
Abstract
Purpose
Nerve transfers to restore elbow flexion have been described for traumatic brachial plexus palsy in adults. Indications are less frequent in infants and the results are less published.
Methods
Ten patients with obstetrical brachial plexus palsy were operated on for lack of flexion against gravity with ulnar or median nerve transfer to biceps motor branch. The primary endpoint was improvement in elbow flexion and supination.
Results
Mean age at surgery was 12.5 months and mean follow-up was 2.6 years. The Active Movement Scale (AMS) was used to evaluate elbow flexion and forearm supination. At the last follow-up, the average AMS score improved from 0.3 to 5.7 for elbow flexion and from 0.6 to 5.8 for forearm supination. There was no statistical correlation between the age at surgery and the AMS score 18 months post-operatively.
Conclusions
Nerve transfer to the biceps motor branch can improve elbow flexion and forearm supination in selected patients with upper lesions and can be safely performed until the age of two years.
Introduction
Obstetrical brachial plexus palsy (OBPP) often affects C5 and C6 or C5, C6 and C7 roots. One of the main goals in the treatment of those upper palsies is elbow flexion recovery. Surgery is usually planned when infants do not recover elbow flexion before six months of age. The most commonly performed surgery is brachial plexus microsurgical exploration, neuroma resection and nerve grafting.1,2 Unfortunately, nerve grafting is impossible in cases of root avulsion from the cord. 3 Furthermore, the chance of recovery after nerve grafting decreases when surgery is performed after the age of nine months. 4
Nerve transfers to restore elbow flexion have been described for traumatic brachial plexus palsy in adults.5–7 Nevertheless, indications are less frequent in infants.8–18 We asked the following two questions: 1) is nerve transfer to the biceps motor branch from ulnar or median nerve an alternative to brachial plexus exploration to restore elbow flexion and supination in the management of upper OBPP?; 2) until what age can these nerves transfers be carried out?
Patients and Methods
In this retrospective study, patients with OBPP upper palsies without elbow flexion against gravity recovery were operated on between 2001 and 2014 by two upper limb senior surgeons (PJ and FF). Nerve transfer has been performed in three clinical situations: upper root avulsion from the spinal cord, late presentation or failed elbow flexion recovery after primary brachial plexus graft. All patients had pre-operative brachial plexus MRI and roots avulsions were suspected in the presence of myelomeningocele.
We used the surgical technique described for adults; ulnar nerve fascicle to the flexor carpi ulnaris or median nerve fascicle to the flexor carpi radialis were transferred to the motor branch of the biceps. 6 As the ulnar nerve has a very small diameter in young children, it was always dissected with the use of an optical microscope in order to safely separate the fascicles. The motor fascicle to the flexor carpi ulnaris was found by electro stimulation. The motor branch of the biceps was found at the entrance of the biceps muscle. Proximal separation of the biceps nerve branch from the musculocutaneous nerve was performed in order to obtain adequate length for a suture without tension. Nerve suture was always performed with fibrin glue. The distinctive paediatric features were therefore the exclusive use of optical microscope and the use of a NIMBUS i-Care light tripolar electrode (INNOPSYS, Carbonne, France) for specific fascicle selection (Fig. 1).
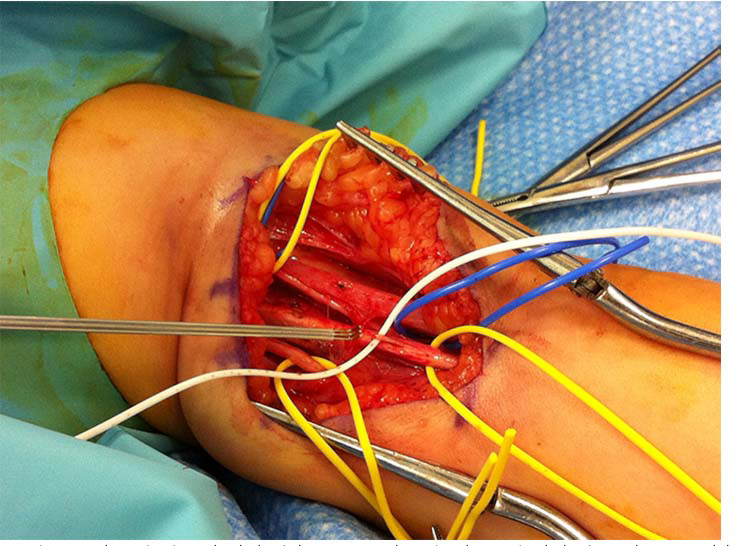
Nerve selection with tripolar electrode. The hook shape is required to isolate the fascicle. The hook is made of an anode between two cathodes to avoid any diffusion of the stimulation.
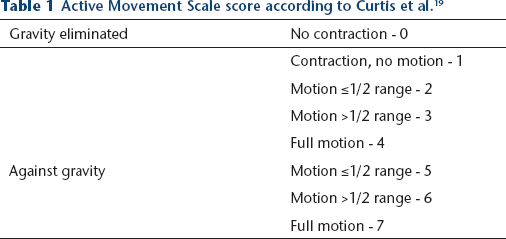
The two senior surgeons gathered the data. The active ranges of movement for elbow flexion and forearm supination were measured by a goniometer. When the patients were not able to understand simple orders, data were graded with toy stimulation or with the parents’ help. Elbow flexion was defined by the angle between the humerus and the ulna on a profile view. Forearm supination was defined by angle between the dorsal side of the hand and the humerus line on a face view. We used the Active Movement Scale (AMS) to evaluate the function (Table 1). This score includes details about range of movement and muscle strength and is very effective for OBPP palsy follow-up. It has an excellent interobserver reliability for elbow flexion/extension, but moderate/poor for forearm supination and pronation. 19 A score lower than 5 is defined as a poor result, a score equal to 5 as a fair result and a score higher than 5 as a good result and a functional upper limb. The infants were examined pre-operatively and three months, six months, one year and then again every six months post-operatively.
Active Movement Scale score according to Curtis et al. 19
Statistical analysis
We used non-parametric tests because of the low number of patients and the non-normal layout of AMS score. Spearman's correlation coefficient was used to determine the association between age at surgery and AMS score at 18 months. Pearson's correlation coefficient was used to ascertain the association between age at surgery and functional movement age recovery according to AMS score. Fisher's exact test was used to compare post-operative function according to the level of root lesion and to the surgical indication. A p-value ≤ 0.05 was considered significant.
Results
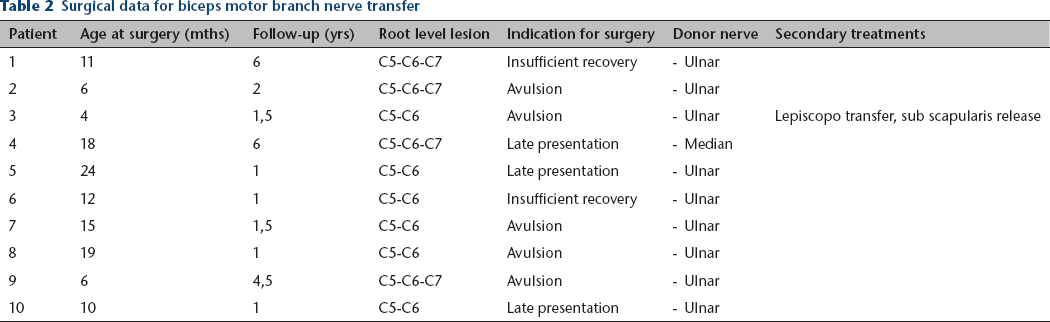
Data related to surgery are presented in Table 2. The mean follow-up was 2.6 years (1.5 to 6; sd 2.1). The average age at surgery was 12.5 months (4 to 24; sd 6.5). Some of these patients were potentially within the expected period of obtaining further recovery but with no active elbow flexion improvement for a six-month period. Six patients had a C5-C6 lesion and four a C5-C6-C7 lesion. Five patients had nerve transfer for root avulsion, three for late presentation and two for insufficient recovery after brachial plexus graft. Concerning the donor nerve for the biceps motor branch, ulnar nerve was used in nine cases and median nerve in one case because the ulnar nerve was found to be too small at the time of the surgery.
Surgical data for biceps motor branch nerve transfer
At the last follow-up, the mean active elbow flexion was 110° (0° to 140°) and the mean active forearm supination was 54° (0° to 80°).
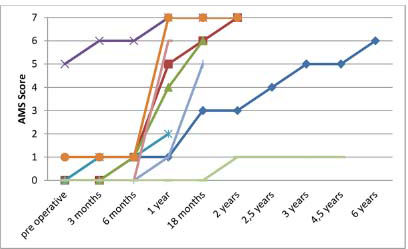
Figure 2 shows the evolution of the AMS score for elbow flexion depending on time. After one year, the mean AMS score was 4.5. After 18 months, the mean AMS score was 5.3. At the last follow-up, the mean AMS score was 5.7 (1to 7); seven patients had a score equal to 6 or 7 and two equal to five (Table 3).
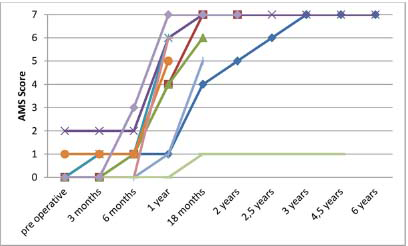
Active Movement Scale score for elbow flexion according to the time for each patient.
Data for elbow flexion and forearm supination after nerve transfer
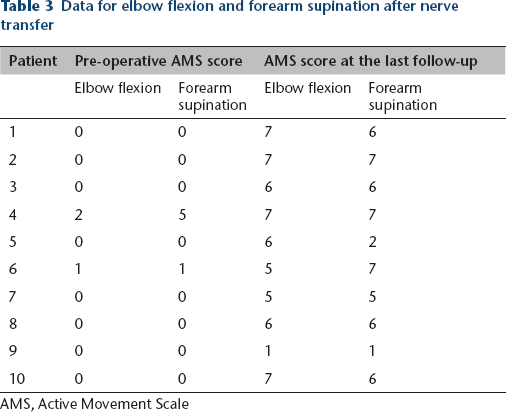
AMS, Active Movement Scale
Figure 3 shows the evolution of the AMS score for the forearm supination depending on time. After one year, the mean AMS score was 3.9. After 18 months, the mean AMS score was 4.8. At the last follow-up, the mean AMS score was 5.8 (1 to 7); four patients had a score equal to 7, one patient had a score equal to 6 and one patient had a score equal to 1.
Active Movement Scale score for forearm supination according to the time for each patient.
There was no statistical correlation between the age at surgery and the AMS score at 18 months for elbow flexion (Spearman Rank-order Coefficient (rs) = 0.13, p = 0.779) and forearm supination (rs = 0.358, p = 0.43). The root lesion level was not associated to the functional recovery after two years for elbow flexion (p = 0.428) and for forearm supination (p = 0.428). There was no correlation between the patients operated on for late presentation, root avulsion from the spinal cord or failed biceps flexion recovery after two years for elbow flexion (p = 0.771) and for forearm supination (p = 1). The age at surgery was not associated to the speed of functional recovery for elbow flexion (ρ: -0.45; 95% confidence interval (CI) -0.8418 to 0.2491; p = 0.19) and for forearm supination (ρ: 0.1597; 95% CI -0.5225 to 0.7172; p = 0.659).
We did not find any limitation of wrist function after the loss of the flexor carpi ulnaris or flexor carpi radialis innervation. However, the follow-up is short and this point should be re-evaluated at the end of growth. We had one case with post-operative claw deformity of the fourth and fifth fingers in relation to temporary weakness of intrinsic muscle. The patient recovered full movement after six months.
Discussion
One of the main objectives in upper OBPP is elbow flexion recovery against gravity. 20 Currently, the consensus is to perform a surgical exploration of the brachial plexus with neuroma resection and nerve grafting when the infants do not recover elbow flexion before the age of six months.1,12 Unfortunately, the only possibility for nerve repairs in case of root avulsion, late presentation, insufficient recovery or dissociative regeneration after primary brachial plexus repair is nerve transfer. 21 Nerve transfers have been well described in adults. Their effectiveness is superior to nerve grafting in traumatic brachial plexus palsy. 7
Our study depicted satisfactory elbow flexion results two years after nerve transfer with a flexion against gravity in nine out of ten patients. We had two patients with an AMS score equal to 5. However, these two patients also had a short follow-up and may improve their AMS score with the time (Fig. 2). Every patient who started recovering one year after the transfer achieved good elbow function according to the AMS scoring system at the last follow-up. In our series, the recovery was gradual. Biceps contraction usually starts between three and six months. Flexion without gravity starts between six months and one year. Flexion against gravity starts coming out one year post-operatively. Similar values are found in the literature.11,13,16,17 Neurotisation on the biceps motor branch is efficient but can also fail. There is one case in our study, probably because the child presented a missed initial total OBPP with partial recovery on the lower roots. 16 Further studies are mandatory to assess whether the tripolar electrode may help to determine if there is adequate recovery of the fascicle used in transfer.
Although results of elbow flexion recovery were already published in OBPP, there is only one study to our knowledge presenting results about forearm supination. 16 Contrary to our study, only 21% of the infants recovered forearm supination after nerve transfer on the biceps motor branch. In an article by Little et al, 16 no supination recovery was found if surgery was performed after the age of eight months. We did not find that the age at surgery was a predictive factor for supination recovery. This conflict might be explained by the intensive physiotherapy programme for our patients to maintain the complete passive supination pre- and post-operatively. This apparent difference may also be explained by the lack of long-term follow-up in Little et al's 16 study.
We did not find any correlation between age at surgery and the final AMS score. Similar findings have been published but functional recovery seems to be less reliable when infants grow up. 17 The period before surgery is longer in children than in adults but the deadline for nerve transfer in OBPP is not clearly defined.22,23 Some authors find a correlation between a young age at surgery and a better recovery. 16 We did not find this correlation in our study. Three patients in our series were older than 18 months (18, 19 and 24 months, respectively) and all achieved a good final result. A recent study presents poorer results than ours after performing nerve transfer in a group of patients with a mean age of 41 months. 24 The small number of patients in our series and the absence of a control group make it difficult to draw firm conclusions regarding for what age this technique should be recommended. Nevertheless, the ideal age seems to be between two and three years old.
Finally, we had one case of partial ulnar nerve palsy with spontaneous recovery. This complication might be related to the extensive ulnar nerve dissection to select the fascicle to be transferred to the biceps.
There are several limitations in this study. First, this is a retrospective study with a small number of patients and a short follow-up period. The statistical power is therefore insufficient to show any correlation between age at surgery or root level to recovery. Further evaluation is mandatory, especially at the end of growth. Secondly, there is a lack of a control group of similar patients. The evaluation with the AMS score should be enhanced by a more functional evaluation as the brachial plexus outcome measure. 25
Nevertheless, although this pathology is rare, this study showed that nerve transfer on the biceps motor branch is a reliable surgery in upper lesions to recover elbow flexion and forearm supination and can be performed until the age of two years. Although these results are encouraging, more powerful studies should be undertaken to specify outcomes and surgical indications between nerve transfer and primary brachial plexus exploration in upper OBPP.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.