable. Eventually, MRI screening was obtained of her cervical spine, revealing a large compressive lesion at C2. She underwent surgical decompression with good relief of her symptoms
Discussion
Osteochondromas are among the most common musculoskeletal tumors. First described in 1814 by Boyer, MHE is due to a mutation in the tumor suppressor genes EXT1 (18q), EXT2 (11p), and EXT3 (19p), which codes for a protein that participates in the biosynthesis of heparan sulfate. In patients with MHE, heparan sulfate stays inside the cell and does not go through the membrane. This causes a disturbance in the negative feedback regulatory system, thus, leading to undifferentiated proliferation of chondrocytes in the metaphyseal region [23–27]. Their composition consists of healthy, lamellar bone and a cartilaginous cap, growing by endochondral bone formation at the metaphysis of long bones [4, 6, 28, 29]. Malignant transformation to a chondrosarcoma has been reported in both the appendicular and axial skeleton, primarily in adults [30–32].
The majority of the vertebral column lesions occur in the cervical (50–80 %) and thoracic (20–36 %) regions, and rarely in the lumbar spine (Table 2). Overall, C2 is the most commonly affected vertebrae [1, 8]. It has been hypothesized that the microtrauma from cervical spine mobility leads to the displacement and subsequent growth of small cartilaginous remains, thus, resulting in a predominance of cervical lesions [5, 7].
Summary of reported spinal osteochondromas in young patients (≤25 years of age)

Extra-canal cervical osteochondromas may present with dysphagia, sleep apnea, or a palpable mass [33–37]. Intracanal lesions may cause pain, paresthesias, myelopathy, weakness, or gait disturbance [4, 6, 8–10, 23]. However, spinal cord compression can be difficult to detect in children. Neurologic findings such as pain or weakness are frequently a late manifestation of cord compression in children [6, 8]. Although spinal lesions tend to progress slowly, they can lead to acute neurological symptoms following minor trauma [5, 6, 8, 38, 39]. In Roach et al.'s series, two of the three patients with symptomatic lesions had permanent neurologic sequelae (presenting with paraplegia and quadriplegia), strengthening the case for screening and aggressive surgical management of asymptomatic lesions [6].
Our series is noteworthy in that the first patient had no symptoms attributable to the cervical spine lesion, and the second patient only had headaches. More concerning, the second patient had headaches following orthopedic surgery, then her symptoms resolved, only to recur 6 month later, finally resulting in a diagnosis. It is possible that hyperextension of the neck at the time of intubation resulted in worsening symptoms due to her C2 spinal stenosis, which, at the time, was undiagnosed. Thus, routine preoperative spinal screening may be warranted for MHE patients in anticipation of neck manipulation during the process of intubation, particularly given the high rate of surgical treatment in this population. According to a recent report, 77 % of children with MHE may be expected to undergo an orthopedic surgery related to their condition [32]. Children with MHE who had had axial imaging had undergone nearly five surgeries on average, typically for the removal of symptomatic osteochondromas or placement of guided growth plates for angular deformity.
In contrast to the rheumatoid population, routine plain radiographs will not necessarily show the pathology [6]. Roach et al. [6] demonstrated that only 17 % of lesions were identifiable on radiographs. Osteochondromas that occur in long bones tend to be pedunculated lesions, while in the spine, these lesions are sessile [4, 29]. Identifying spinal osteochondromas on plain films is difficult due to the complex anatomy of the spine [7]. Thus, axial imaging of MHE children would be required, which is a potentially costly undertaking, particularly if the study were to be obtained in young children who require sedation. Both patients in our series were adolescents. However, the youngest patient in Roach et al.'s series with spinal cord compromise was 5.8 years old, suggesting that imaging is necessary even in young patients.
Roach et al.'s series was remarkable in that they noted that 9 out of 12 patients with lesions penetrating into the canal were asymptomatic. Three of the nine asymptomatic patients underwent prophylactic surgical decompression [6, 9]. Our series adds to these findings, reporting two additional children, one asymptomatic and one complaining only of headaches, who had compressive cervical spine lesions with T2 signal change requiring urgent decompression. It is important for caregivers to be familiar with the potential for spinal stenosis in this patient population, and for providers to have a low threshold for obtaining axial imaging. The primary weakness of our study is that not all 44 MHE patients in our cohort underwent axial imaging. This indicates that the prevalence of compression lesions may be higher than our reported rate of 4.5 % (2 of 44 patients). Given the retrospective nature of this study, we have not yet undertaken routine MRI screening of the neuroaxis in this patient population.
Thus, our series lends further support to routine axial imaging in children with MHE in order to detect compressive lesions and prevent neurologic compromise. Further work remains to determine whether a particular mutation or phenotype holds a greater propensity for large intracanal lesions. This may help refine the indications for screening. For now, we have begun screening all children with MHE at our center at one point during their childhood. Unless symptoms warrant it, screening is typically performed after the child is able to undergo an MRI scan without sedation in order to minimize the risk to the child. We prefer MRI over CT for screening children with MHE. With CT, the osseous center can be clearly visualized, but this often underestimates the size of the lesion. With MRI, the cartilaginous cap of the lesion is clearly visualized. It has been found that MRI and CT are comparable with respect to reliability in detecting an osteochondromas compressing the spinal cord. MRI has a greater advantage in growing children in that there is no radiation exposure, particularly in children with MHE, who have multiple lesions with potential for malignant transformation in adulthood.
In summary, the experience at our center reveals that at least 4.5 % of patients with MHE had compressive osteochondromas (2 of 44 patients). One patient was asymptomatic. Neurologic deficit in similar patients has been reported following minor trauma. Unlike patients with skeletal dysplasia and rheumatoids who undergo preoperative cervical evaluations, neck pathology in MHE patients may not be readily detectible in children with plain imaging. Thus, we confer with the recommendations of Roach et al. for the routine axial screening of these children. Further study is required in order to determine the true prevalence of these lesions and to formalize the indications and frequency of imaging, including preoperative and, potentially, preparticipation sports screening for MHE patients.
Footnotes
Acknowledgments
No external funding was obtained for this study.