
Abstract
Introduction:
The objective of this study was to search existing literature on nerve reconstruction surgery in patients with obstetric brachial plexus palsy to determine whether treatment with supraclavicular exploration and nerve grafting produced better elbow flexion outcomes compared to intercostal nerve transfer.
Methods:
This study was a systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Individual Patient Data guidelines. A systematic search was conducted using multiple databases. An ordinal regression model was used to analyze the effect of using supraclavicular exploration and nerve grafting or intercostal nerve on elbow flexion with the two scores measured: elbow flexion Medical Research Council scores and Toronto active movements scale scores for elbow flexion.
Results:
A final patient database from 6 published articles consisted of 83 supraclavicular exploration and nerve grafting patients (73 patients with Medical Research Council and 10 patients with Toronto score) and 7 published articles which consisted of 131 intercostal nerve patients (84 patients with Medical Research Council and 47 patients with Toronto scores). Patients who underwent supraclavicular exploration and nerve grafting presented with an average Medical Research Council score of 3.9 ± 0.72 and an average Toronto score of 6.2 ± 2.2. Patients who underwent intercostal nerve transfer presented with an average Medical Research Council score of 3.9 ± 0.71 and an average Toronto score of 6.4 ± 1.2. There was no statistical difference between supraclavicular exploration and nerve grafting and intercostal nerve transfer when utilizing Medical Research Council elbow flexion scores (ordinal regression: 0.3821, standard error: 0.4590, p = 0.2551) or Toronto Active Movement Scale score for elbow flexion (ordinal regression: 0.7154, standard error: 0.8487, p = 0.2188).
Conclusion:
Regardless of surgical intervention utilized (supraclavicular exploration and nerve grafting or intercostal nerve transfers), patients had excellent outcomes for elbow flexion following obstetric brachial plexus palsy when utilizing Medical Research Council or Toronto scores for elbow flexion. The difference between these scores was not statistically significant.
Type of study/Level of evidence:
Therapeutic Study: Investigating the Result of Treatment/level III.
Introduction
With an estimated incidence between 0.4 and 4 per 1000 live births obstetric brachial plexus palsy (OBPP) is rare but can be a debilitating injury at birth. The extent of nerve involvement is different among patients and can be categorized into the following syndromes: upper trunk (C5-C6 ± C7) and complete (C5-T1). While complete palsy presents with effects on shoulder, elbow, wrist, and hand movement, patients with upper trunk palsy most prominently have a lack of active shoulder abduction and elbow flexion.1,2 While most OBPP cases may result in spontaneous recovery, there are a variety of primary and secondary surgical interventions that can be used to treat OBPP to improve function of the affected limb. 3 Primary surgical interventions include neurolysis, nerve grafting and nerve transfers.
Traditionally, primary surgery to improve elbow flexion in OBPP involves a supraclavicular incision, subsequent exploration of the brachial plexus to identify viable proximal roots and then attachment of these roots to the trunk, cord, or peripheral nerve through a nerve graft.4,5 While proximal nerve transfers are performed near the site of injury in the supra- or infra-clavicular fossa, distal nerve transfers are those performed beyond the brachial plexus zone and near the neuromuscular junction.
Proximal nerve transfers usually include diagnosing the lesion via brachial plexus exploration and dissection, followed by surgical intervention. These procedures have been well studied and produce excellent outcome. This operation presents with some disadvantages including longer recovery times and greater technical demands as compared to nerve transfers. 6
Unlike proximal nerve transfers, distal nerve transfers are performed away from the site of injury and closer to the target muscle, do not require nerve grafts, result in shorter surgery times and, skills wise, are within grasp for a surgeon without high volume exposure to OBPP cases due to decreased technical demand and subjectivity of the procedure. Although there are clear benefits of distal nerve transfers, these are at the expense of full donor nerve function and post-operative complications such as respiratory failure. 6 The distal procedure of intercostal nerve (ICN) transfer for reconstruction of the musculocutaneous nerve (MCN) has been used for adult brachial plexus injury. More recent studies have shown it to be effective in obstetric brachial palsy patients, with 70%–90% of patients achieving greater than or equal than Medical Research Council (MRC) M3 strength of biceps.7,8
Elbow flexion is critical to a child’s development and to many activities of daily living, from eating to buttoning a shirt. OBPP involving the C5-C6 nerve roots and global palsy without recovery of C5-C6 frequently results in reduced to absent elbow flexion. 9 Thus, the reconstructive strategies currently employed in improving elbow flexion in OBPP patients are of considerable interest. Given that there has been no conclusive determination as to whether one procedure may be superior to the other, there is a significant need to analyze the current data.
The aim of this study was to analyze all available literature and assess whether supraclavicular exploration with nerve grafting or ICN transfer is more effective in improving elbow flexion utilizing a variety of outcome measures.
Methods
Literature search
This study was conducted under Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Individual Patient Data (PRISMA-IPD) guidelines. First, a systematic search of the literature was conducted using PubMed, Cochrane, Web of Science, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases. Specific search terms including “brachial plexus,” “injury,” “palsy,” “nerve plexus,” “upper plexus,” “pediatric,” and “surgery” were used. The complete collection of Boolean searches is provided in Supplemental Appendix A. From the initial set of articles, duplicates were removed, followed by an abstract and full-text screening. In these screenings to build the preliminary database, English text studies on brachial plexus surgery in pediatric patients were identified. The exclusion criteria for these studies were as follows: (1) studies that were not full text; (2) studies classified as commentaries, review papers, or editorials; (3) studies that were non-human or had less than three participants; (4) studies which had full texts that were inaccessible. The full-length texts were accessed online. For completion, the references of all selected articles were cross-checked. If these articles were not previously included and fulfilled the inclusion/exclusion criteria, they were included in the database.
From this preliminary database, articles were then screened for relevance to this study’s specific objective. Only studies which investigated patients who received ICN transfers or treatment with supraclavicular exploration and nerve grafting (SENG) were included. Studies with ICN nerve transfers and SENG were then subdivided into groups based upon the type of outcome measures used to evaluate elbow flexion. These included the Medical Research Council (MRC) Scale for Muscle Strength (elbow flexors) and elbow flexion Toronto Active Movement Scale (Table 1).
ICN and SENG studies.
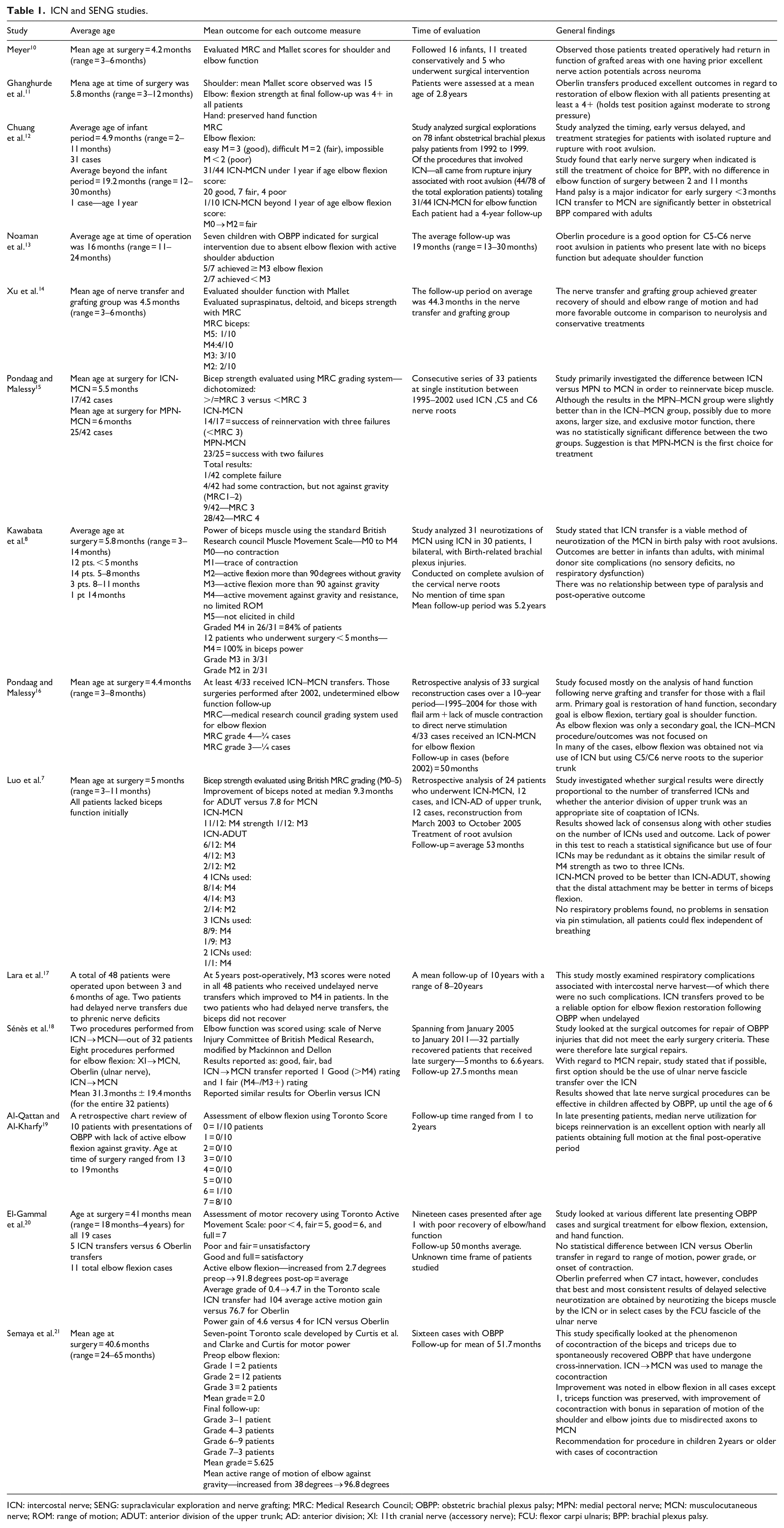
ICN: intercostal nerve; SENG: supraclavicular exploration and nerve grafting; MRC: Medical Research Council; OBPP: obstetric brachial plexus palsy; MPN: medial pectoral nerve; MCN: musculocutaneous nerve; ROM: range of motion; ADUT: anterior division of the upper trunk; AD: anterior division; XI: 11th cranial nerve (accessory nerve); FCU: flexor carpi ulnaris; BPP: brachial plexus palsy.
Data extraction
Data extracted from articles in the preliminary database included number of patients, patient characteristics, follow-up, outcomes following surgery, and information about any secondary procedures. Data extraction was conducted by all the authors. The authors of articles that did not have comprehensive data were contacted for additional information. If these authors did not respond or could not provide additional data, these studies were excluded from the present analysis.
Statistical methods
We employed an ordinal regression model to analyze the effect of using SENG or ICN on elbow flexion with the two scores measured: elbow flexion MRC and elbow flexion Toronto Active Movement Scale. We choose ordinal regression because it is designed for order response categorical variable and allows for the independent variable (SENG/ICN method in our case) to be either continuous or discrete. We used a logit link function which is the most widely used in statistical application literature, and the model is formulated as: log(Pr(Score≤j)Pr(Score>j)) = β0j;+β1Method+ɛ.
Results
The PRISMA-IPD workflow used to identify studies is shown in Figure 1. Initially, 2936 texts were identified using the search terms. After a title screening, texts that were irrelevant to pediatric brachial plexus palsies, case reports, traumatic injuries, meta-analyses, editorials, secondary surgeries, reviews, non-microsurgical operations, and unavailable full texts were excluded, resulting in an initial index of 93 full texts. An additional 18 texts were identified by cross-references. This produced a preliminary database of 111 texts. Afterwards, texts were screened for relevancy to SENG and ICN transfers. This produced 49 texts. Following this, the authors screened the published texts for results reported (elbow flexion MRC and elbow flexion Toronto scores) (Figure 2). In addition, the authors filtered out articles that reported grouped results or non-standardized scores. For example, some authors chose to report scores of as MRC scores 4 and 5 as excellent, 2 and 3 as adequate, and 1 as unsuccessful. Attempts were made to reach out to these authors for a more detailed report of patient outcomes; however, this was unsuccessful in most instances. A final patient database from six published articles consisted of 83 SENG patients (73 patients with MRC and 10 patients with Toronto score) and seven published articles which consisted of 131 ICN patients (84 patients with MRC and 47 patients with Toronto scores).
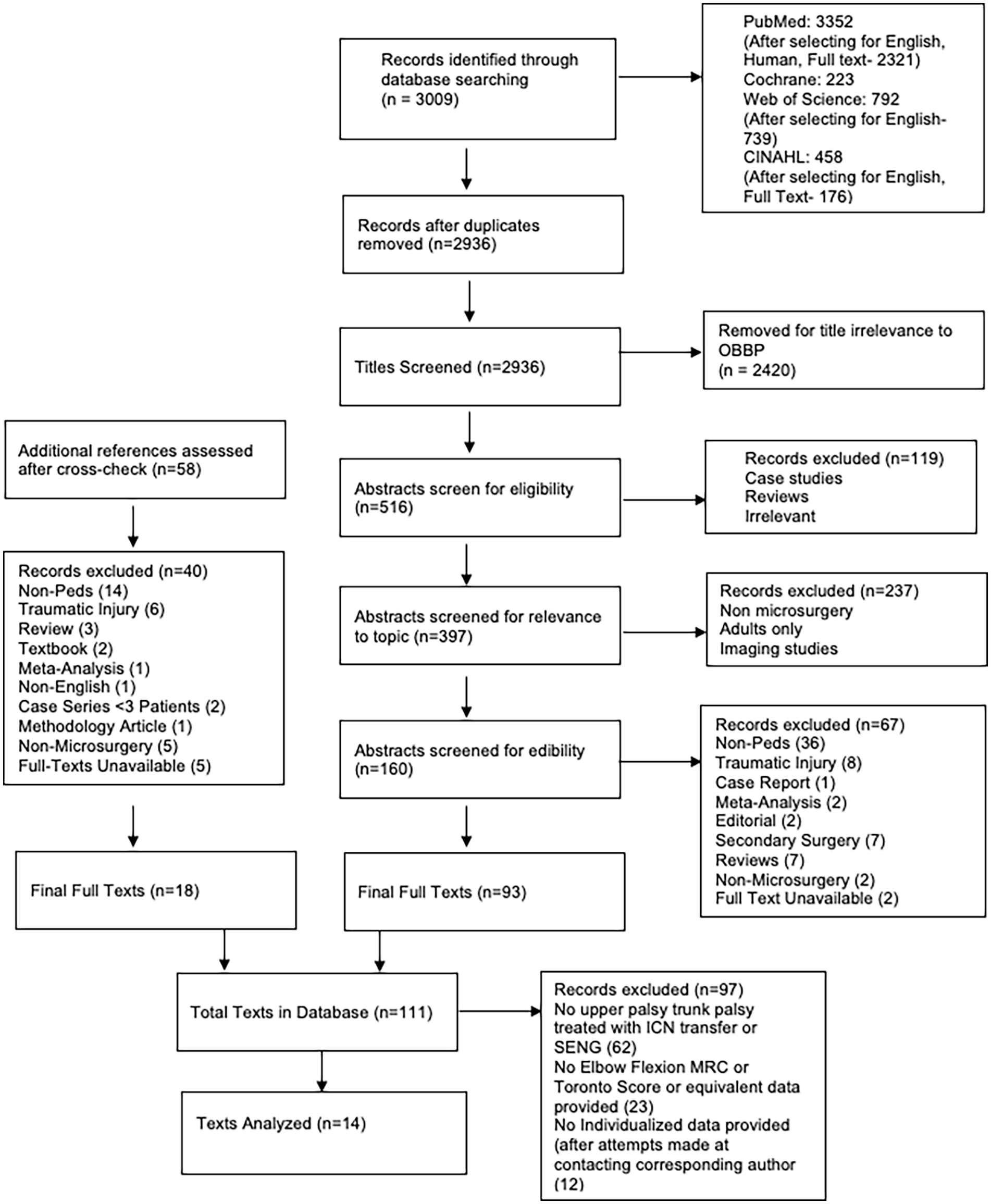
PRISMA workflow.
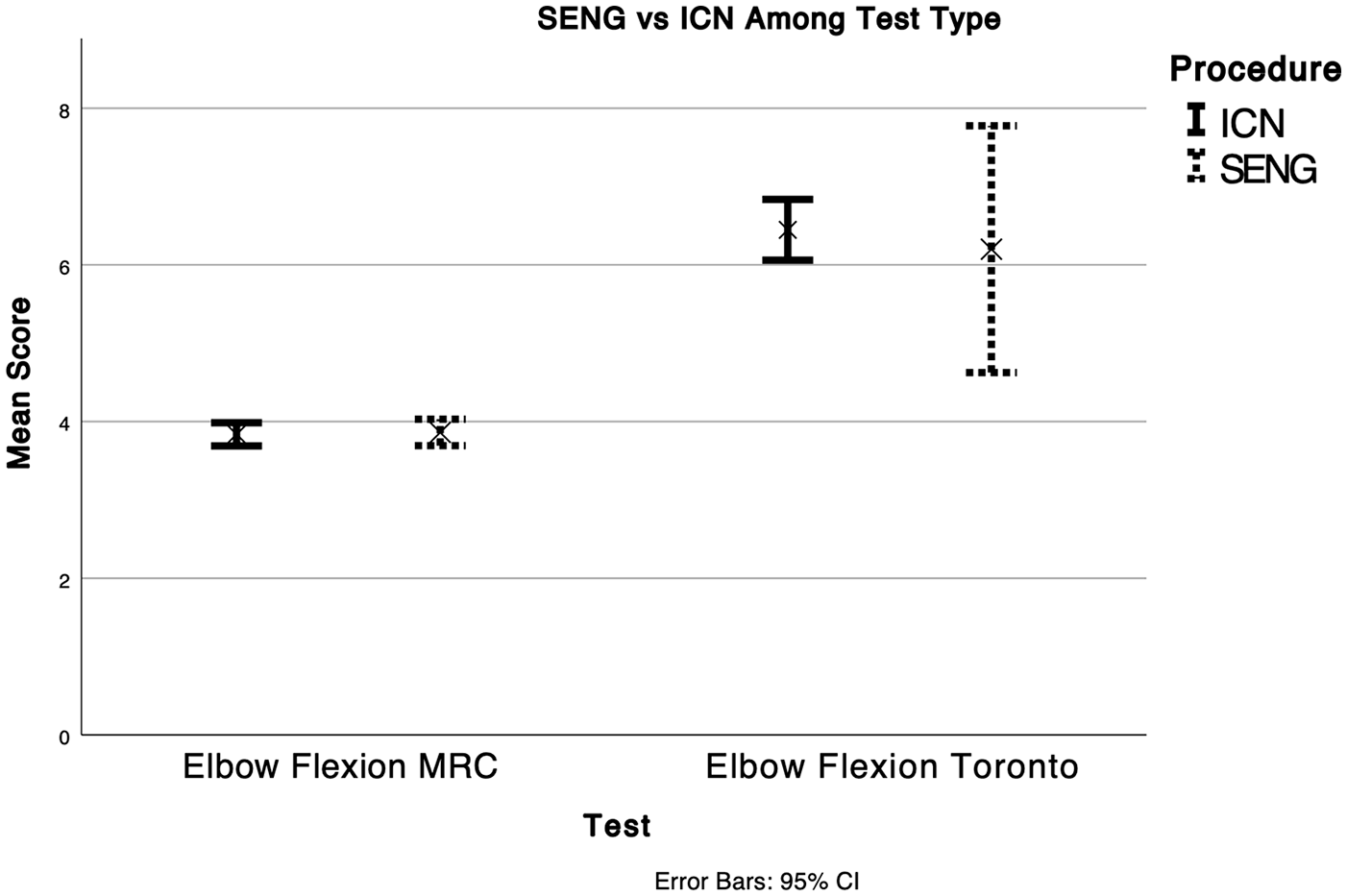
SENG versus ICN among test type (elbow flexion MRC, elbow flexion Toronto).
Data gathered from six texts of patients undergoing SENG present an average MRC score of 3.9 ± 0.72.10 –15 Data gathered from five texts of patients undergoing ICN transfers present an average MRC score of 3.9 ± 0.71.7,8,16 –18 Data gathered from one text of patients undergoing SENG present an average Toronto score of 6.2 ± 2.2. 19 Data gathered from two texts of patients undergoing ICN transfers present an average Toronto score of 6.4 ± 1.2.20,21 The regression value between SENG and ICN transfers when comparing MRC scores is MRC scores is 0.3821 (standard error 0.4590, p = 0.2551). The regression value between SENG and ICN transfers when comparing Toronto scores is 0.7154 (standard error 0.8487, p = 0.2188). There is no statistical significance between SENG and ICN transfers when utilizing MRC or Toronto scores.
Discussion
Currently, there is little guidance for the use of different surgical procedures for patients undergoing repair for OBPP. Treatments for patients with upper nerve palsies emphasize the restoration of active shoulder abduction and elbow flexion. Traditionally, the use of SENG has produced favorable outcomes for patients. However, newer procedures that include the use of ICN transfers have not been extensively compared to proximal surgeries for elbow flexion in the pediatric population. We have found that both procedures result in excellent patient outcomes as a function of elbow flexion measured using the MRC score.
The use of SENG provides surgeons and patients with advantages for repair. This surgical procedure has been the standard for brachial plexus lesions in adults and children. Multiple studies have shown that this procedure has provided patients with a safe and effective treatment option for upper palsies. Furthermore, the surgical window allows for not only repair but also diagnosis and visualization of the lesion. This allows repair of multiple deformities and injuries that may be present in patients during one operation. While these procedures have been well studied and produce excellent outcomes, this operation presents with some disadvantages including the morbidity of longer dissections in an already traumatized area, longer operative times, and the necessity of subjective factors such as visual assessment of lesions in continuity and relying on intraoperative nerve action potentials.6,22 In addition, SENG procedure is not appropriate in all patients, especially in more extensive injuries with poor quality of proximal donors accompanied by root avulsion.
Distal nerve surgeries can provide patients with an improved post-surgical recovery experience as patients tend to have a faster recovery period. Furthermore, there is strong evidence that in the adult population, intra-plexus dual nerve transfers provided better outcomes for shoulder and elbow functions in patients with traumatic upper plexus palsy compared to traditional nerve grafting. However, this procedure does present with some technical and clinical difficulty. While distal transfers spare some operative morbidity due to their distance from the site of injury, this same distance can be a drawback, preventing diagnostic visualization of the affecting lesion. 4 This coupled with potentially decreased donor nerve function and lower Mallet scores can call into question the value of ICN procedures compared to SENG, 6 taking into account that pros and cons of both procedures can only be debated for a group of patients where the both options exist, as opposed to patients with poor proximal donors where SENG cannot be performed. Furthermore, complications of ICN transfers have been explored and include pleural tears, wound infections, pleural effusions, acute respiratory distress syndrome, and wound seromas. 23 Because of the lack of long term studies, it is unclear the total effect of ICN transfers in the long term such as chest deformity or influence on ventilation at an older age. With the literature showing cases of deformity at 20 years post–operatively, there should be hesitancy to make ICN transfer a first-line treatment for pediatric populations. 17
Others have expressed the concern of impaired respiratory function following ICN transfer with concomitant phrenic nerve transection. This concern may be unfounded as the literature has shown comparable pulmonary function in adults after ICN transfer. In a study of 42 adult patients undergoing phrenic nerve transfers and ICN transfers, it was found that there was no significant difference in phrenic nerve transfers and multiple ICN transfers compared to phrenic nerve transfers alone. 24 In addition, other studies concluded that 10 adult patients undergoing simultaneous phrenic and ICN transfers did not produce clinically evident respiratory dysfunction post-operatively. 25 To our knowledge, there are no studies describing these complications in pediatric patients.
While conducting this study, many of the shortcomings regarding literature data presentation were highlighted. Some of these shortcomings can be attributed to a lack of studies containing children undergoing ICN transfers. In addition, a lack of standardization when compiling results contributed to the limited number of studies that can be compared. Data are often grouped differently between authors as some choose to report results as a function of time, procedure, location, or final outcome. This lack of standardization makes it difficult for surgeons to compare treatment options when choosing the operations that are best for their patients. Furthermore, very few authors provide individual data on patient outcomes. This can make it difficult to compare results and identify differences between selection criteria and functional results between different sets of literature. These issues are especially prevalent in the literature surrounding the treatment and assessment of brachial plexus injuries. Previous attempts have been made to find a consensus on how to report data using the international Plexus Outcome Study Group (iPLUTO) project. 26 Some of the recommendations include the use of a data set and timing protocol when providing data in all scientific papers.
There are several limitations to this study. Limited sample sizes and inability to personally and empirically assess each patient hindered our ability to provide concrete insights and recommendations. Furthermore, nerve grafting to the anterior division of the upper trunk and ICN transfer to the MCN are not always utilized for different types and severities of injury. This prevented direct comparison between the two surgical options and can introduce bias. The use of ICN transfers for obstetric brachial plexus palsies continues to be an area of unknown for clinicians. Comprehensive and comparative studies for this treatment option are sparse. For physicians and surgeons to be fully equipped to help their patients, there needs to be a standardized, systemic approach for result presentation.
Conclusion
Both SENG and ICN transfers produce favorable outcomes for patients suffering from OBPP. There are a plethora of functional outcomes used to evaluate shoulder, elbow, and wrist function following surgical intervention. Elbow flexion is of particular interest as it is crucial in motor skill development of an infant. In this study, SENG and ICN transfers produced equivalent outcomes when utilizing MRC elbow flexion scores or Toronto active movement scale scores for elbow flexion.
Supplemental Material
sj-docx-1-cho-10.1177_18632521231211644 – Supplemental material for Intercostal Nerve Transfer for Biceps Reinnervation in Obstetrical Brachial Plexus Palsy: A Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Individual Patient Data Systematic Review using Individualized Fusion and Comparison to Supraclavicular Exploration and Nerve Grafting
Supplemental material, sj-docx-1-cho-10.1177_18632521231211644 for Intercostal Nerve Transfer for Biceps Reinnervation in Obstetrical Brachial Plexus Palsy: A Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Individual Patient Data Systematic Review using Individualized Fusion and Comparison to Supraclavicular Exploration and Nerve Grafting by George Abdelmalek, George Ehab Mina, Krittika Pant, Zheshi Zheng, Jasmine Mahajan, Nivetha Srinivasan, Shivani Gupta, Jasmine Shafei, Michael F Levidy, Aleksandra McGrath and Alice Chu in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-2-cho-10.1177_18632521231211644 – Supplemental material for Intercostal Nerve Transfer for Biceps Reinnervation in Obstetrical Brachial Plexus Palsy: A Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Individual Patient Data Systematic Review using Individualized Fusion and Comparison to Supraclavicular Exploration and Nerve Grafting
Supplemental material, sj-pdf-2-cho-10.1177_18632521231211644 for Intercostal Nerve Transfer for Biceps Reinnervation in Obstetrical Brachial Plexus Palsy: A Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Individual Patient Data Systematic Review using Individualized Fusion and Comparison to Supraclavicular Exploration and Nerve Grafting by George Abdelmalek, George Ehab Mina, Krittika Pant, Zheshi Zheng, Jasmine Mahajan, Nivetha Srinivasan, Shivani Gupta, Jasmine Shafei, Michael F Levidy, Aleksandra McGrath and Alice Chu in Journal of Children’s Orthopaedics
Footnotes
Author contributions
A.C. and A.M. conceived the study. G.A., G.E.M., and K.P. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.