
Abstract
Abstract
Purpose
A San Diego pelvic osteotomy is frequently used as part of the surgical treatment of neuromuscular patients with hip displacement. This short-term follow-up study assesses the effectiveness of this osteotomy in patients with closed triradiate cartilage compared with open triradiates.
Methods
Retrospective review of 43 patients (44 hips) with neuromuscular hip disease who underwent a San Diego pelvic osteotomy to correct hip displacement. In all 24 hips had open triradiate cartilage at the time of surgery and 20 hips were closed. Centre edge angle (CEA), acetabular angle (AA) and Reimer's index (RI) were recorded from preoperative, postoperative and the latest follow-up radiographs and statistical analysis was performed.
Results
CEA improved by 39° (7° to 69°) in the open group and 30° (9° to 80°) in the closed group from preoperative radiographs to postoperative, with no significant difference in improvement between groups (p = 0.084). There was no significant difference in AA between the open (improved by 11° (3° to 23°)) and closed (improved by 10° (4° to 21°)) groups (p = 0.65). RI improved from 61% to 11% in the open group and 51% to 12% in the closed group. There was no statistically significant difference between groups in RI at preoperative, immediate postoperative and final follow-up radiographs. At latest follow-up, CEA, AA and RI all remained relatively stable in both groups.
Conclusions
San Diego pelvic osteotomy is equally effective in improving radiographic parameters in neuromuscular patients with both open and closed triradiate cartilage. This study challenges the notion that closed triradiate cartilage is a contraindication to a San Diego pelvic osteotomy.
Level of Evidence
III
Keywords
Introduction
Hip displacement is common in paediatric patients with neuromuscular disorders such as spastic cerebral palsy (CP) and myelomeningocele and can lead to poor sitting balance, pelvic obliquity, scoliosis and difficulty with perineal care. If left untreated, it can progress to complete dislocation of the hip and painful, degenerative arthritis. Natural history studies demonstrate that patients with spastic hip dislocation, if left untreated, develop clinically significant pain in over 50% of patients.1–3 Hip reconstruction in these instances has been shown to be beneficial and usually entails a combination of soft-tissue releases with a femoral and pelvic osteotomy.4–7 The goal of surgical procedures is to achieve a stable, congruent hip with adequate acetabular coverage of the femoral head in order to improve range of movement, prevent or treat pain and improve sitting ability and perineal care.
There are multiple different pelvic osteotomies that have been described for the correction of spastic hip dysplasia and hip displacement depending on the severity and patient factors. The Pemberton osteotomy, 8 the Dega osteotomy 9 and the San Diego osteotomy5,6 have become standard procedures in hip reconstruction of spastic hips. All of these osteotomies have historically been indicated and performed on patients with open triradiate cartilage as they all rely on acetabular hinging on the open triradiate cartilage. Another option for skeletally mature patients with CP includes the Bernese periacetabular osteotomy where the ilium, ischium and pubis are divided, however, this is a more technically challenging procedure and fewer surgeons are comfortable performing this surgery. 10
At our institution, a San Diego incomplete trans-iliac periacetabular osteotomy as was described by Mubarak et al, 5 is performed for patients with neurogenic hip disease who require a pelvic osteotomy. We have been utilizing this procedure in neuromuscular patients with open and closed triradiate cartilages. There is a paucity of literature with regards to incomplete trans-iliac osteotomies in patients with closed tri-radiate cartilage and there is no data comparing this patient group with the skeletally immature patient group for which this procedure was originally indicated.
The goal of this study is to compare the effectiveness of the San Diego acetabuloplasty for patients with closed versus open triradiate cartilage in terms of postoperative change in radiographic parameters as well as after follow-up. We predicted that the degree of correction of dysplasia we could achieve in both groups would be similar postoperatively as well as at later follow-up.
Patients and methods
We retrospectively reviewed the medical records and radiographs of patients ten years or older, who underwent surgical reconstruction for neuromuscular hip displacement that included a pelvic osteotomy between the years 2009 and 2016. All procedures were performed at our institution by the senior author (V.T.S.). The surgical reconstruction consisted of the San Diego type pelvic osteotomy as described by Mubarak et al 5 in 1992 along with appropriate soft-tissue muscle releases and a femoral varus derotational osteotomy (VDRO) stabilized with a fixed angle blade plate.
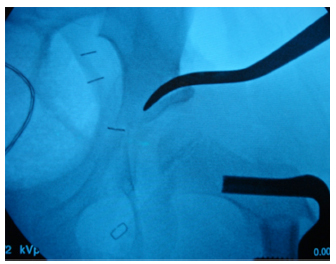
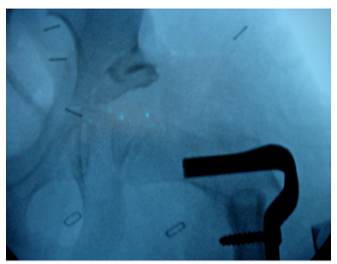
The patients included in the study were divided into two groups. Group one consisted of the ‘open triradiate cartilage’ group at the time of surgery and group two consisted of the ‘closed triradiate cartilage’ group at the time of surgery. Preoperative pelvis radiographs and CT scans, when available, were reviewed to determine whether the triradiate cartilage was open or closed. The patients were then grouped into the appropriate category based on their re-sults (Figs 1 and 2).

Radiographs of representative patient from open triradiate cartilage group: preoperative, immediate postoperative and recent follow-up.
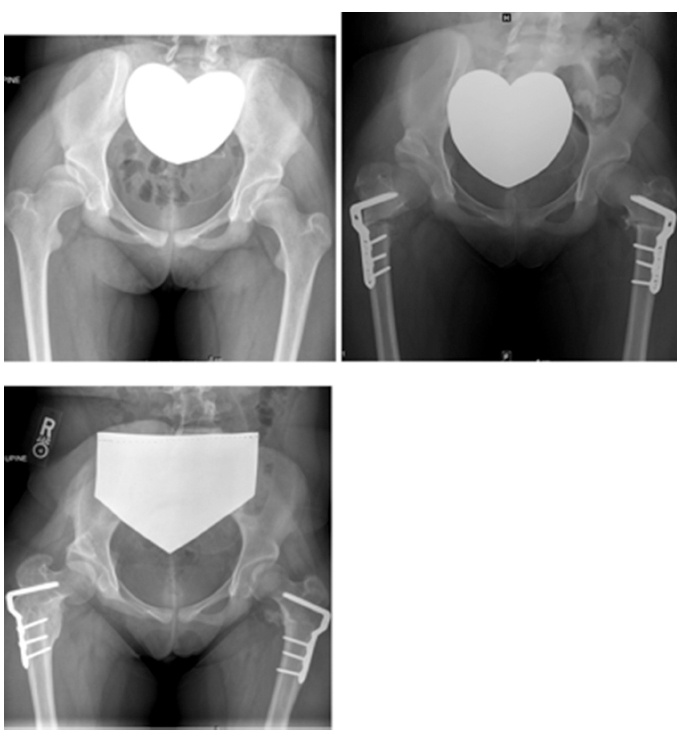
Radiographs of representative patient from closed triradiate cartilage group: preoperative, immediate postoperative and recent follow-up.
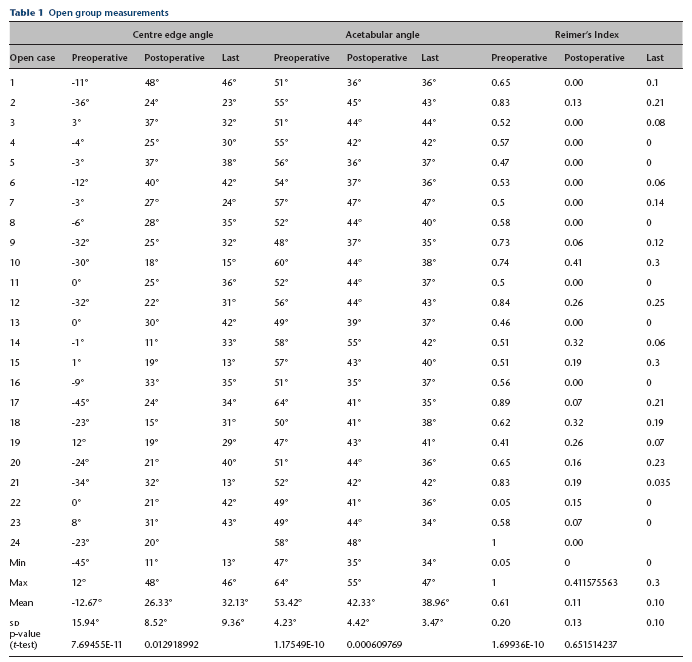
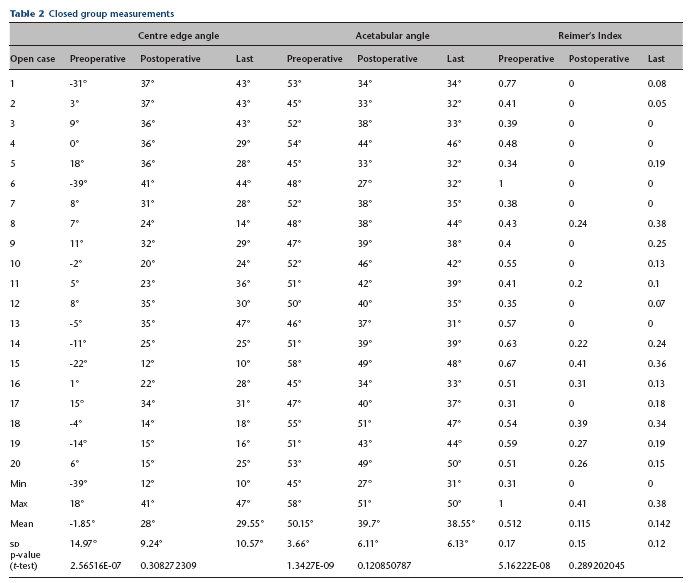
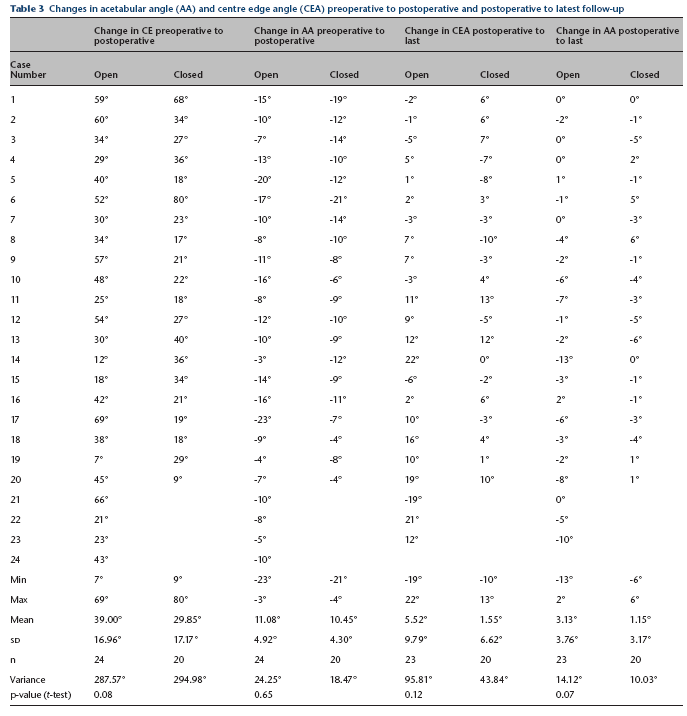
The first author (J.M.), who was not involved in the care of the patients, reviewed the preoperative, immediate postoperative and latest follow-up visit radiographs. The Reimer's migration index, the centre edge angle (CEA) and the acetabular angle (AA) were recorded for both groups (Tables 1 and 2). The AA was defined as the angle formed by a horizontal line connecting both inferior margins of the pelvic teardrop and a line, which extends from the inferior margin of the pelvic tear drop to the acetabular roofs. 11 The CEA and the AA were used to measure the coverage of the femoral head and the Reimer's migration index was recorded to monitor the lateral uncoverage of the femoral head and quantify subluxation/dislocation. The difference in the CEA and AA between the preoperative and immediate postoperative radiographs was also calculated to determine how much improvement the surgery provided (Table 3). The difference between the CEA and AA postoperatively and at last follow-up was also recorded in each group to monitor change over time. The preoperative Reimer's index was compared with the postoperative Reimer's index in both groups and then compared with the latest follow-up to monitor any change. Statistical analysis was performed using the paired t-test within the individual groups and the unpaired t-test when comparing the open group to the closed group.
Open group measurements
Closed group measurements
Changes in acetabular angle (AA) and centre edge angle (CEA) preoperative to postoperative and postoperative to latest follow-up
Surgical technique
The surgical technique consisted of a combined one-stage surgical procedure that included soft-tissue muscle releases as necessary, a bilateral VDRO stabilized with a fixed-angle blade plate, and a San Diego pelvic osteotomy as described by Mubarak et al. 5 Proximal femoral VDRO was performed through a lateral approach to the proximal femur. After this, the anterolateral aspect of the ilium was exposed using a bikini skin incision and the Smith-Peterson interval. 12 A Chandler retractor was placed in the greater sciatic notch. Using intraoperative imaging for guidance, the outer table of the ilium was scored from the anterior inferior iliac spine to the sciatic notch along a line approximately 1 cm above the outer edge of the acetabulum. A bicortical cut was made through the anterior inferior iliac spine anteriorly using an osteotome. Either a straight or a curved osteotome was then used to complete the osteotomy aimed toward the centre of the triradiate cartilage. In cases where the triradiate was closed, the osteotome was aimed toward to triradiate scar. A bicortical cut was then made posteriorly into the sciatic notch using either an osteotomy or a kerrison rongeur. The osteotomy is then opened using a combination of a Chandler retractor and a laminar spreader (Fig. 3). The resected wedge of bone removed from the proximal femur was then reshaped and used as a bone graft (Fig. 4). Internal fixation was not necessary, as the osteotomy remained stable after placement of the cortical bone wedge. Postoperatively, the patient was placed into a total body splint, which was utilized full-time for the first two weeks followed by part-time usage. When appropriate, weight bearing was allowed at six weeks after surgery.
Osteotomy stops short of the triradiate cartilage and is then hinged open laterally to provide coverage for the femoral head.
Bone graft can either be harvested from the anterior superior iliac crest or a wedge of bone from the varus derotational femoral osteotomy can be used in its place. It is then wedged into the osteotomy to provide coverage where needed, most often posteriorly.
Results
We identified 43 patients aged ten years or older who had a reconstructive procedure incorporating a San Diego pelvic osteotomy. Of the 43 patients, 37 had a diagnosis of CP, five had a diagnosis of myelomeningocele, one had a diagnosis of Cornelia de Lange syndrome and one had a diagnosis of traumatic brain injury and resultant spasticity. All patients were included in the study given their hip disease was neuromuscular in nature. The mean time to follow-up after surgical treatment was 25.21 months in the open group (5.4 to 72.4), 20.64 months in the closed group (1.4 to 38.8) and 23.16 months overall (1.4 to 72.4).
The ‘open cartilage’ group consisted of 24 patients. There were 18 male and six female patients with a mean age of 12 years (10 to 15). The ‘closed cartilage’ group consisted of 20 patients (11 male and nine female) with a mean age of 13 years (10 to 20). It should be noted that one patient is included in both ‘open’ and ‘closed’ cartilage group as he was ten years old during his first operation and eventually needed a revision during which point his triradiate was closed. He is excluded for long-term follow-up in the ‘open’ given he underwent a revision procedure and is instead included in the closed group for follow-up of his revision.
Postoperatively, there was an improvement in hip coverage of all patients. In the closed group, the mean Reimer's index improved from 51% to 11% (p < 0.0001). In the open group it improved from 61% to 11% (p < 0.0001).
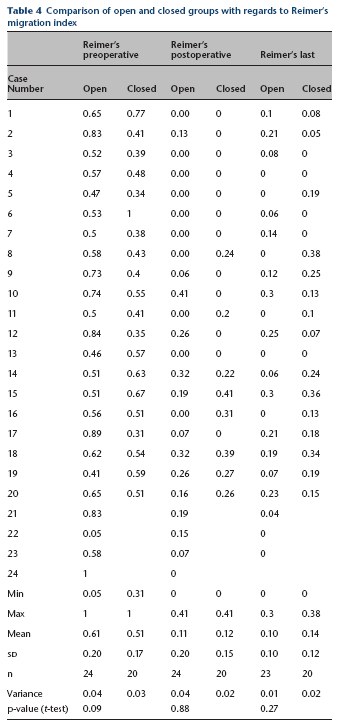
When comparing the open group with the closed group, there was no statistical difference between the preoperative Reimer's index (p = 0.094) and the postoperative Reimer's index (p = 0.875). There was also no statistical difference between the two groups with respect to Reimer's index at the latest follow-up (p = 0.27) (Table 4).
Comparison of open and closed groups with regards to Reimer's migration index
Acetabular shape was improved in both groups postoperatively. The mean preoperative AA in the closed group was 50° (45° to 58°) and 53° (47° to 64°) in the open group. Postoperatively these improved to 40° (27° to 51°) in the closed group and 42° (35° to 55°) in the open group. When comparing the improvement in AA between the two groups (mean of 11° in open group and 10° in closed group), there was no statistically significant difference between the groups (p = 0.65) (Fig 5) (Table 3).
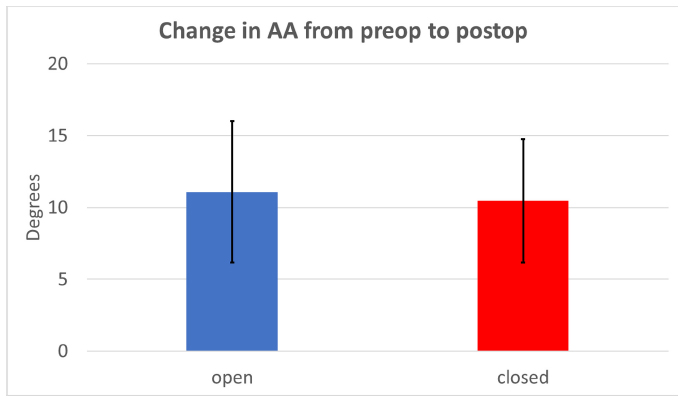
Change in acetabular angle (AA) from preoperative (preop) to postoperative (postop), no statistical difference between the two groups.
The CEA improved in all groups as well. The mean CEA preoperatively was −2° (−39° to 18°) in the closed group and −13° (−45° to 12°) in the open group. Postoperatively the mean CEA was 12° (12° to 41°) in the closed group and 26° (11° to 48°) in the open group. The open group improved by a mean of 39° (7 to 69) while the closed group improved by a mean of 30° (9 to 80), however, these improvements were not statistically significantly different be-tween the two groups (p = 0.084) (Fig. 6) (Table 3).
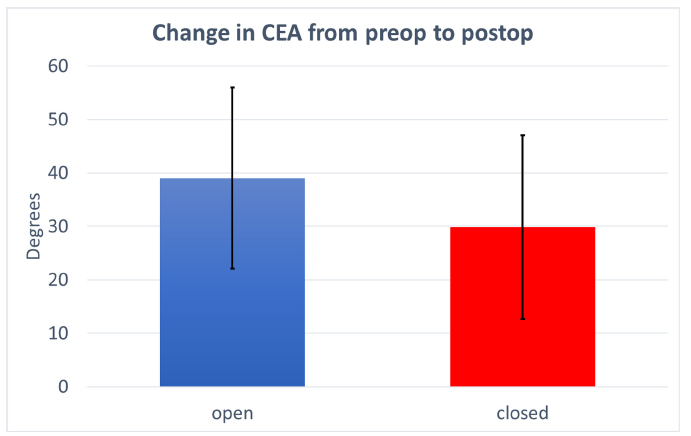
Change in centre edge angle (CEA) from preoperative (preop) to postoperative (postop), no statistical difference between the two groups.
Longer term comparisons between immediate postoperative radiographs and the latest follow-up radiographs demonstrated that the AA changed from 42° to 39° in the open group which was statistically significant (p < 0.05) within this group, however, the clinical relevance of this change was not assessed. In the closed group the AA changed from 40° at immediate postoperative to 39° at last follow-up and this was not a statistically significant change within this group (p = 0.12). When comparing the changes between the two groups, there was not a statistically significant difference (p = 0.68) (Table 3).
With regards to the CEA at long-term follow-up, in the open group the CEA changed from a mean of 26° immediately postoperative (11 to 48) to a mean of 32° at the latest follow-up (13 to 46) (p < 0.05). In the closed group, the CEA changed from a mean of 28° immediately postoperatively (12 to 41) to a mean of 30° at latest postoperative follow-up (10 to 47) (p = 0.31). When comparing the changes between the two groups, there was no statistically significant difference between them (p = 0.12) (Table 3).
The Reimer's index did not significantly change in either of the groups independently between immediate follow-up and latest follow-up (open group p = 0.65, closed group p = 0.29) and there was no significant difference between the groups at immediate postoperative follow-up (p = 0.88) or at latest follow-up (p = 0.27) (Table 4).
Discussion
Hip displacement is common in patients with certain neuromuscular diseases and can lead to pain, poor sitting tolerance and long-term arthritis. The ideal early management of neuromuscular hip dislocation is prevention by surveillance and surgical treatment when appropriate. In such instances a soft-tissue release, femoral osteotomy and pelvic osteotomy may be indicated, and have been shown to have satisfactory results.4,5,13,14 Given that many of these patients are in their adolescence, their triradiate cartilages may or may not remain open at the time of presentation. A closed triradiate cartilage is traditionally held to be a contraindication for a reshaping periacetabular osteotomy. This traditional approach would leave adolescent patients with more technically challenging options such as a Bernese periacetabular osteotomy or a salvage pelvic osteotomy.
Several studies have demonstrated that an incomplete trans-iliac osteotomy has been performed on patients with closed triradiate cartilage with success.15,16 The first mention of an incomplete trans-iliac osteotomy in patients with a closed triradiate cartilage was in 2005 when Roposch and Wedge 17 published their experience with a San Diego type incomplete periacetabular osteotomy in patients with neuromuscular disorders, where in nine of 41 hips, the triradiates were closed. They did not elaborate on this finding but in 2006 Robb and Brunner 15 and Inan et al 16 both published their respective results, performing an incomplete trans-iliac periacetabular osteotomy in patients with closed triradiate cartilage, noting that it is technically feasible and reproducible. In our study, we aimed to see if there was any radiographic difference in patients with and without an open triradiate cartilage who underwent this type of osteotomy.
Our data demonstrates that there is no statistically significant difference in terms of the amount of acetabular coverage or correction we are able to obtain after a San Diego osteotomy when comparing patients with or without open triradiate cartilage. The improvement in CEA and AA in both groups is not statistically significant when comparing them to each other. From preoperative to postoperative, the CEA improves by a mean of 39° in the open group and 30° in the closed group (p = 0.08). The AA improves by a mean of 11° in the open group and 10° in the closed group (p = 0.65). Additionally, we also demonstrate that there is no statistical difference in Reimer's index in both groups at preoperative, immediate postoperative and last follow-up.
Interestingly, the mean CEA in the open triradiate group has a statistically significant increase within the group from the immediate postoperative to the last follow-up radiographs from 26° to 32°. This may be due to the fact that there is more remodelling potential in patients with open triradiates compared with those with closed triradiates, resulting in improved acetabular coverage as the patient ages. Another possible explanation could be that due to changes in the sphericity of the femoral head over time accounting for continued improvement in CEA as proposed by Jóźwiak et al[18]. This trend was not observed in the closed triradiate group as the mean change in CEA from immediate postoperative to last follow-up was only 2°. The rest of our data clearly demonstrates that there is no statistically significant difference between the two groups with regards to changes in the CEA or AA at preoperative, immediate postoperative and at final follow-up, demonstrating that both groups achieve and maintain correction in a similar fashion radiographically.
This study challenges the notion that a closed triradiate cartilage is a contra-indication to performing a San Diego pelvic osteotomy. Two other studies in the past have demonstrated that this type of osteotomy is technically possible in patients with closed triradiate cartilages.15,16 Robb and Brunner 15 noted that the Reimer's index improved in their cohort after an incomplete pelvic osteotomy but made no comparisons with patients with open triradiates. Inan et al 16 further demonstrated that the Reimer's index improved but also added that Sharp's angle is improved; they were also able to provide a painless stable hip for most of their patients. No comparison was made with patients with open triradiates.
It is unclear why the osteotomy works in the closed group, as it does not have an open triradiate cartilage to hinge through. In either group, we did not experience any significant intraoperative complications such as fractures. It has been suggested that patients with CP do have softer and more deformable bone but further research is needed in this area to address this discrepancy. 15 We theorize that patients with neuromuscular diagnoses may have softer bone even in adolescence as they often do not weight bear as much as typically developing patients. Other possible aetiologies may be medication-related, as many of these patients are on seizure medications and other compounding factors that may affect bone health in this patient population. 19 In addition, during the surgical procedure care was taken to ensure completeness of the cuts anteriorly and posteriorly in the sciatic notch in attempt to avoid fracture.
Our study does have limitations. It is a radiographic case control study that does not address the clinical outcomes of the patients. It is also retrospective in nature which comes with its own limitations and possible biases. Additionally, the patient cohort was comprised of patients with heterogeneous underlying diagnoses. We recognize that these disease processes are not the same, however, given that they are all neuromuscular in nature, we do not believe that the disease process itself had an impact on technical ability to perform the surgery or its postoperative radiographic measurements. In addition, the follow-up period was relatively short and may miss some late re-subluxations. Lastly the radiographic measurements were not validated by more than one independent reviewer.
The ability to reshape the acetabulum and provide adequate coverage of the femoral head with an incomplete trans-iliac osteotomy gives providers another tool into their armamentarium when taking care of patients with neuromuscular hip disease who are skeletally mature or approaching skeletal maturity. The San Diego osteotomy is a versatile procedure that can be modified depending on where acetabular coverage is needed by placing the graft more posterior or anterior. Additionally, it is advantageous compared with redirectional osteotomies because it does not provide coverage in one area at the expense of another. It is also technically less demanding than a Bernese periacetabular osteotomy and does not require internal fixation.
In summary, we believe that the San Diego pelvic osteotomy, along with muscle releases and a femoral varus derotational osteotomy, is a powerful tool for the treatment of neuromuscular hip disorders in patients with and without open triradiate cartilage.