
Abstract
Abstract
Purpose
Patients with developmental dysplasia of the hip (DDH) may require a pelvic osteotomy to treat acetabular dysplasia. The Pemberton osteotomy and modified San Diego acetabuloplasty are two options available when surgically treating DDH. The purpose of this study was to compare outcomes following the Pemberton and modified San Diego when treating patients with acetabular dysplasia in typical DDH.
Methods
We included 45 hips in the modified San Diego group and 38 hips in the Pemberton group. Hips with less than two years follow-up and patients with a neuromuscular diagnosis were excluded. Clinical outcomes were rated using the modified McKay criteria with radiographic outcomes graded using the Severin score. Avascular necrosis (AVN) was assessed using the Kalamchi and MacEwen criteria.
Results
Mean follow-up was 4.9 years (2.1 to 11.2). Both procedures produced similar decreases in the acetabular index (modified San Diego: 17.0°
Conclusion
The modified San Diego acetabuloplasty is a safe and effective alternative to treat acetabular dysplasia in patients with typical DDH. By maintaining an intact medial cortex, acetabular reshaping can be customized to address each patient's specific acetabular deficiency
Level of evidence
Level III retrospective comparison
Introduction
Acetabular dysplasia past infancy often requires surgical treatment to increase acetabular coverage and improve hip congruence. 1 The choice of treatment is dependent on patient age. In infants, concentric reduction of the femoral head into the acetabulum, through closed or open reduction, and maintained hip abduction, is generally sufficient to encourage reciprocal remodelling and development of a congruent and well covered hip. In older children, most orthopaedic surgeons agree that treatment with a pelvic osteotomy, with or without a concomitant femoral procedure, is warranted to ensure adequate femoral head coverage.2,3 When successful, this redirects shear forces on cartilage to better tolerated compressive forces, resulting in decreased chondral damage and increased survivability of the hip.
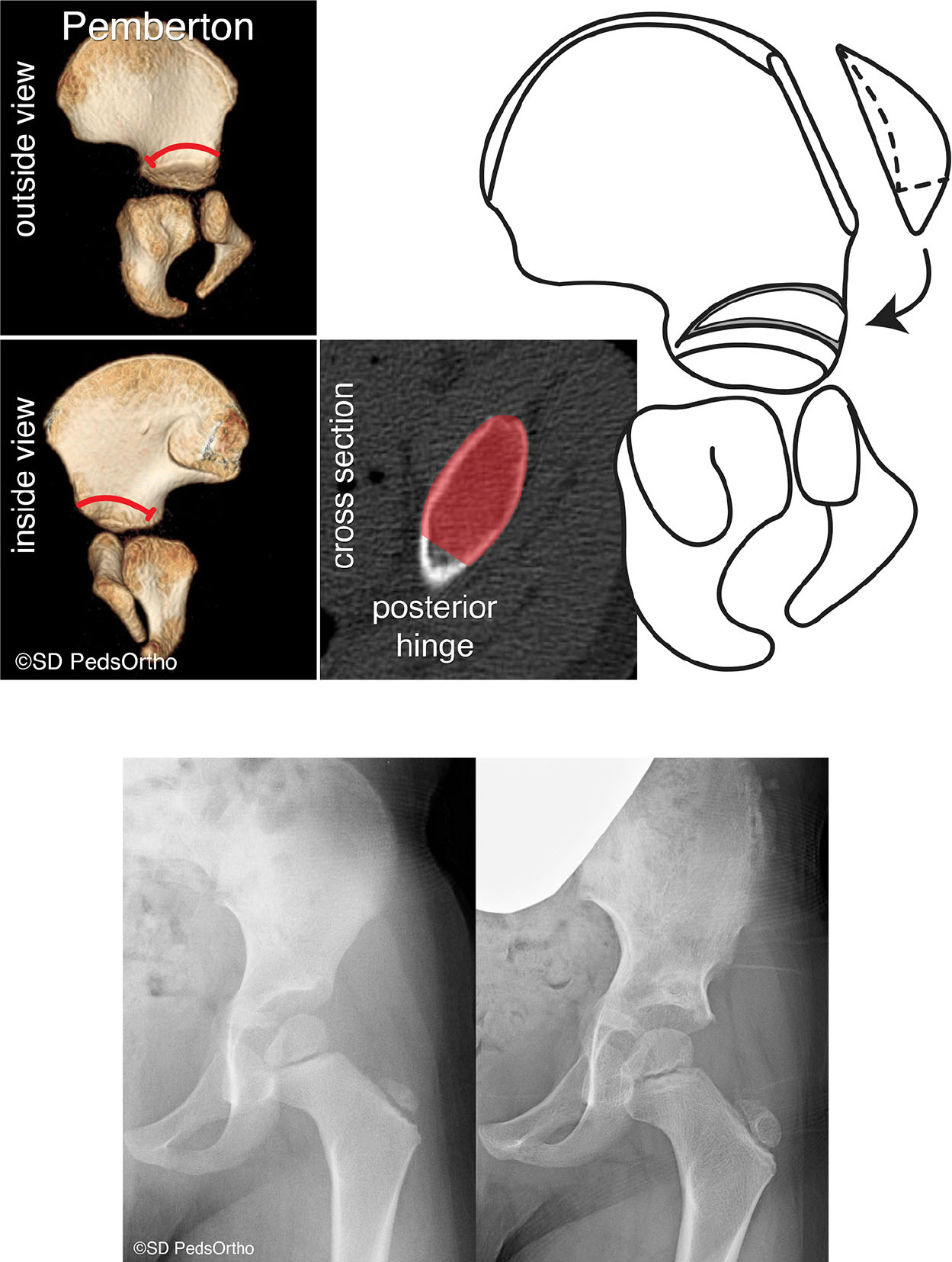
Reshaping osteotomies such as the Pemberton pericapsular osteotomy rely on an open triradiate cartilage hinge and alter the shape of the acetabulum to better cover the femoral head. Specifically, the Pemberton osteotomy uses an incomplete cut through the ilium extending through both the medial and lateral tables of the ilium, and hinges on the posterior limb of the triradiate cartilage to provide increased anterior and lateral coverage4,5 (Fig. 1). The sciatic notch is not cut. The incomplete cut through the ilium maintains inherent stability and does not usually require supplementary internal fixation (in contrast to complete osteotomies such as the Salter innominate osteotomy).
(
The San Diego acetabuloplasty was originally designed to address the acetabular deficiency in patients with hip dysplasia secondary to neuromuscular disease. Early studies identified predominantly posterosuperior or direct lateral undercoverage in these patients,
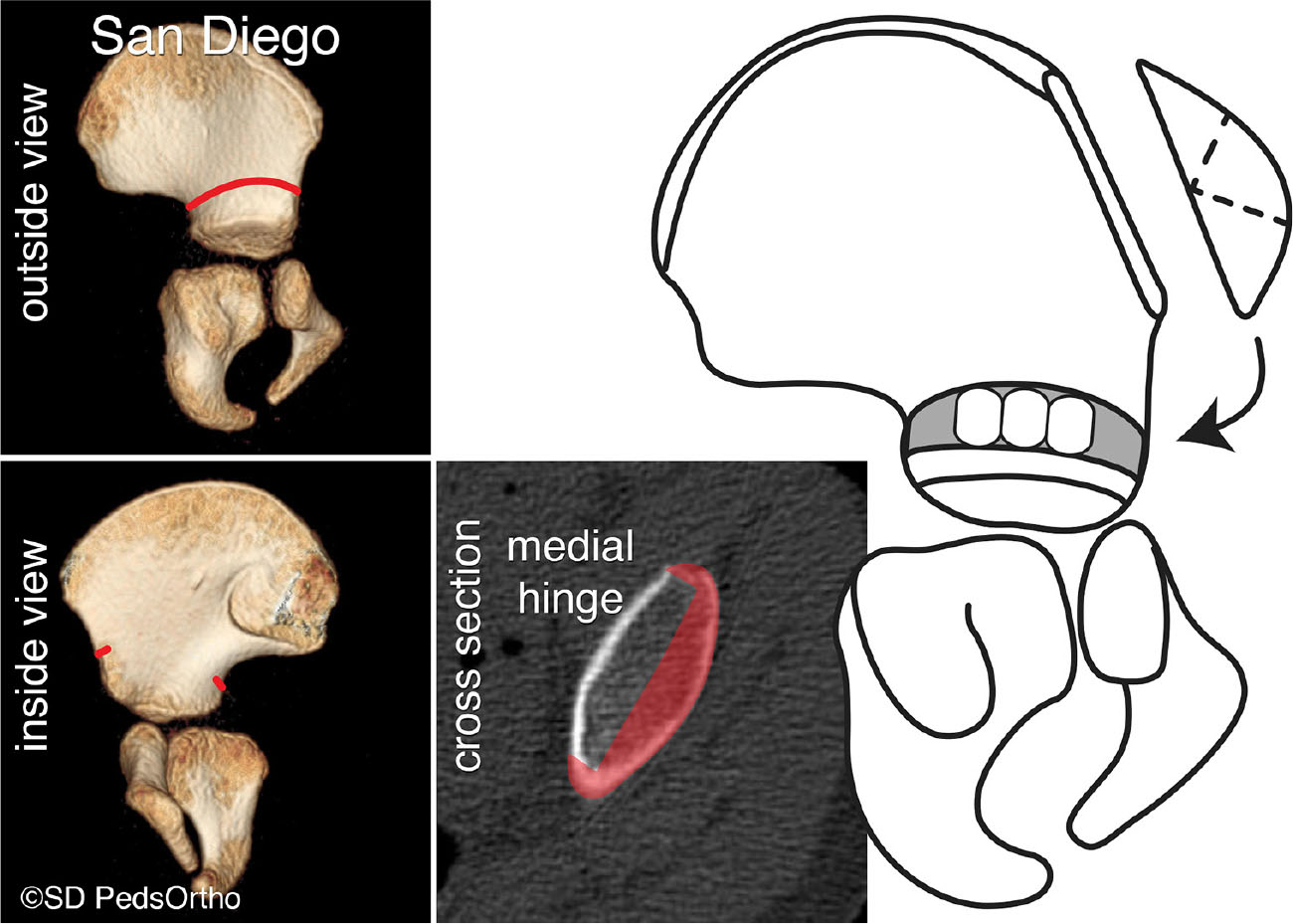
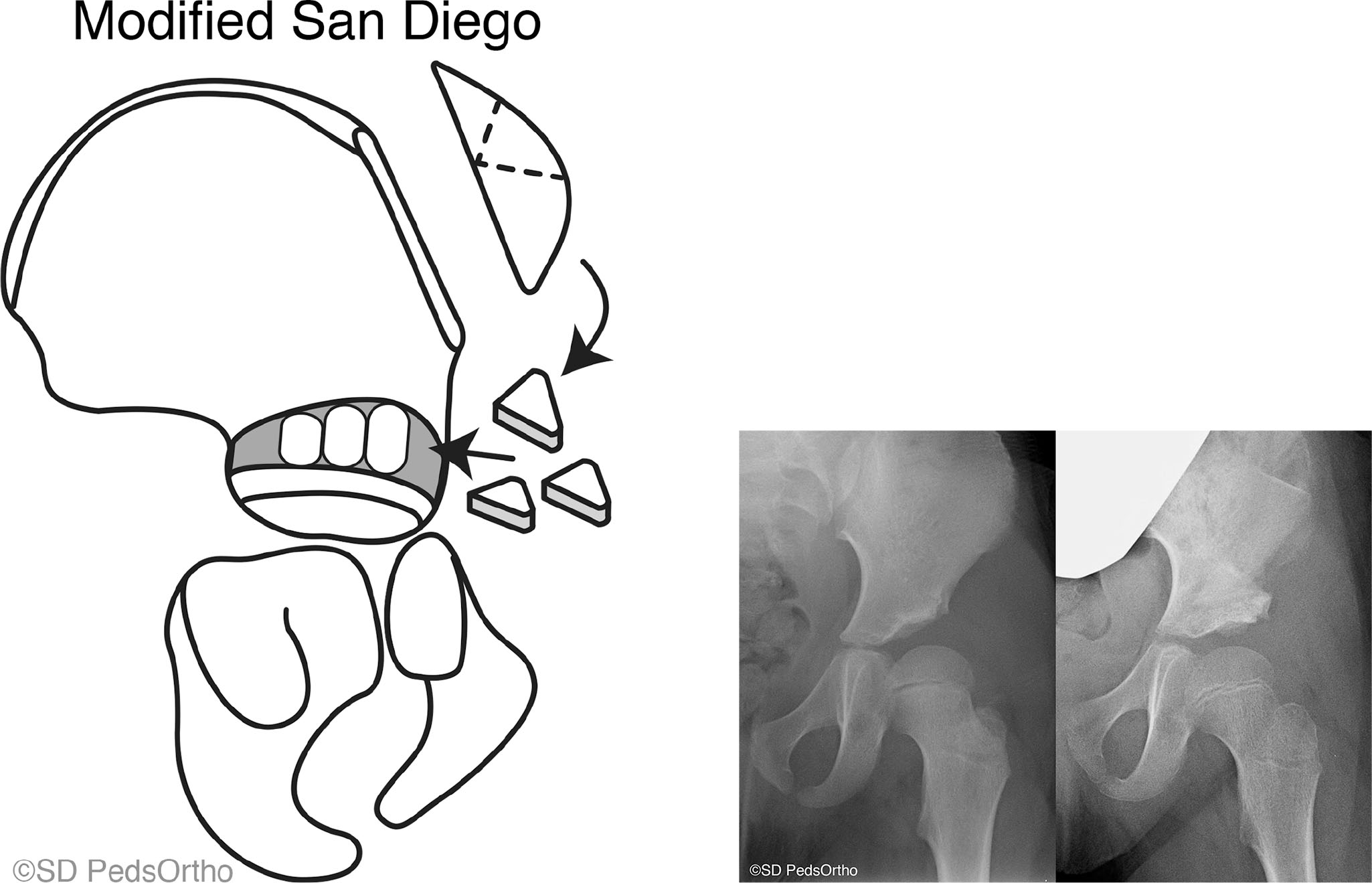
Illustration of the original San Diego acetabuloplasty (designed to treat neuromuscular hip dysplasia – three equally sized triangular bone wedges are used).
Analysis of acetabular morphology using 3D CT scans demonstrates that the acetabular deficiency in developmental hip dysplasia can occasionally be directly lateral, anterior superior or posterior superior, even in children without neuromuscular disease.10,11 We have consequently expanded use of the San Diego acetabuloplasty (Fig. 3) beyond patients with neuromuscular disease, to specifically address the under-covered region in typically developing patients with acetabular dysplasia. We also began to use the modified San Diego acetabuloplasty instead of the Pemberton osteotomy for acetabular dysplasia in typical DDH because we found it easier to conceptualize and teach to orthopaedic staff, residents and fellows.
(
This study aims to retrospectively compare early outcomes between the Pemberton osteotomy and the modified San Diego acetabuloplasty (modified San Diego) performed in children with typical DDH at our institution. In particular, we assessed clinical outcomes, pre- and postoperative radiographic outcomes, as well as complications including the presence of avascular necrosis (AVN).
Materials and methods
After obtaining institutional review board approval, we selected all patients who underwent either a Pemberton or modified San Diego osteotomy for hip dysplasia at our institution between 2006 and 2015. Hips were treated with either the Pemberton or modified San Diego based on surgeon preference. The primary indication for surgery was acetabular dysplasia, which was determined based on a variety of variables including increased acetabular index, decreased lateral centre-edge angle (LCEA), subluxation of the hip or a blunted lateral edge of the acetabulum. Four late presenting hips were dislocated at the time of initial visit and underwent a concomitate open reduction.
Patients were excluded if they had a diagnosis of neuromuscular disease, other concomitant bony procedures in the pelvis or less than two years of follow-up. Overall, 83 hips in 59 patients met these inclusion criteria. Exclusions can be found in Figure 4. Variables studied included age at surgery, recurrent subluxation or dislocations, presence of AVN and return to the operating room. Operative reports were reviewed to identify intraoperative complications. Clinical outcome was measured by the modified McKay criteria. 12 Preoperative, postoperative and final radiographs were assessed and hips were graded using the Severin score. Retroversion was evaluated using the cross-over and ischial spine signs, and acetabular index and lateral centre-edge angle were recorded. AVN, if present, was graded using the Kalamchi and MacEwen criteria. 13
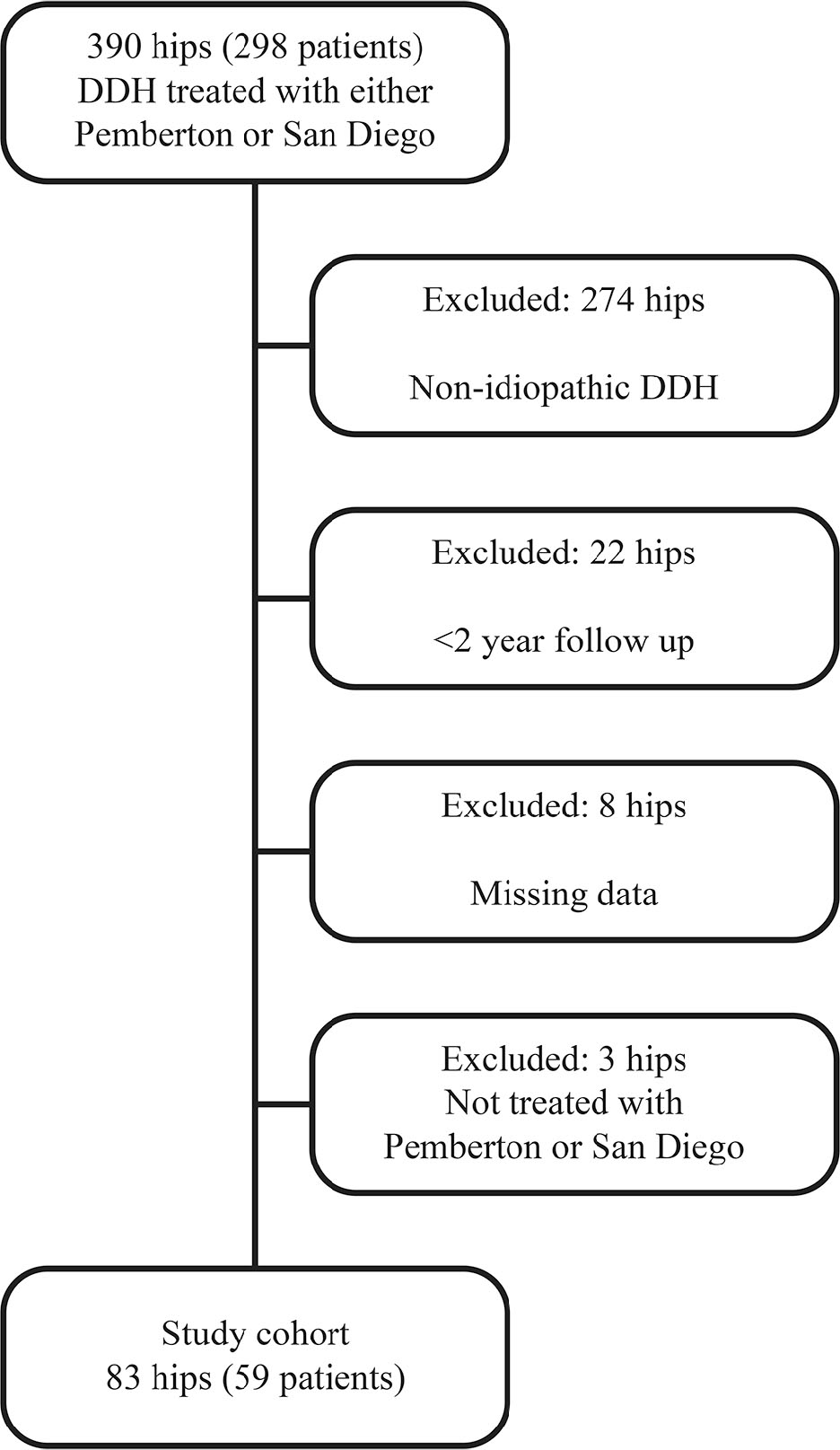
Diagram of our exclusion criteria. Three patients had one hip included and the other hip excluded due to follow-up; one patient had one hip included and the contralateral hip excluded because that side was treated with a surgical procedure that was not a Pemberton acetabuloplasty or San Diego acetabuloplasty (DDH, developmental dysplasia of the hip).
Radiographic measurements were made using the Merge picture and archiving communication system (Merge Healthcare, Chicago, Illinois). The Shapiro-Wilk test of normality and Levene's test of homogeneity of variances was performed on all continuous data. Normally distributed data were analyzed with analysis of variance (ANOVA) and non-normal data were analyzed with the Mann-Whitney test. Categorical data were analyzed with the Pearson chi-squared test or Fisher's exact test. Basic descriptive statistics and odds ratios are reported. No a priori power analysis was performed. Statistical analysis was conducted using SPSS (version 25; IBM, New York, New York) with significance set at a p-value of < 0.05.
Results
Cohort description
In all, 83 hips were included in this study. A total of 55 hips were treated at one or less years of age. Three of these hips were treated with an open reduction at age one year. The remaining 52 hips were treated with a brace; eight of these failed brace treatment and required a closed or open reduction. The remaining 28 hips presented at over one year of age and had an acetabular osteotomy as their initial treatment. Additional cohort characteristics can be found in Table 1.
Cohort characteristics
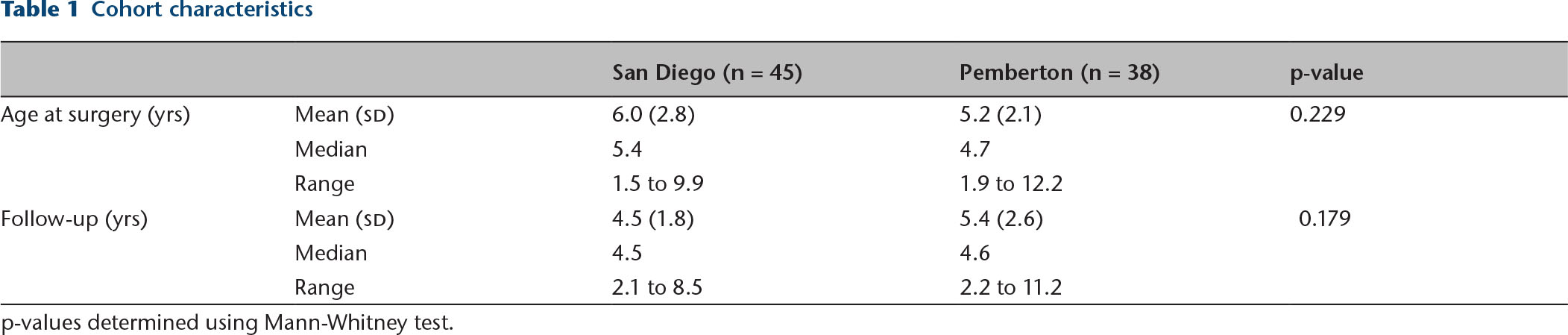
p-values determined using Mann-Whitney test.
There were 32 patients (45 hips) in the modified San Diego group and 29 patients (38 hips) in the Pemberton group. Two patients had a Pemberton on one hip and a modified San Diego on the contralateral hip. Average age at the time of procedure was not different between groups (p = 0.229). Average length of follow-up was 4.9 years (2.1 to 11.2). Four hips (two in the modified San Diego group, two in the Pemberton group) were dislocated at the time of surgery and underwent a concomitate open reduction. Three hips required a revision procedure, two were secondarily treated with a periacetabular osteotomy (PAO) and one was treated with a reverse PAO.
Clinical outcomes
No statistically significant clinical differences were observed between the two groups. In all, 53% of hips treated with the modified San Diego were found to be excellent using the modified McKay criteria, compared with 63% of hips in the Pemberton group. Mild pain was noted in nine hips at the most recent follow-up; seven of these were treated with a modified San Diego acetabuloplasty and two were treated with a Pemberton osteotomy (p = 0.17). There were no subsequent dislocations or subluxations in ether group. Two hips (4.4%) treated with a modified San Diego procedure required a revision acetabuloplasty compared with one hip (2.6%) in the Pemberton group (p = 0.318). Table 2 illustrates the clinical outcomes compared between groups.
Clinical outcomes of interest
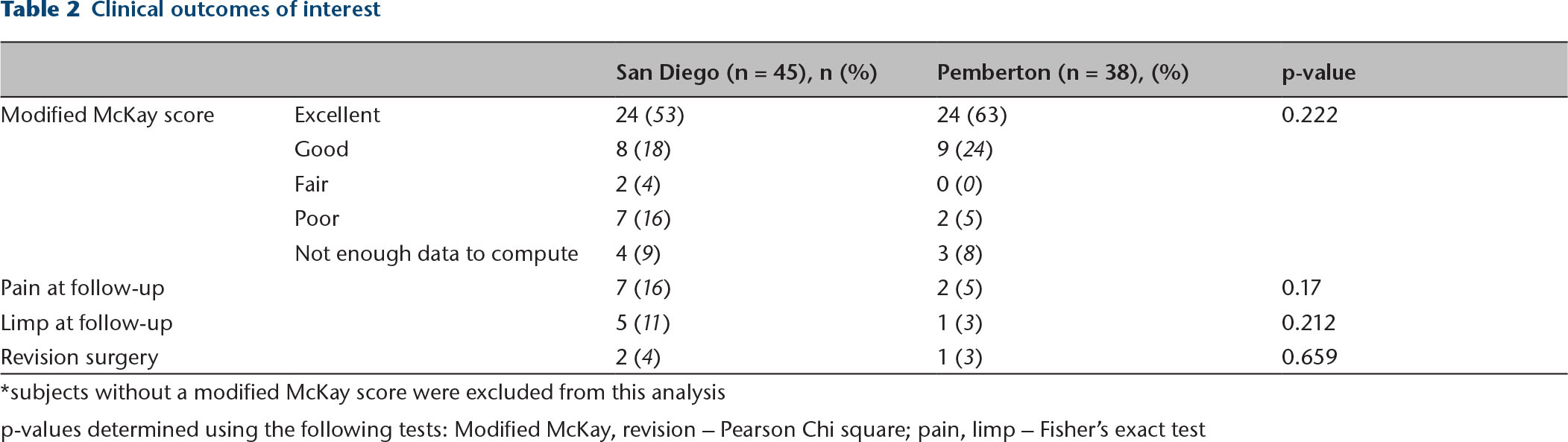
subjects without a modified McKay score were excluded from this analysis
p-values determined using the following tests: Modified McKay, revision – Pearson Chi square; pain, limp – Fisher's exact test
Radiographic outcomes
The primary radiographic outcome was the Severin score. The proportion of hips graded good or excellent on the Severin scale were statistically similar between groups (100% in the modified San Diego
Radiographic outcomes of interest
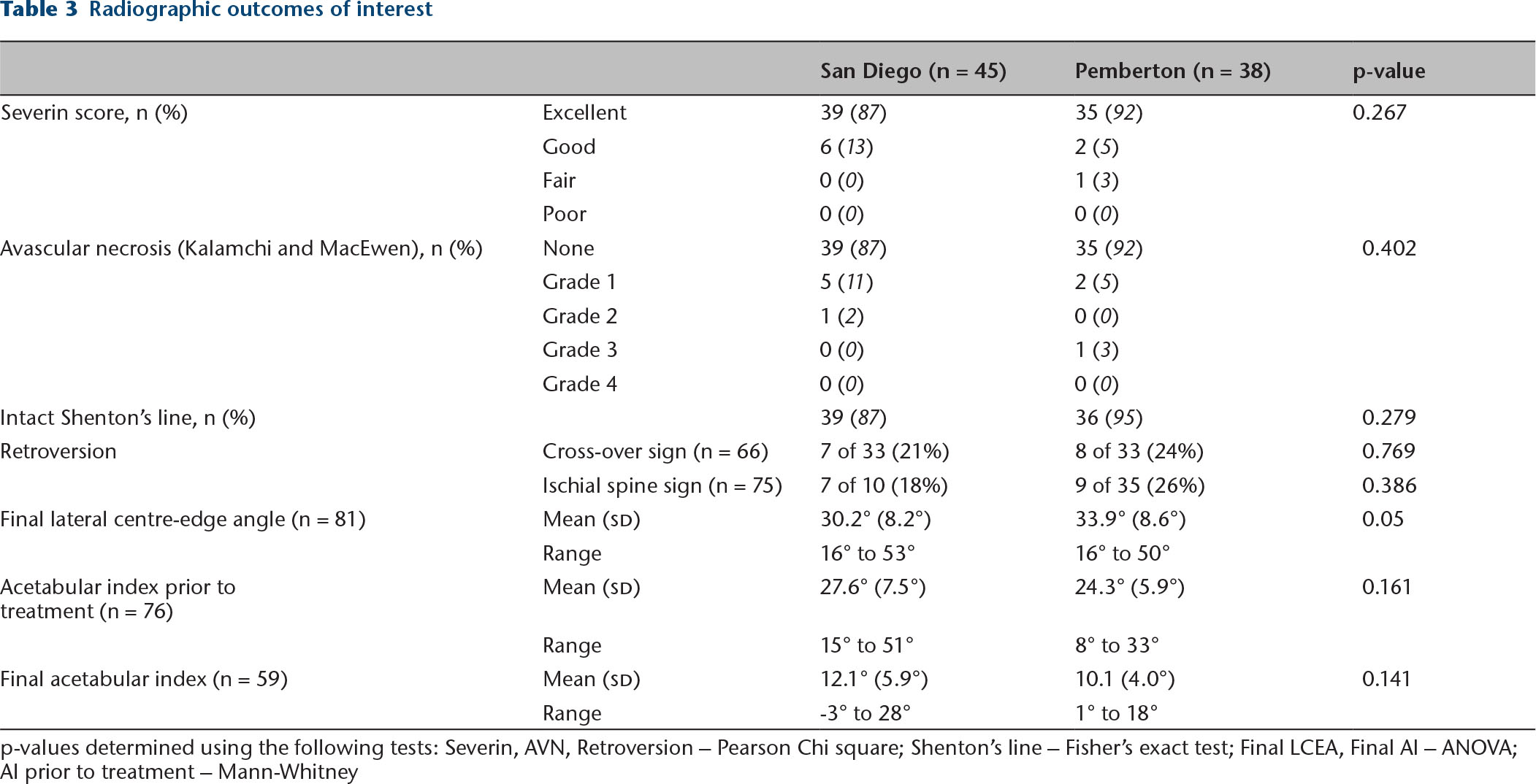
p-values determined using the following tests: Severin, AVN, Retroversion – Pearson Chi square; Shenton's line – Fisher's exact test; Final LCEA, Final AI – ANOVA; AI prior to treatment – Mann-Whitney
Discussion
DDH is the most common paediatric hip disorder, and is best treated in infancy with a Pavlik harness (or other dynamic brace) or closed/open reduction and spica casting. However, either due to delayed presentation or despite early treatment, some patients have acetabular dysplasia after two years of age. 14 Three patients (four hips) in this study were treated with an acetabular osteotomy prior to age two, two hips were dislocated (International Hip Dysplasia Institute (IHDI) grade IV) and two hips were subluxated (IHDI grade II). Lalonde et al 2 demonstrated improved outcomes with surgical treatment of hips in this younger age group, specifically with the Pemberton osteotomy. The Pemberton osteotomy is one of the first described acetabular reshaping osteotomies in North America. Using the posterior wing of the tri-radiate cartilage as a hinge, the osteotomy increases anterolateral coverage. Additionally, as with other reshaping osteotomies, because the cut made through the pelvis is incomplete, implants to stabilize the osteotomy are not usually required. 5 The procedure, with a single triangular bone graft, improved anterolateral coverage. Multiple recent studies have demonstrated good outcomes following the Pemberton osteotomy.15–18
The San Diego acetabuloplasty extends the osteotomy to the sciatic notch, thereby allowing for increased posterior coverage. With this procedure, coverage can be increased in the desired direction by varying the size and placement of the wedging iliac crest bone blocks.8,9,19 The San Diego acetabuloplasty was originally described for use in patients with hip dysplasia secondary to neuromuscular disease, which are typically thought to lack adequate superior-posterior coverage. This is in contrast to hips with typical DDH, which were traditionally thought to primarily lack anterolateral coverage. The San Diego acetabuloplasty is similar to, and often confused with the Dega acetabuloplasty. The Dega goes through the medial and lateral cortex of the ilium stopping short of the sciatic notch while the San Diego goes primarily through the lateral cortex of the ilium and disrupts the medial and lateral cortices at only the anterior inferior iliac spine and sciatic notch. The Dega hinges down anteriorly on an intact sciatic notch and the San Diego hinges laterally through the posterior limb of the tri-radiate cartilage.
Multiple recent studies have demonstrated that the acetabular morphology in patients with typical DDH is more varied than previously thought. Even as early as 1988, Klaue et al 20 used axial CT cuts and found a number of patients with DDH who demonstrated primarily posterolateral undercoverage. Wenger and Kim, 10 using 3D CT scans, found no cases of posterior undercoverage, but a significant proportion of patients with primarily direct lateral deficiency. Anteversion of the acetabulum also varies considerably in patients with DDH. Studies have shown similar average acetabular anteversion in normal hips and hips with DDH, with a wide range of values in both groups.11,21,22 This wide range of anteversion in DDH perhaps reveals why the Pemberton and other osteotomies have been thought to produce acetabular retroversion in some cases.23,24
The modified San Diego osteotomy allows the surgeon to accommodate these variations in acetabular morphology in typical DDH by increasing coverage in the desired direction. Our study demonstrates comparable radiographic outcomes between the two procedures. Both groups had similar degrees of correction, and the majority were rated as excellent on the Severin scale. There was a trend towards superior clinical results in the Pemberton group due to a higher number of patients with reports of mild pain in the modified San Diego group, but this did not reach statistical significance. We did find that subjects reporting mild pain at final follow-up tended to have a higher LCEA at final follow-up. Subjects without pain had a mean LCEA of 31.1° sd 8.2° (16° to 50°) compared with subjects that did report pain who had a mean LCEA of 39.0° sd 9.6° (25° to 53°) (p = 0.021). Rates of AVN were similar between groups, and lower than that recently reported in the literature 25 . Although the Pemberton osteotomy has been suggested as producing acetabular retroversion, this was not borne out in our data.23,24
Advantages to the modified San Diego for typical DDH are:
Because many paediatric orthopaedic surgeons use the San Diego acetabuloplasty to treat dysplastic hips in cerebral palsy, they can apply that experience when using its modified form in typical DDH.
In rare cases, the Pemberton graft is unstable and may require fixation with a Kirschner (K)-wire. This occurred 39% of the time in our series. With the medial wall intact, the modified San Diego may be more stable and pin fixation is not needed. However, the addition of a stabilizing K-wire does not seem to affect clinical or radiographic outcomes.
Finally, understanding the versatility of using different sized triangular grafts allows the experienced surgeon to ‘customize’ acetabular correction in any hip dysplasia case in which advanced imaging studies have localized the location of the most severe acetabular deficiency.
The primary limitation of this study is its retrospective nature. The choice of procedure on individual patients was entirely based on combined decision-making between the surgeon and family. Additionally, the inherent nature of chart review relies on accurate and complete documentation, which sometimes led to missing data points. All surgeries were performed at a single institution but patients were treated by five different surgeons. Differing experience and surgical skill were not accounted for in this analysis. This study is likely underpowered to find a statistically significant difference among our two groups. A
Advanced imaging studies allow orthopaedists to better define each patient's acetabular deficiency in 3D. With more attention being paid to the specific area of acetabular undercoverage, there is a need for acetabular procedures that can be customized to the individual hip. The modified San Diego osteotomy affords the surgeon increased flexibility in reshaping the acetabulum to address the specific deficits. Future studies are necessary to identify the patients best suited for this type of correction based on preoperative imaging, and to describe long-term outcomes from the procedure.
Footnotes
JDB: contributed to data acquisition, data analysis, and the drafting and critical revision of the manuscript.
DRW: contributed to the design of the study, interpretation of data, and critical revision of the manuscript.
SJM: contributed to the design of the study, interpretation of data, and critical revision of the manuscript.
VVU: contributed to the design of the study, interpretation of data, and the drafting and critical revision of the manuscript.