
Abstract
Purpose
This study aimed to determine the incidence of acetabular dysplasia at six months of age in patients with breech presentation and previously normal hip ultrasounds, reporting primary radiographic measurements to allow for comparison with other patient cohorts.
Methods
A retrospective analysis of breech infants with initially normal clinical examinations and hip ultrasounds was performed to determine the rate of subsequent acetabular dysplasia and to characterise the distribution of acetabular index (AI). At approximately six months of age, AI was measured bilaterally on anteroposterior (AP) pelvic radiographs and reported using descriptive statistics.
Results
A total of 94 hips in 47 breech infants were eligible for analysis. All infants demonstrated normal ultrasound findings at a mean age of 6.9 ± 1.7 weeks and returned for follow-up at a mean age of 6.4 ± 0.5 months. On AP pelvic radiographs, mean right hip AI was 25.0°, with an interquartile range (IQR) (25th -75th percentile) of 23° to 27° and mean left hip AI was 25.5°, with an IQR of 22° to 28°. If one applies a single commonly used threshold value for defining dysplasia (AI ≥ 30°), 10/94 hips (10.6%) meet diagnostic criteria. Alternatively, strict adherence to previously established normative AI values stratified by gender and laterality results in 4/94 hips (4.3%) qualifying as significantly dysplastic.
Conclusions
The proportion of breech infants who, despite normal initial ultrasound findings, were diagnosed with dysplasia at six months supports observation of breech-born patients beyond six weeks. Reliance on different threshold values for diagnosing acetabular dysplasia can lead to discrepancies in incidence rates.
Introduction
Breech presentation is an important risk factor for developmental dysplasia of the hip (DDH), with breech newborns having an estimated incidence of neonatal hip instability ranging from 12% to 24%.1,2 Even with normal hip exams, babies born in breech position are typically referred to paediatric orthopaedic surgeons for clinical examination and hip ultrasound to identify patients with more subtle forms of DDH. 3 For those with normal clinical and ultrasound findings, the risk of subsequent dysplasia at an older age and the need for further follow-up remain poorly defined. While early identification of acetabular dysplasia may allow for timely intervention with less expensive and less complex treatment measures,4,5 the burden of continued follow-up radiographs and clinic appointments for all breech infants can be substantial. Essential to understanding the value of continued observation of this patient cohort is an accurate estimation of the incidence of subsequent acetabular dysplasia. Previous studies assessing this population have relied on various threshold values for diagnosing dysplasia without reporting primary radiographic measurement data.1,2,6 Such variability may be responsible for discrepancies in reported incidence rates. The purpose of this study was to determine the incidence of acetabular dysplasia at six months of age in patients with breech presentation and previously normal hip ultrasounds, reporting primary radiographic measurements to allow for comparison with other patient cohorts.
Patients and Methods
Approval for this investigation was granted by our Institutional Review Board. At our tertiary-care paediatric center, breech infants with normal ultrasound imaging during early infancy continue to be observed and return for follow-up clinical examination and plain radiographic evaluation at approximately six months of age. Those who are considered to have acceptable radiographic indices at that age are discharged from care. Those with radiographic findings of hip dysplasia at six months of age, which we define using the traditional single threshold of acetabular index (AI) ≥ 30°, are treated with abduction bracing and followed further. We performed a retrospective analysis of these breech infants with initially normal clinical and ultrasound findings to determine the rate of subsequent acetabular dysplasia and to characterise the distribution of AI. A list of patients was generated from a query of our institution's billing records using the ICD-9 code 763.0 over a six-year interval. A manual review of electronic medical records and an electronic medical imaging database (iSite Enterprise software; Phillips, Amsterdam, Netherlands) was performed to determine patient eligibility. Inclusion criteria consisted of infants with breech presentation, normal initial clinical examination, and normal ultrasound as defined by Graf 〈 angles α 60° bilaterally and femoral head coverage ≥ 50% bilaterally. Exclusion criteria included presence of an underlying diagnosis, treatment with Pavlik harness, or absence of relevant imaging data.
At approximately six months of age, the AI for each hip was measured by the first author on digital supine anteroposterior (AP) pelvic radiographs using standard PACS (Picture Archiving and Communication System) software tools. As described previously,5,7,8 AI was measured by first drawing Hilgenreiner line, a horizontal line connecting the superior aspects of both hips’ triradiate cartilages. A tangential line was drawn along the boney edge of the acetabulum that connects the superolateral margin of the ossified acetabulum with the superolateral margin of the triradiate cartilage. The angle formed between these two lines was measured as the AI.
For a subset of 40 hip joints selected at random, AI measurements were repeated by the same observer six months after initial measurements. Intraclass correlation coefficient (ICC) calculations were performed to assess the level of intra-observer reliability, with ICC > 0.8 indicating almost perfect agreement between two measurement sets.
Descriptive summary statistics were used to report AI data. The Shapiro-Wilk test was performed to determine if the data were normally distributed. Data with non-normal distribution was reported by the interquartile range (IQR) (25th to 75th percentiles). Population means of acetabular indices as reported by Tönnis et al 9 were used as normative data for considering differing threshold values to diagnose acetabular dysplasia. The traditional single threshold of AI ≥ 30°, approximately two standard deviations above the population mean, was used to guide treatment decisions.
Results
A total of 94 hips in 47 breech infants (38 female, nine male; 17% with family history of DDH) were eligible for analysis. Infants were seen for initial visit at a mean age of 6.9 ± 1.7 weeks. Among this cohort of patients with normal ultrasound findings, mean alpha angle of the left hip was 66.3°, with an IQR of 62° to 70°. Mean alpha angle of the right hip was 66.0°, with an IQR of 62° to 70°. On follow-up AP pelvic radiographs performed at a mean age of 6.4 ± 0.5 months, mean AI of the right hip was 25.0° (IQR 23°-27°) and mean AI of the left hip was 25.5° (IQR 22° to 28°) (Fig. 1). AI values of D(94) = 0.945, p < 0.05 demonstrated significant deviation from a normal distribution. The ICC calculated on the subset of 40 hips whose AIs were re-measured by the same observer six months after initial measurement was 0.984, indicating excellent agreement.
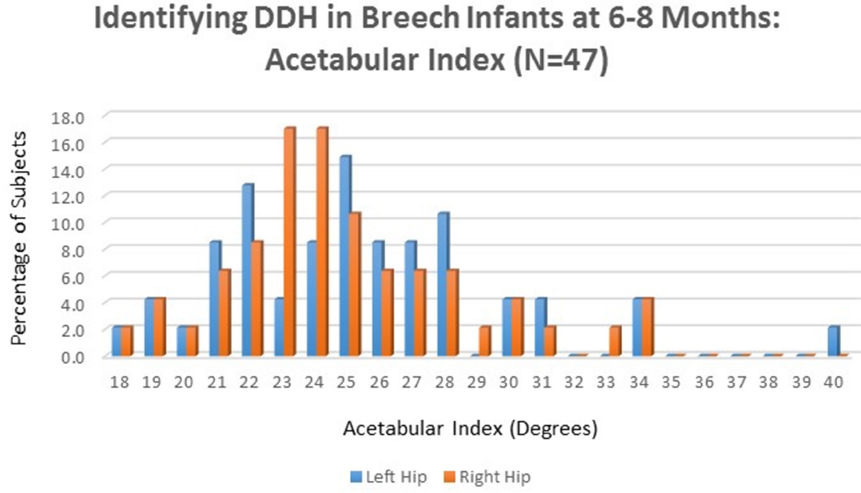
Identifying developmental dysplasia of the hip in Breech Infants at six to eight months.
Applying the traditionally used single threshold value for diagnosing acetabular dysplasia at this age (AI ≥ 30°), 10/94 hips (10.6%) met diagnostic criteria. These ten dysplastic hips were comprised of five patients with bilateral dysplasia, who were treated with abduction bracing and followed further. Alternatively, Table 1 stratifies the patient cohort by gender and laterality, providing differing rates of acetabular dysplasia as defined by both one and two standard deviations above each sub-group mean as originally reported by Tönnis et al. 9 Applying this stratified normative data results in 19/94 (20.2%) hips with an AI that is one standard deviation above the population mean and 4/94 (4.3%) hips with an AI that is two standard deviations above the population mean (Fig. 2). The calculated incidence of acetabular dysplasia varied widely depending on which diagnostic threshold was applied (4.3% vs 10.6% vs 20.2%) (Table 2).
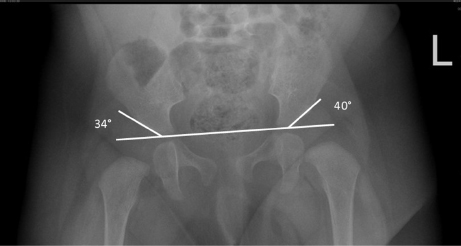
Anteroposterior pelvic radiograph taken of a patient at six months old demonstrating acetabular dysplasia in a breech infant who previously had a normal US at four weeks of age. This patient was treated with hip abduction brace.
Percentage of patients meeting the criteria for acetabular dysplasia per Tönnis et al. 9
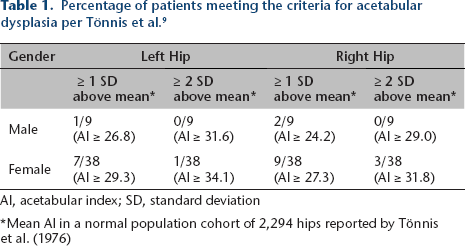
Al, acetabular index; SD, standard deviation
Mean AI in a normal population cohort of 2,294 hips reported by Tönnis et al. (1976)
Variable criteria for diagnosing acetabular dysplasia produce vastly difference incidence rates.
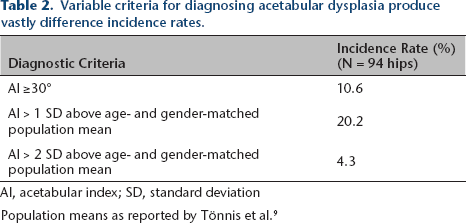
AI, acetabular index; SD, standard deviation
Population means as reported by Tönnis et al. 9
Discussion
Recognised risk factors for DDH include a positive family history, a positive newborn hip examination, and breech presentation.2,10 More subtle forms of dysplasia not detected in childhood or adolescence can contribute to the long-term development of osteoarthritis with sequelae of joint pain, impaired function, decreased quality of life, and increased need for surgical intervention as an adult. 11 Early identification of mild acetabular dysplasia may allow for timely intervention to improve acetabular morphology through non-operative means. 5 Thus, it is imperative to establish an evidence basis for the clinical decision to discontinue routine follow-up in babies born with risk factors for DDH.
Several authors have previously recommended no further follow-up for patients with risk factors and normal ultrasound screening examination. In cohorts of 89 and 181 patients respectively, Arumilli et al 12 and Osarumwense et al 13 demonstrated that no newborns with a family history of DDH and normal ultrasound findings at six weeks required intervention at 12 months follow-up. Jellicoe et al 14 reported that among a cohort of 139 at-risk infants (not limited to breech presentation) with normal ultrasound findings, all patients who returned at 12 months exhibited normal findings on radiographs. In addressing breech presentation specifically, Imrie et al 6 found that, among 193 breech newborns with normal clinical and ultrasound findings at six weeks, 29% had radiographic and/or clinical evidence of hip dysplasia at four to six months follow-up. Our study of breech infants reports a lower, yet meaningful proportion (4.3% to 10.6%) of patients that met diagnostic criteria for acetabular dysplasia at six month follow-up. This study's findings corroborate the practice described by Imrie et al 6 of continued monitoring of patients with breech presentation even after normal findings at six weeks of age.
It is important to consider that previous reports on the incidence of acetabular dysplasia in infants with DDH or risk factors for DDH suffer from heterogeneity in diagnostic criteria. This issue stems, in part, from a lack of primary radiographic measurements in early studies establishing normative values for acetabular index in children. For example, in the highest quality study to date assessing acetabular dysplasia in breech infants with initially normal sonographic imaging, Imrie et al 6 relied on age-matched controls as reported by Scoles et al 15 However, in this original study, Scoles et al 15 do not explicitly report mean AI and standard deviations for each age group they evaluated, nor do they report whether AI values were normally distributed within each age group assessed. In order to apply strict AI cutoff values for diagnosing hip dysplasia at six months of age, we used primary data from Tönnis et al 9 to provide an age-matched control group. By reporting the primary AI values and distribution in our cohort, we aim to encourage other authors addressing this question to apply this strategy to facilitate direct comparison and meta-analysis of study data.
Additionally, it is noteworthy that in the classic report of normative values for acetabular indices at different ages, Tönnis et al 9 stratify data not only by age, but also by gender and laterality. It is our experience that these gender and laterality-based criteria are not applied in routine clinical practice and instead a single threshold value is usually favored. While it may be easier for clinicians to apply a single threshold value for making a treatment decision, the discrepancy between this and the original normative data, as well as the varying incidence rates reported in the present study (Table 2), highlight the flawed manner in which we determine what constitutes abnormal hip development.
Our findings must be considered within the context of the study's limitations. Our results reflect a retrospective review of patients at a single institution, and may therefore not be generalisable to all populations with differing ethnic distributions. In addition, measurement error of the acetabular index may have contributed to study error.8,16 However, measurement of AI with digital radiographs (as in the present study) has been shown to have a high rate of reproducibility and accuracy, including a 2-° to 3-° intra-observer error and a 0- to 1-° interobserver variance. 17 Further, while our institution routinely re-images patients when the treating physician deems the radiograph to be of poor quality or with excessive pelvic rotation or tilt, no quantitative assessment of pelvic rotation or inclination was performed in the current analysis. Finally, the purpose of this study was only to evaluate the incidence of dysplasia at six months of age in breech infants with previously normal hip ultrasounds, and it has been our practice to discharge infants from further follow-up after two normal imaging studies. As a result, we cannot comment on the longer-term natural history of breech infants. Those hips that we did consider to be dysplastic were treated with part-time abduction bracing, which has been shown to be effective for improving the acetabular index. 5 As Imrie et al 6 asserted, we cannot exclude the possibility that patients’ still-developing hips may normalise without treatment, but the authors consider it difficult to withhold brace treatment from a patient population for which therapy may potentially provide a clinical benefit.
In summary, the significant proportion of breech infants who, despite normal initial ultrasound findings, were later diagnosed with dysplasia supports continued observation of breech-born patients for at least six months regardless of ultrasound findings in early infancy. However, reliance on differing threshold values for diagnosing acetabular dysplasia can lead to wide discrepancies in reported incidence rates. The acetabular indices reported in this series for breech infants following initially normal ultrasound may be used for direct comparison with other cohorts of similar infants.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
No funding was received for this study.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: An institutional review board granted a waiver of informed consent due to the minimal risk involved for subjects. The research was conducted after IRB approval
Acknowledgement
We thanks Divya Talwar, PhD, MPH of The Children's Hospital of Philadelphia for her support with statistical analysis