
Abstract
Purpose
Mucopolysaccharidoses (MPS) are a group of rare lysosomal storage disorders associated with involvement of multiple organs along with a generalised skeletal dysplasia. Both haematopoetic stem cell transplant and enzyme replacement therapy have improved the outlook for patients while surgery remains high-risk and there is little information on clinical or functional outcome to justify many of the surgical procedures performed. This paper aims to summarise the orthopaedic surgical procedures in MPS patients for which quality of life (QoL) and functional data are available and to describe additional QoL and functional measurement tools of relevance to the assessment of orthopaedic outcomes in MPS.
Methods
We reviewed the available literature to look for reported outcomes of orthopaedic surgery to lower and upper limbs and the spine. In addition, we describe the general and MPS-specific health measures that might be of relevance to the orthopaedic surgeon.
Results
There is some evidence in the literature that orthopaedic surgery may improve QoL and function in some specific aspects of the MPS condition (in relation to genu valgum, carpal tunnel syndrome and trigger digits); however, the literature is sparse and consists of level 4/5 studies only. Further studies of these conditions should include QoL and functional assessment in order to confirm or refute these reports. In other areas (spine and hip), outcomes are judged largely on radiographic appearances with little clinical correlation and short follow-up; however, one long-term study of function following hip dysplasia surgery suggests poor outcomes. Anaesthetic morbidity/mortality is not insignificant in these complex patients with multi-organ involvement. Careful assessment is required, particularly when there is neurological involvement.
Conclusions
Orthopaedic surgeons involved with MPS patients should be encouraged to use and report measures of QoL and function with respect to musculoskeletal manifestations and response to surgery, recognising that such assessments in these complex and challenging patients may require a multidisciplinary approach.
Introduction
Mucopolysaccharidoses (MPS) are a group of disorders caused by single enzyme defects resulting in abnormal glycosaminoglycan (GAG) metabolism with multisystem effects. Symptoms often manifest in infancy or early childhood. Eleven distinct enzyme deficiencies cause seven recognised MPS syndromes. 1
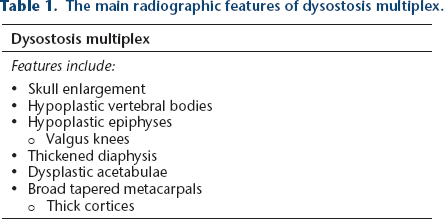
All MPS disorders involve the musculoskeletal system. Dysostosis multiplex refers to a characteristic constellation of radiographic anomalies (Table 1) that is prominent and progressive in MPS. The underlying pathophysiology is not well-understood and histological findings 2 likely reflect complex secondary alterations in cell-signalling rather than direct effects of GAG deposition.
The main radiographic features of dysostosis multiplex.
The outlook for patients with many MPS subtypes has significantly improved due to haematopoetic stem cell transplant (HSCT) for rapidly progressive MPS I (Hurler) patients and enzyme replacement therapy (ERT) for MPS I, II, IV and VI. 3 Unfortunately, these treatments fail to halt the progression of certain systemic manifestations, including musculoskeletal abnormalities. This leads to an increasing number of ageing patients with partially corrected abnormalities 4 and orthopaedic surgery is probably increasing in the MPS population. 5
Surgery in MPS remains high-risk4,6 and must be justified on clinical grounds. Measures of quality of life (QoL) and function are important to determine the clinical interplay in this complex multisystem disease, 3 yet reported outcomes for orthopaedic surgery in MPS more commonly focus on radiological and other musculoskeletal specific measures, rather than evaluating the patient's overall response to orthopaedic intervention.
The aims of this paper are:
to summarise the orthopaedic surgical procedures in MPS patients for which QoL and functional data are available; and to describe additional QoL and functional measurement tools of relevance to the assessment of orthopaedic outcomes in MPS.
QoL and function following orthopaedic surgery in MPS patients: Lower limb
Genu valgum
Surgery for genu valgum is usually performed in MPS IV (highest incidence), I, II and VI.7–9 Interventions include guided growth techniques, osteotomies, gradual correction with the use of external fixation and total knee arthroplasty for end-stage deformities.2,10 If using guided-growth techniques, surgery should be offered early as MPS patients have reduced peak growth velocity. 2
23 MPS IVA patients underwent distal femoral and/or proximal tibial eight-plate hemi-epiphysiodesis at a mean age of 8.3 years (4 to 15) with average follow-up of 44 months (19 to 84). 9 Three patients underwent repeat hemi-epiphysiodesis and one femoral osteotomy was performed for residual deformity. Functional outcomes were assessed subjectively according to the use of mobility aids and objectively using the 6-minute walk test (6MWT). Of the 23 patients, 19 remained mobile at final follow-up; three previously mobile patients became immobile post-surgery for no obvious medical reason: one post osteotomy, one a few months after eight-plate insertion and one three years after eight plate insertion. The 6MWT is a submaximal intensity endurance test assessing cardiorespiratory and musculoskeletal function in the MPS population.11,12 It has been used extensively in MPS clinical research to characterise natural history,11,13 as well as a primary measure of efficacy in trials of ERT.14–18 The test is performed on a 30-m long, flat course and the patient is instructed to walk as far as possible in 6 minutes, using any of their normal walking aids. 12 In research settings, the test is often performed on two separate days, with either the average result taken for analysis15,16,19 or the greater distance. 14 Upper and lower limits for inclusion are generally set to minimise any ceiling effect and to exclude patients whose walking has deteriorated to a point where it is irrecoverable despite therapy.11,15 Correction of genu valgum in MPS by hemi-epiphysiodesis was associated with an average improvement of 69.5 m walking distance (30% improvement) post-surgery (p = 0.03) in the 15/23 patients for whom 6MWT data were available. 9 However, patients remain significantly impaired. The post-surgery average distance covered of 297 m contrasts strongly with a distance of 618 ± 79 m seen in healthy individuals aged 5 to 17 years. 20
Hip dysplasia
Hip dysplasia is found in almost all MPS I patients and also in MPS II, III, IV and VI. As in other childhood conditions of hip subluxation and dislocation, acetabular and femoral osteotomies have been performed to achieve femoral head coverage.2,21 Hip development in these patients is associated with femoral head epiphyseal dysplasia that is osteonecrosis-like but not related to surgical intervention. In MPS III, the changes are less frequent but more often resemble true osteonecrosis.2,10,22 High rates of recurrent hip subluxation post-operatively have also been reported for MPS IV. 23 Total hip replacement may become more common with systemic MPS therapy leading to prolonged lifespan. 2 A 2013 consensus statement recommended consideration of early surgical hip reconstruction in MPS I patients following HSCT, but there was not consensus as to whether surgery should be offered to all patients to prevent complications or only symptomatic patients. 24
The only study reporting functional outcomes following hip surgery in MPS does not support early hip reconstruction in MPS I post-HSCT if the goals are satisfactory long-term radiological and functional outcomes. 25 A total of 13 patients (24 hips) underwent surgery, with the majority undergoing a Salter pelvic osteotomy +/- proximal femoral osteotomy, a single patient undergoing femoral osteotomies only and another open reduction in conjunction with femoral and pelvic osteotomies. The average age at surgery was four years (2 to 6.3) and average follow-up was 14.6 years (10.3 to 21.6). Despite achieving stable, well-covered hips, at final follow-up advanced degenerative changes were seen radiologically in 10/24 (41%) hips. The authors used the Harris Hip Score (HHS) 26 for assessment of function. The score has a maximum of 100 points (best possible outcome) and cases with scores less than 70 are consistent with poor hip function and can be considered surgical failures. 27 Of 13 cases, seven were considered surgical failures in this series. There may be a role for hip reconstruction in terms of improving anatomy for a later total hip arthroplasty but this would be speculative and not measurable in terms of QoL or functional outcome measures.
Further evidence that radiological hip pathology in MPS has poor correlation with function was provided by an assessment of pelvic radiographs reported in the previously described MPS IV genu valgum study. 9 There was no correlation between 6MWT distances and degree of hip migration, and patients with hip migration percentage greater than 40% had no increased probability of being wheelchair-bound.
Ankle and foot deformity
Ankle valgus and foot deformities of equinus, hindfoot valgus and forefoot adductus with prominence of the first metatarsal head and curly toes are seen in MPS. 28 Non-surgical interventions include orthotics and custom footwear and surgical interventions include guided-growth techniques and osteotomies.2,29 Surgical functional and QoL outcomes have not been reported for foot and ankle procedures in MPS. 18 patients, with a mean age of 10.3 years (4 to 21), with MPS I treated with HSCT who had not undergone foot and ankle surgery were evaluated for baseline function using the Oxford Foot and Ankle Questionnaire for Children (OxAFQ-C). The OxAFQ-C is a 15-item child- or parent (proxy)-reported health status questionnaire validated for children aged five to 16 years. 30 Questions cover physical, school and play, and emotional domains, with an additional question regarding footwear. A score of 60 is considered healthy. 28 Four of 18 patients tested with MPS I had a score of 60. The average score was 45.7 (11 to 60). The functional domains scored lower than those associated with emotional impact or school and play. Ten of 18 patients were unable to wear stock footwear.
Upper limb
Skeletal deformities
Upper extremity skeletal deformities are most severe in MPS IV due to the associated joint laxity. Severe ulnar deviation at the wrist can be treated with external splints or surgically with wrist arthrodesis or partial arthrodesis.8,31 Function and QoL outcomes following wrist arthrodesis have not been reported in MPS.
Carpal tunnel syndrome and trigger fingers
Carpal tunnel syndrome is essentially unknown in children generally but common in MPS I, II and VI. 32 Many MPS children have no obvious symptoms 33 and routine neurophysiological testing from five years of age has been recommended to permit early open carpal tunnel release before permanent nerve damage occurs. Concomitant neurolysis of the median nerve is controversial.34,35
Trigger fingers are seen frequently (MPS I, II and VI) and often present in association with carpal tunnel syndrome (especially types I and II). 36 Trigger digits are treated surgically with an A1 and/or A3 pulley release. One paper recommends partial resection of the flexor digitorum superficialis tendon and careful debridement of the tenosynovial deposits 37 to reduce recurrence.
17 children who underwent open carpal tunnel surgery with or without concomitant trigger digit release were evaluated for post-operative hand function using a questionnaire, the details of which were not reported but included asking parents to grade the post-operative hand function improvement; the frequency of hand pain, numbness, and night pain; and their child's difficulty performing tasks. 37 The average length of the post-operative follow-up period was three years. Of the eight children who underwent carpal tunnel surgery as well as trigger digit surgery (A1 +/- A3 pulley release +/- resection of flexor digitorum superficialis slip), the parents of four patients reported no difficulty with tasks, two reported occasional difficulties and two reported frequent difficulties. Parents reported increased dexterity and spontaneous hand use. The authors caution that for optimal outcomes, trigger digits must be distinguished pre-operatively from joint stiffness. Phalangeal joint contracture is found in all MPS types, except for MPS IV (and IX). 36
Spine
Thoracolumbar and cervicothoracic deformity
Thoracolumbar kyphosis is a classic finding in MPS I and has also been reported in MPS II, 38 IV and VI.10,39–41 Scoliosis can occur in association with kyphosis or in isolation, but surgery for scoliosis is uncommon in the absence of significant kyphosis. 10,42,43
Cervicothoracic kyphosis can also occur in MPS I and IV, particularly in conjunction with thoracolumbar kyphosis.42,44
Deformity progression,40,43 defined as > 10° increase over a 12-month period,41,45 kyphosis > 40° to 45°,39,41,45 disruption of sagittal balance 41 and/or neurological compromise 39 are reported indications for surgical intervention.
There are no studies reporting QoL and function before and after spinal surgery for thoracolumbar kyphosis. In fact, it has been suggested that QoL is not significantly compromised, even in the presence of severe spinal deformity 46 , and, in the absence of symptoms, some surgeons advocate surgery only for progressive kyphosis > 70°. 2 Although it can be assumed that neurological compromise resulting from thoracolumbar kyphosis would significantly affect QoL and function, neurological compromise as an indication for surgery in this circumstance has been reported rarely. 47 Thoracolumbar spine surgery has been ineffective in the medium term in preventing neurological deterioration in patients where the deterioration has been attributed to pathology elsewhere in the spinal column, ischaemic insult or ongoing deposition of GAG breakdown products.42,48
Craniocervical and upper cervical spine pathology
Upper cervical and craniocervical spine pathology is commonly seen in MPS IV and VI and less commonly in MPS I.10 Myelopathy and neurological abnormalities are more commonly associated with pathology at this level than at the thoracolumbar region.
While surgery is recommended to prevent devastating neurological compromise, there are no studies of QoL or function following cervical spine surgery in MPS to demonstrate surgical benefit. In fact, reports of neurological function and mobility following upper cervical surgery in MPS suggest that the usual outcome is stabilisation of neurological function rather than improvement.49–51 This contrasts with the few reported cases of neurological compromise associated with thoracolumbar surgery, where symptoms improved post-surgery. 52 Expectations for patients presenting with established neurological compromise should be managed appropriately in the light of these reports.
Additional QoL and functional measurement tools in MPS
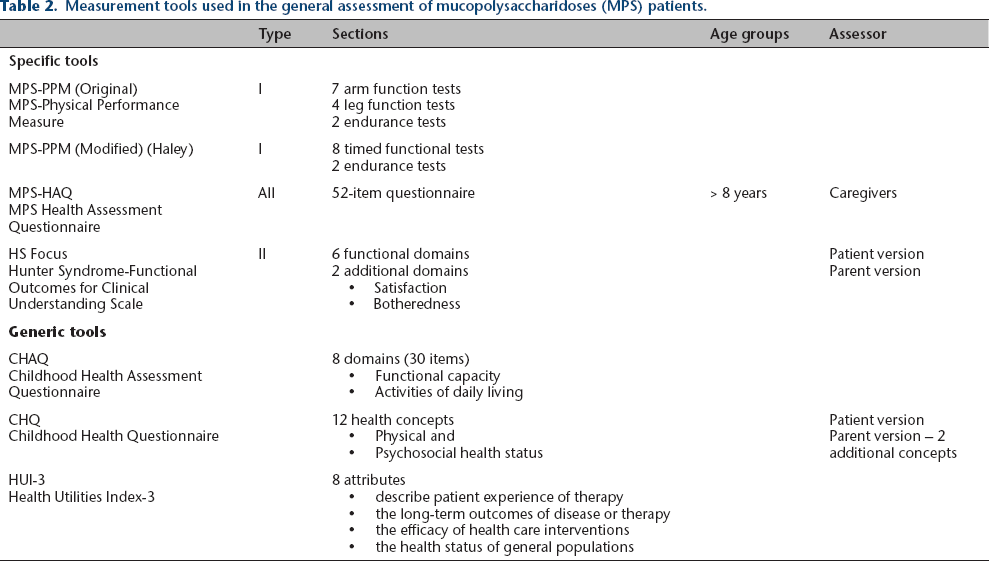
The following disease-specific or generic QoL and functional assessment tools (Table 2) have been used in the setting of clinical management and/or research involving MPS patients and may be useful for the orthopaedic surgeon involved in MPS care.
Measurement tools used in the general assessment of mucopolysaccharidoses (MPS) patients.
The MPS-Physical Performance Measure (MPS-PPM) was developed specifically for MPS I. 53 A revised version was used on ten MPS I children confirming its utility in identifying limitation in age-related physical performance. Good inter-rater and test-retest reliabilities were reported. 54
The MPS Health Assessment Questionnaire (MPS-HAQ) is disease-specific but not type-specific, measuring disability in patients aged over eight years. 55 Parini et al 56 compared MPS-HAQ scores at baseline and at end of ERT (five to nine years), and showed that the subgroup of MPS IIA patients (CNS involvement) improved in 9/52 but worsened in 32/52 items, while MPS IIB patients (no CNS involvement) improved in 23/52 items and worsened in only 3/52.
The Hunter Syndrome-Functional Outcomes for Clinical Understanding Scale (HS-FOCUS) is type-specific, assessing impact of MPS II on function. 57 Raluy-Calado et al 58 evaluated MPS II patients with the HS-FOCUS questionnaire and other generic tools: 1) Childhood Health Assessment Questionnaire (CHAQ); 2) Childhood Health Questionnaire (CHQ); and 3) Health Utilities Index-3 (HUI 3). Children with MPS II were most compromised in physical function and the activities of daily living (ADL), along with a considerable psychological impact, affecting self-esteem and family cohesion most notably.
The CHQ was used to describe QoL in patients with the attenuated form of MPS II and its change over time. Physical QoL decreased while psychosocial QoL increased with age, although older children reported an increasing sense of inadequacy and low self-esteem. 59
Other generic instruments used in MPS patients include the Pediatric Quality of Life Inventory (Peds-QL), KIDSCREEN, European QoL-5 Dimensions (EuroQoL; adults only) and Short Form questionnaire 36 (SF-36; adults only).60–62
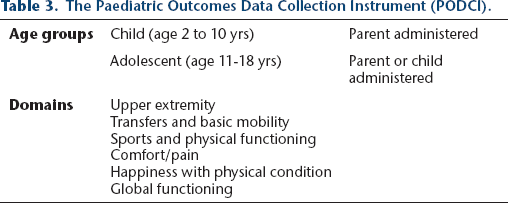
The Paediatric Outcomes Data Collection Instrument (PODCI) (www.aaos.org/outcomes) has become the tool of choice for assessing musculoskeletal-related function and QoL in many conditions, including MPS63,64 (Table 3). As well as assessing baseline status, it is used for assessing medical and surgical interventions with good reliability, construct validity and sensitivity to change. 63
The Paediatric Outcomes Data Collection Instrument (PODCI).
O'Brien et al 65 used the PODCI tool in 25 MPS patients of four different types and demonstrated compromised musculoskeletal function in patients compared with normally developing children in most domains. The lowest scores were recorded in the sports/physical conditioning scale and the highest in the happiness scale. Overall, MPS VI had the highest scores and MPS II the lowest, with significantly more severe deficits in upper extremity and physical function compared with other subtypes.
White et al 63 also used the PODCI to assess the benefits of ERT on function and QoL in seven MPS II children. All patients displayed limitations in shoulder range of motion (ROM) and a combination of compromised function in other joints, including the hip, knee, elbow and ankle with spinal deformity in some. Five of the seven patients received ERT and serial PODCI exams were performed (at baseline and one to two years’ follow-up) to detect changes in function. Positive trends towards improvement were seen in all domains but statistical significance was reached in only three (‘transfers and basic mobility’, ‘sports and physical functioning’ and ‘global functioning’).
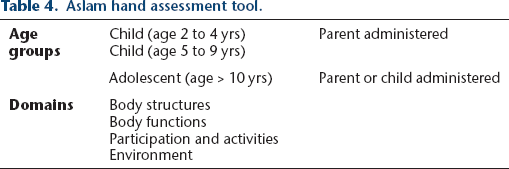
For the specific subjective assessment of hand function, Aslam et al 31 (Table 4) described a questionnaire based on the principles of the World Health Organization International Classification of Functioning, Disability and Health (WHO ICF) which provides a holistic approach based on four domains. Of the ten MPS IV patients studied, all reported hand/upper limb weakness, while pain, paraesthesia and stiffness were variable. Seven and ten out of ten children felt moderately limited in normal classroom activities and physical education/sports, respectively. All patients felt supported by their family and healthcare team. The most difficult activities were carrying heavy objects, personal hygiene, pouring liquids and making the bed, while using games consoles was not difficult. Only 17% (aged < 10 years) and 9% (aged > 10 years) of responses were scored ‘no activity limitation’. 31
Aslam hand assessment tool.
Other recommended questionnaires for assessing upper limb function include the Functional Dexterity Test (FDT) and Disabilities of Arm, Shoulder and Hand (DASH); 8 however, no studies utilising these tools in MPS have been identified.
Gross and fine motor skills contribute significantly to motor functioning. Tools that have been used to assess these skills in MPS populations include the Vineland Adaptive Behavioral Scales (VABS), Peabody Developmental Motor Scales edition two (PDMS2) and Denver Developmental Screening Test (DDST). 5
Objective measures
A number of clinical tests assessing musculoskeletal function in MPS patients have been described. Raluy-Calado et al 58 used objective clinical measures in addition to the four questionnaires described to assess their validity. One measure was joint range of motion (JROM): the authors assessed a total of 23 motions for the shoulder, elbow, wrist, index finger, hip and ankle bilaterally and calculated the average value of two measurements at two separate visits to determine a global JROM score. Parini et al 56 used the JROM to quantify musculoskeletal improvement after ERT in 13 MPS II patients and reported some increase in ROM of shoulders, elbows, hips and knees in the first two years of ERT but with no overall statistical significance.
Aslam et al's 31 objective hand function assessment compared passive and active ROM of the wrist and hand joints and looked at grip strength. Large differences between passive and active ROMs were interpreted as representing significant compromise in joint function. In the ten patients assessed, the difference in interphalangeal joint (IPJt) movement was not clinically significant but active movement at the wrist was significantly compromised. Both gross grip strength and lateral key grip were severely compromised (57% and 93% below the mean normative values, respectively). 31
Harmatz et al 19 assessed the effects of 48 weeks of ERT on endurance, mobility and joint function in MPS VI patients and reported significant improvements in all outcome measures. Endurance and mobility were assessed by a 12-minute walk test, a 3-minute stair climb test and the Expanded Timed Get-Up-and-Go (ETGG) test (Table 5). For joint function assessment, objective measures consisted of shoulder ROM, grip and pinch strength, while pain and stiffness were assessed by an analogue scale based on the Health Assessment Questionnaire (HAQ) and the CHAQ.
Gait and endurance tests.
Conclusions
Following improvements in lifespan for MPS patients due to developments in HSCT and ERT, orthopaedic surgery in MPS is now performed more frequently in certain centres, often following guidelines and practices developed for patients without MPS. 25 A pitfall with this approach is that the orthopaedic pathology in MPS is not similar enough to other pathologies to ensure satisfactory outcomes in MPS patients. The complex pathology may explain poor clinical outcomes following reconstructive hip surgery in MPS, despite satisfactory initial radiological outcomes. 25
Another problem is the multisystem nature of MPS. Cognitive, cardiorespiratory and other musculoskeletal disease can all impact on the outcomes following orthopaedic surgery. Improvement post-operatively of a specific orthopaedic measure may be clinically irrelevant if disease elsewhere significantly limits function and QoL. For this reason, using general, rather than joint specific functional and QoL tools may be more useful in this population.
Despite advances in medical management, peri-operative mortality in MPS remains high (4.2% 30-day mortality for MPS I) 66 Cardiorespiratory complications, including airway difficulties account for 63% of deaths. International management guidelines for MPS I recommend avoidance of operations requiring general anaesthesia where possible and highlight the challenges of providing safe peri-operative care in the MPS population. 67 MPS types with frequent skeletal involvement, are those more likely to require orthopaedic surgery but also those with the highest anaesthetic risk.10,68,69 Peri-operative spinal cord injury in MPS patients is an increasingly recognised complication. This has been reported following both spinal and lower limb surgery in patients with MPS I and IV.48,70,71 In light of these reports, the routine use of spinal cord monitoring for all MPS patients undergoing prolonged orthopaedic procedures should be considered. 72 These reports caution against the use of epidural anaesthesia in MPS patients as it masks the recognition and potential treatment of evolving spinal cord injury. The decision to undertake any orthopaedic surgery in an MPS patient must be well-considered and should be conducted within the context of multidisciplinary management in a centre with appropriate experience and expertise.
There is evidence that orthopaedic surgery may improve QoL and function in MPS with genu valgum, 9 carpal tunnel syndrome and trigger digits; 37 however, the literature is sparse and further studies of these conditions should include QoL and functional assessments in order to confirm or refute these reports. In contrast, there is evidence that orthopaedic surgery fails to improve QoL and function in MPS patients with hip dysplasia, despite successful early radiological outcomes. 25
Orthopaedic surgeons involved with MPS patients should be encouraged to use and report measures of QoL and function with respect to musculoskeletal manifestations and response to surgery.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
This article does not contain any studies with human participants performed by any of the authors.
All three authors declare that they have no conflict of interest.
Dr Williams is funded by the Royal Australasian College of Surgeons, Lumley Surgical Exchange Research Scholarship. Dr Williams has received honoraria and payment for travel expenses from BioMarin to attend mucopolysaccharidosis symposia and expert meetings in the Asia Pacific region.
Miss Eastwood discloses that Biomarin paid travel expenses to the Japanese Orthopaedic Association meeting for an industry-sponsored symposium in December 2015.