
Abstract
Purpose
To review the outcomes of tibial derotational osteotomies (TDOs) as a function of complication and revision surgery rates comparing a cohort of children with myelodysplasia to a cohort with cerebral palsy (CP).
Methods
A chart review was completed on TDOs performed in a tertiary referral centre on patients with myelodysplasia or CP between 1985 and 2013 in patients aged > 5 years with > 2 years follow-up. Charts were reviewed for demographics, direction/degree of derotation, complications and need for re-derotation. Two-sample T-tests were used to compare the characteristics of the two groups. Two-tailed chi-square tests were used to compare complications. Generalised linear logit models were used to identify independent risk factors for complication and re-rotation.
Results
The 153 patients (217 limbs) were included. Average follow-up was 7.83 years. Overall complication incidence was 10.14%, including removal of hardware for any reason, with a 4.61% major complication incidence (fracture, deep infection, hardware failure). After adjusting for gender and age, the risk of complication was not statistically significantly different between groups (p = 0.42) nor was requiring re-derotation (p = 0.09). The probability of requiring re-derotation was 31.9% less likely per year increase in age at index surgery (p = 0.005).
Conclusion
With meticulous operative technique, TDO in children with neuromuscular disorders is a safe and effective treatment for tibial torsion, with an acceptable overall and major complication rate. The risk of re-operation decreases significantly in both groups with increasing age. The association between age at initial surgery and need for re-derotation should help guide the treatment of children with tibial torsion.
Introduction
Rotational deformities of the tibia are common among children with myelodysplasia and cerebral palsy (CP). Unlike idiopathic tibial torsion, torsion in children with a neuromuscular disease often does not resolve without surgical intervention.1,2 In the typically developing child, the tibia is internally rotated at birth and external tibial rotation occurs throughout growth, predictably improving with age. 3 In contrast, external tibial torsion is often progressive, more frequently requiring surgical correction, even in the idiopathic population. 2
In the neuromuscular population, dynamic muscular imbalance, weakness and, in some cases, spasticity commonly lead to progressive rotational deformity that may significantly affect brace wear in all affected patients and gait biomechanics in ambulatory patients1,4–7 (GMFCS I-III in the CP population and lumbar or sacral levels of involvement in the myelodysplastic population). Internal tibial torsion can lead to frequent falls resulting from poor foot clearance - from the ground and from the other leg in swing. External tibial torsion can lead to hindfoot valgus, pes planus, increased valgus stress at the knee, excessive shoe wear, poor orthotic control and trophic ulceration in the myelodysplastic population who lack protective sensation.1,4 Both internal and external torsion may result in lever arm dysfunction, which can lead to the development of crouch gait with resultant decreased velocity, poor endurance and knee pain in both populations.5,7–9
In both groups, significant improvements in gait biomechanics have been reported following tibial derotational osteotomy (TDO).10,11 Surgery should be considered for all tibial torsion affecting gait biomechanics (typically > 20° of absolute rotation in either direction), with the goal of improving brace tolerance, minimising brace requirement and achieving a near-normal gait pattern. 5 Yet despite documented clinical benefits, high complication rates between 5% and 33%4,12–19 and substantial re-torsion rates between 16% and 58%19,20 have dampened enthusiasm for surgical intervention in these populations.
Nevertheless, much of the reported outcomes data are of mixed neuromuscular diagnoses without comparison among these distinctive populations. However, the aetiology and natural history of rotational deformities in these populations are not equivalent, and their response to surgical intervention may also be dissimilar, warranting deeper evaluation into these groups’ surgical outcomes. Further, surgical technique and post-operative management are quite variable among previous reports.4,12–20 As such, the goal of the present study was to review the results of derotational osteotomies as a function of complications and need for revision surgery in a population of children with myelodysplasia compared with a population of children with CP.
Patients and methods
A retrospective chart review was performed to identify patients with myelodysplasia or CP who underwent TDOs for tibial torsion affecting brace wear, standing transfers, gait biomechanics and/or gait velocity between 1985 and 2013. All children included in the analysis with myelodysplasia had low lumbar or sacral level involvement apart from three thoracic-level patients. Functional neurologic level was assigned by the treating surgeon based on manual muscle testing performed by the institution's department of physical therapy at the pre-operative clinical visit. All children included in the analysis with CP were classified as GMFCS I-III except for one GMFCS IV (no GMFCS V). GMFCS level was assigned by the treating surgeon based on functional capacity documented at the pre-operative clinical visit. All GMFCS levels were prospectively documented in the patient charts after 1997, when the original description of the classification system was published. 21 For those patients treated prior to 1997, GMFCS was retrospectively assigned based on a careful chart review by the treating surgeon. Retrospective assignment of GMFCS has been shown to have high inter-observer reliability and to be consistent with levels assigned at the time of evaluation. 22 All participants were aged five years or older and had at least 20° of absolute internal or external tibial torsion that interfered with gait or bracing/shoe-wear, with at least two years of follow-up. Participants were excluded from the analysis for insufficient data, age less than five years at time of index surgery and for less than two years of follow-up.
Rotation was calculated by the two senior authors using thigh foot angle 1 pre-, intra- and post-operatively. All angles were obtained using a goniometer. Pre- and post-operative measurements were obtained prone and intra-operative measurements were obtained supine. Data were insufficient to determine inter-rater and intra-rater reliability. However, this has been previously described in similar studies. 11
All surgeries were performed by the two senior authors (VS, LD) at a single tertiary care paediatric referral centre. The surgical technique used has been previously described. 19 In brief, the surgery is performed supine through an anterolateral longitudinal incision overlying the distal tibia, to allow room for a four to six hole 3.5 mm or 4.5 mm limited contact direct compression plate (LC-DCP) placed proximal to the distal tibial physis. A separate direct lateral longitudinal incision overlying the fibula - at the same level as the planned tibial osteotomy - is made, and a transverse osteotomy is completed using an oscillating saw prior to TDO.
The TDO is created with multiple drill holes placed in parallel and it is completed using a straight AO osteotome to limit osteonecrosis. The derotation is then performed manually, using smooth K-wires placed proximal and distal to the osteotomy site prior to osteotomy as a guide for correction, with a goal to correct to between neutral and 5° external rotation, measured by goniometer. The osteotomy is then fixed using the LC-DCP placed on the anterolateral face of the tibia in compression mode (Fig. 1). The incisions are closed with interrupted nylon sutures over a drain that remains in place for 24 hours. Intravenous antibiotics are given for 24 hours post-operatively. All patients are placed in short-leg casts and made non-weight-bearing for an average of three weeks post-operatively with an additional three weeks spent in a walking cast thereafter. Routine removal of hardware is not performed, as is done in some centres.
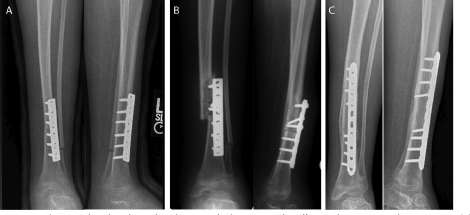
Example of a patient with spina bifida whose hardware failed catastrophically 30 days after index surgery: (
After identification of participants, charts were reviewed for demographic information, direction of derotation, correction achieved (in degrees) at index surgery, incidence of complications, type of complication, as well as the need for re-operation. Complications included in analysis were superficial infection, deep infection/dehiscence, fracture, hardware failure and removal of hardware for any reason. Removal of hardware was performed only in patients with symptomatic hardware and was included as a complication because it necessitated a return to the operating room. Two-sample T-tests were used to compare the characteristics of the two groups. Descriptive statistics were used to determine the incidence of complications as well as need for re-operation, and two-tailed chi-square tests were used to compare incidence of complications between cohorts. Generalised linear logit models were used to identify independent risk factors for complication and need for re-derotation among the two cohorts.
Results
Demographics and surgical characteristics
A total of 153 patients - 64 of whom underwent bilateral osteotomies - met the criteria for inclusion, for a total of 217 limbs. Of these, 64 patients (82 limbs) had CP and 89 (135 limbs) had myelodysplasia. In total, 88 male and 65 female patients were included for analysis. Of those with spina bifida, 36 (40.45%) had L4 and proximal levels of involvement and 53 (59.55%) had L5 or sacral levels of involvement. Of those with CP, 36 (56.25%) were classified as GMFCS I or II and 28 (43.75%) were classified as GMFCS III or IV. Average age at index surgery was older in the cohort with CP compared with those with myelodysplasia (12.47 vs 9.33, p < 0.0001), with a resultant longer average follow-up for those patients with spina bifida (8.57 years (2.35 to 18.78) vs 6.76 years (2.05 to 18.76)) (Table 1).
Patient characteristics stratified by disorder.
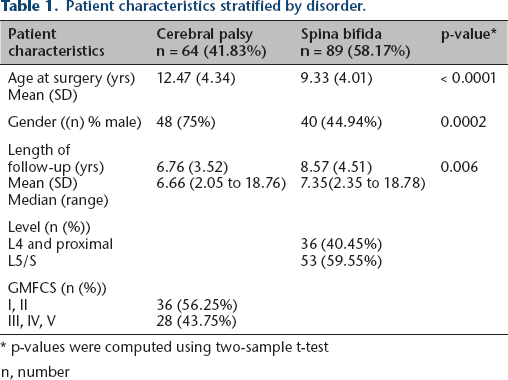
p-values were computed using two-sample t-test n, number
Of those with spina bifida, 54 (40%) had surgical correction of internal tibial torsion and the remaining 81 (60%) had correction of external tibial torsion. The average derotation was 28.90° (± 7.39°), which was maintained at 26.14° (± 12.49°) of correction at final follow-up. In those with CP, 17 (20.73%) had surgical correction of internal tibial torsion and the remaining 65 (79.27%) had correction of external tibial torsion. The average derotation was 26.37° (± 6.20°), which was maintained at 24.07° (± 7.22°) of correction at final follow-up. Taken together, the average derotation achieved was 27.94° (± 7.06°) and was maintained at 25.36° (± 10.84°) of correction at final follow-up. The majority of tibial osteotomies (78.3%) were completed in conjunction with other lower extremity surgeries for functional malalignment and limitations in range of motion affecting the femur, foot, hip, knee or ankle joint. Concomitant surgeries included lower extremity tendon/muscular lengthening and/or femoral/pelvic osteotomies, which included 31 (14.3%) tendo-achilles lengthenings/gastrocnemius recessions, 40 (18.4%) soft tissue procedures in the foot, 25 (11.5%) corrective osteotomies or fusions in the foot, and 32 (14.7%) concomitant ipsilateral femoral derotational osteotomies, between both groups.
Complications
All patients went on to union despite ten tibiae (4.61%) that required prolonged casting (more than ten weeks) for delayed union (without fracture). Those patients that were casted more than ten weeks were evenly divided between the studied cohorts. The average time spent in a cast was 7.04 weeks (± 1.93 weeks) for all patients, which was, on average, shorter for patients with CP (6.63 weeks ± 1.62) compared with those with spina bifida (7.29 weeks ± 2.07) (p = 0.204). Cast removal was performed when there was evidence of consolidation at the osteotomy site and is being reported as a surrogate for osteotomy healing time, as this specific data point was not available from chart review.
The overall incidence of complication was 10.14%, including removal of hardware for any reason, with a 4.61% incidence of major complication including fracture, deep infection and hardware failure (Fig. 1, Table 2). All complications were Clavien-Dindo grades I-III, without any Clavien-Dindo grades IV or V. Five complications were classified as Clavien-Dindo grade I (one CP, four myelodysplasia), eight as Clavien-Dindo grade II (all myelodysplasia) and nine as Clavien-Dindo grade III (four CP, five myelodysplasia). While patients with spina bifida had higher overall complication rates than those with CP (12.6% vs 6.1%), this did not reach statistical significance (p = 0.125). Further, there was no statistically significant difference between groups when comparing major complication rate after adjusting for gender and age (odds ratio = 0.424, 95% confidence interval = 0.086 to 2.103, p = 0.292). Age at initial surgical intervention had no effect on complication rate (p = 0.798).
Complications stratified by disorder (unadjusted).
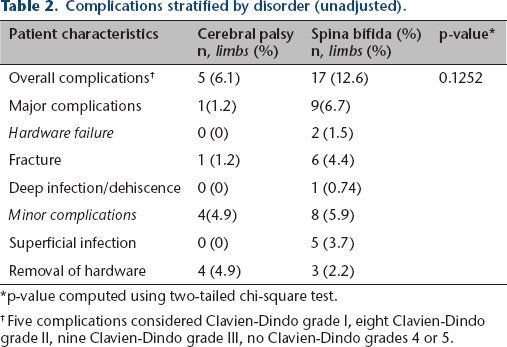
p-value computed using two-tailed chi-square test.
Five complications considered Clavien-Dindo grade I, eight Clavien-Dindo grade II, nine Clavien-Dindo grade III, no Clavien-Dindo grades 4 or 5.
Re-derotational surgery
A total of 22 limbs (10.14%) required re-derotational surgery - 21 in the myelodysplastic population (15.6%) and one in the CP cohort (1.2%). Indications for re-operation were the same as for index surgery - tibial torsion affecting gait biomechanics, velocity and/or orthotic wear. In unadjusted analysis, the risk of re-rotation requiring surgery was 93.3% less likely for patients with CP compared with those with spina bifida (0 = 0.01). However, after adjusting for age and gender, there was no statistically significant difference in re-rotation risk between the two cohorts (p = 0.093).
The odds of requiring re-derotational osteotomy were 31.9% less likely per year increase in age at index surgery (p = 0.0048) after adjusting for disease group, gender, direction corrected and magnitude of correction. This was independently true for both cohorts. Length of follow-up was comparable between those that required re-derotation and those that did not (7.38 years vs 7.58 years, on average). Resultantly, this variable was not directly controlled for in this model. There was no association between degree of initial rotation and need for re-derotation (p = 0.608), nor was there an association between direction of rotation and need for re-derotation (p = 0.278). However, there was a trend toward over-correction following external derotational osteotomies (7.1%) and under-correction following internal derotational osteotomies (6.3%) at final follow-up. Neither GMFCS nor neurologic level of involvement reached statistical significance in predicting need for re-derotational osteotomy in each respective cohort.
Discussion
While the aetiology of rotational abnormalities in children with CP and spina bifida are dissimilar, the effect of tibial torsion on children with overall poor musculoskeletal control and weakness results in similar natural history, progressive deformity and resultant disability. Both internal and external rotational deformities can significantly alter standing tolerance and gait patterns in patients with CP and spina bifida wherein surgical correction is necessary to maintain and/or improve ambulatory status. In fact, previous authors have reported significant improvements in gait kinematics and kinetics in both populations following TDO.10,11
Further, despite dissimilar underlying disease processes, response to surgical management of tibial torsion in terms of complications and need for re-derotational osteotomy are similar between populations when using our previously published surgical technique. 19 This method results in an overall acceptable complication rate of 10.14% and a major complication rate of 4.61%, with no appreciable difference in major complication risk between groups. Further, the overall risk of need for re-derotational surgery in this population was 10.14%, with a negative linear relationship between age at index surgery and need for re-derotational osteotomy in both groups.
Theoretically, the myelodysplastic population would be expected to have significantly higher complication rates given the underlying disease process and resultant lack of protective sensation. Likewise, the overall muscular imbalance in the CP population could theoretically increase this cohort's risk for re-rotation. Yet, we did not find any appreciable difference in major complication or need for re-derotation rates between groups. We attribute this relatively consistent complication and re-operation rate to our surgical technique: metaphyseal level osteotomy, the use of drill holes and osteotome to reduce osteonecrosis with osteotomy, rigid fixation and compression at the osteotomy site, concomitant fibular osteotomy and the use of non-absorbable, interrupted sutures for closure over a drain. While many experienced neuromuscular orthopaedic surgeons do not routinely perform concomitant fibular osteotomies in every case, we believe that consistently performing a fibular osteotomy does not increase complication risk or add significant time or complexity to the case. Further, we believe that the addition of the fibular osteotomy better preserves the relationship of the syndesmosis and likely contributes to the durability of our results compared with previously published series in which fibular osteotomies were not routinely performed.
Furthermore, in direct comparison to previously published complication rates following TDO in neuromuscular populations, we report an overall favourable major complication rate for this population (4.61 vs 5.3%). 14 Notably, there was a statistically insignificant trend toward higher complication risk in our spina bifida population compared with our CP population, as would be expected. However, this complication rate (12.6%) remains lower than those of earlier reports (28% to 33%)1,4,18 in isolated populations of spina bifida. It is additionally important to note that if removal of hardware was not included as a complication, the CP population would have an overall complication rate of only 1.2% compared with 10.4% in the myelodysplastic population, but the major complication rate would remain constant in both groups.
In addition to our low complication rate, both studied populations had relatively low re-derotation rates (overall 10.14%). In contrast to these findings, two recent publications reported high rates of late over-correction following external TDOs 23 and high rates of late under-correction following internal TDOs 20 in patients with CP. With an average follow-up of 7.83 years (2.05 to 18.78), we found more durable results following both internal and external rotational osteotomies in both populations. However, there was a noted trend toward over-correction following external derotational osteotomies (overall 7.14% of patients) and under-correction following internal derotational osteotomies (overall 6.31% of patients) in our cohort. These trends paralleled those reported by Er et al, but were significantly smaller in magnitude (56% and 58%, respectively)20,23 despite similar length of follow-up. We attribute these durable, long-term results to our inclusion of a concomitant fibular osteotomy in all cases and our use of rigid internal fixation.
While diagnosis, degree of derotation and direction of derotation did not directly affect the incidence of rerotation, there was a statistically significant association between age at surgery and need for re-derotation. The risk for re-derotational osteotomy was 31.9% less likely per year increase in age at index surgery following both internal and external rotational osteotomies, independent of degree of initial derotation, diagnosis or gender. While our overall results were durable in achieving long-standing correction in the majority of patients, younger children have great remodelling potential regardless of surgical technique and mode of fixation. And while this remodelling potential with an associated high re-operation incidence has been previously reported,18,23 this report is the first to stratify risk of recurrence by age at index surgery, which may be helpful for operative planning and pre-operative counselling.
Although this is the first direct comparison between myelodysplastic patients and children with CP following TDO, it was limited primarily by its retrospective nature. Given the limitations of a retrospective review, data were insufficient to determine accuracy or inter-observer error. However, this has been previously described in similar studies. 11 In addition, concomitant surgeries were not taken into consideration nor controlled for. Given that many children with neuromuscular diseases and tibial torsion require multiple surgeries for lower limb deformity and gait disturbance and that many of these surgeries are performed simultaneously, it was clinically irrelevant to control for the possibility of concurrent soft-tissue procedure or concomitant lower extremity osteotomies. Further, we do not report on functional or subjective outcomes data including gait analysis data. However, previous reports, including that of the senior author (LD), have previously demonstrated improvements in gait parameters following derotational osteotomy for tibial torsion in similar populations.10,11 And while our average follow-up was 7.83 years, our cohort included patients with as little as two years of follow-up, which may have led to an under-representation of late recurrences in these patients. Lastly, the study cohort is limited to the patients that were operated on during the included time period and, as a result, we may be underpowered to answer all clinical questions. However, this remains the largest series of TDOs secondary to a neuromuscular disease process reported in the literature to date.
Despite limitations, given the relatively favourable, consistent complication profile as well as the short-term and presumed long-term benefits of TDO for tibial torsion in patients with myelodysplasia and cerebral palsy, TDO should be strongly considered for patients with appropriate indications. While we previously reported similarly encouraging results in a purely myelodysplastic population, this comparison further reflects the safety and efficacy of TDO using rigid internal fixation and concomitant fibular osteotomy for children with non-idiopathic tibial torsion.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Each listed author declares that he/she has no conflicts of interest. This study received no external or internal funding. All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Institutional Review Board, and given the retrospective nature of the study, a waiver of informed consent was granted.