
Abstract
Purpose
Data on the benefits of perioperative prophylactic antibiotics in the paediatric population are lacking. In this study, we aimed to assess the rate of infection after isolated soft-tissue procedures in patients with cerebral palsy with and without preoperative prophylactic antibiotics between 2009 and 2015.
Methods
We reviewed the records of all children with cerebral palsy who underwent isolated soft-tissue procedures (on the upper and lower limb) at our hospital between 2009 and 2015. Children with at least 30-day postoperative follow-up were included. Children who had groin incisions were excluded.
Results
Two groups were identified: the antibiotic group (77 children with 203 incisions and 343 procedures) had one surgical site infection; the no-antibiotic group (48 children with 102 incisions and 177 procedures) had no surgical site infections.
Conclusion
These results suggest that the use of preoperative antibiotics does not change the rate of postoperative surgical site infections.
Level of Evidence
Level III therapeutic study
Introduction
Perioperative prophylactic antibiotics have been shown to confer numerous benefits for patients undergoing relatively major operations. 1 However, many of the guidelines calling for use of prophylactic antibiotics have been extrapolated from adult spine, joint arthroplasty and trauma literature.2,3 Paediatric data are sparse 4 and include minimally invasive procedures with Kirschner (K)-wire percutaneous pinning. 5 In children with cerebral palsy (CP), the role of prophylactic antibiotics in preventing infections following soft-tissue procedures has not been reported, although these procedures are frequently performed in children with CP. 6
This study aimed to assess the rate of infection after isolated soft-tissue procedures in children with CP. We hypothesized that the incidence of surgical site infections (superficial and deep) would not be different with or without preoperative antibiotics for isolated soft-tissue procedures in these children.
Methods
After obtaining the approval of our Institutional Review Board, we reviewed the records of all children with CP who underwent isolated soft-tissue procedures (on the upper and lower limbs) at our hospital between 2009 and 2015. Children with at least 30-day postoperative follow-up were included.
Excluded surgeries were soft-tissue procedures with groin incisions (adductor and psoas lengthening), soft-tissue procedures associated with any bony procedure (osteotomy, anchors, K-wires or cortical hole drilling) and soft-tissue procedures associated with implants like baclofen pumps or any other non-orthopaedic procedures. Patients who were on antibiotic treatment at the time of surgery were excluded. Patients who had risk factors for surgical site infections, such as diabetes, chronic lung diseases, gastrostomy or tracheostomy were also excluded. These patients were excluded since there was no control group of patients who had groin incisions or had gastrostomy tubes and did not receive preoperative antibiotics.
Clinical data included the Gross Motor Functional Classification System (GMFCS), 7 preoperative use of prophylactic antibiotics, type of prophylactic antibiotic used, number of surgical incisions per patient and number of procedures per patient. Superficial and deep surgical site infections were defined as any infection occurring within 30 days postoperatively, following the previously reported criteria. 8 In our retrospective cohort study, the procedures were performed by the CP team at our hospital, which includes four surgeons. Patients were retrospectively divided into two groups: children who had preoperative antibiotics and those who did not. Infection rate was compared between the groups. All decisions to use antibiotics were based mainly on the surgeon's experience.
Results
A total of 125 children with CP had isolated soft-tissue procedures. A total of 305 incisions (292 lower extremities and 13 upper extremities) and 520 procedures were identified (Tables 1 to 3). There were 402 excluded patients who had groin incisions for adductor lengthening procedures during the study period. All patients who had groin incisions received preoperative antibiotics and were excluded from the study.
Demographics, antibiotic use and infection rate
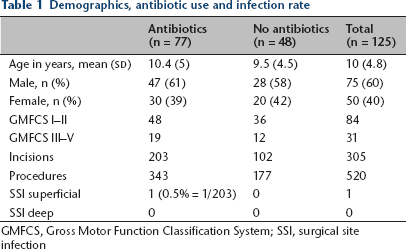
GMFCS, Gross Motor Function Classification System; SSI, surgical site infection
Procedures performed in lower extremities in children with cerebral palsy without bone procedures
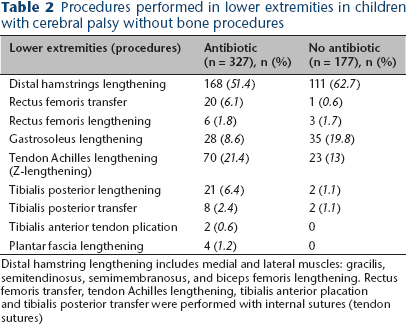
Distal hamstring lengthening includes medial and lateral muscles: gracilis, semitendinosus, semimembranosus, and biceps femoris lengthening. Rectus femoris transfer, tendon Achilles lengthening, tibialis anterior placation and tibialis posterior transfer were performed with internal sutures (tendon sutures)
Procedures performed in upper extremities in children with cerebral palsy without bone procedures
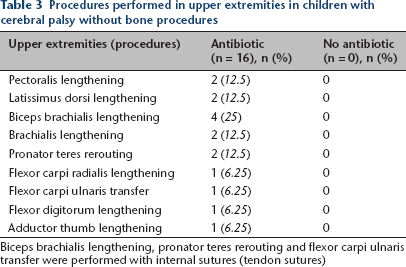
Biceps brachialis lengthening, pronator teres rerouting and flexor carpi ulnaris transfer were performed with internal sutures (tendon sutures)
The first group (children who had antibiotics) included 77 children with 203 incisions and 343 procedures. Cefazolin was used for 76 children, and clindamycin was used for one child. Only one child (GMFCS II) presented with superficial surgical site infection, and the diagnosis was made clinically seven days after the procedure. In this case, there was mild erythema and tenderness around the wound. Oral cephalexin was used for ten days, and no further treatment was needed. Mean hospital stay for this group was one day (sd one day).
The second group (children who did not have antibiotics) included 48 children with 102 incisions and 177 procedures. In this group, seven children had a history of allergy to antibiotics. No surgical site infection was noted in this group. Similar to that of the first group, the mean hospital stay was one day (sd one day).
Discussion
The majority of surgical site infections following orthopaedic procedures are caused by contamination of the surgical site with naturally occurring skin flora – primarily Staphylococcus aureus and Staphylococcus epidermidis.2,9 Therefore, antimicrobial prophylaxis with drugs such as cefazolin that acts against these organisms has been accepted as effective practice for surgical site infection prevention.2,9 However, development of multi-resistant infections remains a risk with the use of wide spectrum antibiotics. Therefore, this study discusses the need to strive for minimizing the use of preoperative antibiotics. Moreover, the type and spectrum of the antibiotic used needs further investigation to reach a balance between the necessary antibacterial coverage and the risk of developing resistant organisms.
Recent studies in the paediatric population have shown no increased incidence of infection when antibiotics were not used before percutaneous pinning of supracondylar distal humerus fractures.10,11 Bashyal et al 10 found a 0.9% infection rate in a review of 459 children who did not have preoperative antibiotics and a 1.2% infection rate in 163 children who had antibiotics before humeral supracondylar percutaneous pinning. Similarly, Iobst et al 11 found a 0% infection rate in a review of 304 children with supracondylar pinning.
In a review of minimally invasive soft-tissue procedures, Formaini et al 5 found one infection in 1243 children who did not have antibiotic prophylaxis. Tosti et al, 12 in a multicentre study including adult hand soft-tissue procedures, found a 0.77% infection rate in 388 patients without using preoperative antibiotics and a 0.47% infection rate in 212 patients who had prophylactic antibiotics. Our results, showing a 0% infection rate in 102 surgical sites for 48 children with CP who had isolated soft-tissue procedures, support these previous findings.
The limitations of our study included its retrospective nature and the small number of patients. However, many patients were excluded during our review to avoid the impact of factors other than the soft-tissue procedure on the infection rate and the decision of antibiotic prophylaxis.
This study suggests that for children with CP who undergo isolated soft-tissue procedures without groin incisions, preoperative antibiotics do not change the rate of postoperative surgical site infections. These procedures are safe when performed under the standards of antiseptic care. While this study excluded patients with CP who had comorbidities such as gastrostomy, further research is needed to investigate the effect of CP comorbidities on infection following soft-tissue procedures. Further studies are also needed to investigate the role of preoperative antibiotics in different procedures performed for children and adults with different conditions.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
None declared