
Abstract
Purpose:
Some articles have focused on the effectiveness of the Pavlik harness treatment for unstable and dislocated hips, yet data on monitoring its effectiveness with the acetabular index remains elusive. Therefore, this study aimed to assess Pavlik harness effectiveness in infants ≤6 months diagnosed with grade I developmental dysplasia of the hip using acetabular index improvement and identify the possible predictors of successful Pavlik harness treatment.
Methods:
A retrospective review of infants with grade I acetabular dysplasia treated with a Pavlik harness and monitored with anteroposterior pelvis X-rays at presentation and follow-up. Successful treatment was defined as achieving an acetabular index <30°.
Results:
A total of 231 infants with acetabular dysplasia were treated with a Pavlik harness. A successful outcome was achieved in 135 infants (58.4%). Younger age, lower initial acetabular index, and patients with unilateral developmental dysplasia of the hip were significant predictors of a successful outcome. An age of 4.5 months or older was found to be the threshold for an unsuccessful result following Pavlik harness treatment, with a sensitivity of 65.2% and specificity of 57.3%. An initial acetabular index of 35.5° was found to be the threshold for an unsuccessful result, with a sensitivity of 83.7% and specificity of 61.5%.
Conclusion:
Pavlik Harness’s success in correcting the acetabular index in acetabular dysplasia patients was related to unilateral cases, a younger age at presentation, and a lower initial acetabular index. The thresholds for unsuccessful treatment were an age of 4.5 months or greater and an acetabular index of 35.5° or higher.
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is a well-defined disorder related to the development of the acetabulum, varying in severity from asymptomatic dysplasia to dislocation.1 –3 Sonographic DDH incidence was reported in a large study that included 18,060 hips at 55.1 per 1000; however, the true DDH incidence was 5 per 1000 hips, this might vary depending on screening protocols and study populations. 4 In a meta-analysis, the risk factors for developing DDH were breech presentation, female gender, left side hip, first pregnancy, and family history, with a relative risk of 3.75, 2.54, 1.54, 1.44, and 1.39, respectively. 5 However, most patients affected by DDH do not appear to have any risk factors,6,7 and some studies suggest that these risk factors are poor predictors of DDH.8,9
Screening for DDH is widely variable and has a diverse group of guidelines across different countries.3,10 –12 Ultrasonography using Graf’s method is one of the most commonly used screening tools, 13 yet, there is no consensus regarding its use as a screening tool. 14 Universal screening for all infants is performed in some countries, such as Germany, Switzerland, Austria, and Italy. Whereas others, like France and the United Kingdom, do selective screening only for infants with risk factors. 15 Meanwhile, in Asia, the introduction of universal screening for DDH for the first time was in 2017 in Mongolia. 16 The lack of training and equipment availability are reported barriers to ultrasound utility in low-resource countries. 17 These might affect the application of ultrasound screening for DDH, as implementing an ultrasound screening policy is determined by the resources, expected outcomes, and available budget. 18 There is no national screening program in Jordan. However, with the increasing awareness among families and physicians, 19 it has become common practice to screen all infants aged 3–4 months using plain pelvic radiographs even in the absence of physical signs and risk factors. Similar screening practices yielded substantial public health benefits and resulted in a lower number of major procedures performed for DDH cases in Chile, considering it an appropriate method to evaluate DDH in regions with limited resources. 20 Excluding patients with a hip dislocation/subluxation, the main parameter used to diagnose DDH on X-ray is the acetabular index (AI), which was first described in 1936. 21 It is the most useful for detecting dysplasia 22 and has good to excellent reliability in monitoring treatment. 23 Nakamura et al. 24 demonstrated that, in a mean follow-up of 16 years, AI was the most reliable predictor of residual acetabular dysplasia, as AI < 30° correlated with favorable long-term outcomes.
Acetabular dysplasia encompasses morphological abnormalities in the acetabulum, which can lead to shearing forces between the acetabular rim and the femoral head. 13 This might stress and eventually damage the cartilage since the articular surfaces are still in contact.22,25,26 Dysplasia in infants under the age of 6 months can be treated with Pavlik harness (PH), which is the most commonly used device. Many other alternatives exist and are widely used, examples include Craig, Von Rosen, and Tübingen splints.27,28 PH maintains the hips in a position of flexion and abduction while still allowing motion, thus promoting normal development of the acetabulum.
The success of PH treatment for unstable and dislocated hips has been the subject of a few articles,10,29 but little is known about its effectiveness in treating asymptomatic dysplasia, particularly when the AI is used as a monitoring tool. In this article, the aim was to investigate PH effectiveness in treating asymptomatic acetabular dysplasia diagnosed by plain radiograph in infants below 6 months, to pinpoint the most important factors contributing to treatment success and to optimize treatment approaches.
Methods
Study design
This retrospective study was conducted at the orthopedic unit of a 600-bed tertiary referral university hospital on patients diagnosed with DDH. We retrospectively reviewed the pediatric orthopedics clinic’s electronic medical records from 2016 to 2019. Our cohort tackled patients aged 3–6 months diagnosed with grade I using the AI and treated with a PH. The acetabular dysplastic subtype was defined as grade I according to the International Hip Dysplasia Institute’s (IHDI) classification, 30 and these were completely reduced hips with an abnormal AI on pelvic X-ray. Children who were not treated with a PH, had suboptimal image quality, or were lost to follow-up were excluded. In addition, subluxated or dislocated DDH cases were not included in our cohort, as the primary goal in such cases is achieving concentric reduction first. The main aim of the study was to identify contributing factors to treatment success and optimize treatment approaches.
The appropriate institutional review board (IRB) of the Jordan University Hospital (JUH) approved the proposal for this study. The Code of Ethics of the World Medical Association (Declaration of Helsinki) was followed while conducting the study. Informed written consent was obtained from the patients.
Data collection process
Data collected included age at presentation in months, gender, duration of PH treatment in weeks, and additional non-surgical or surgical treatment modalities. In addition, the AI of both hips was measured for all cases on all occasions by one consultant pediatric orthopedic surgeon and two senior orthopedic surgery residents on the same imaging system and measurement tools using the Picture Archiving and Communication System (PACS). Senior residents were reliable to assess AI, as in a previous study at the same institution, the interobserver reliability intraclass correlation coefficient (ICC) for AI measurement by senior residents in comparison with orthopedic surgeons was good to excellent (0.904 and 0.88) for the right and left hip readings, respectively, 31 these numbers are based on different images than the ones used in this article.
Diagnosis and treatment protocol
All patients were subjected to the same modality of diagnosis and treatment. A physical examination, including a general orthopedic and hip examination, was done by a consultant pediatric orthopedic surgeon. Then, an anteroposterior pelvic radiograph was taken for all children for screening. The X-rays were taken by two senior radiological technicians with the hips in 15 degrees of internal rotation and abduction to offset any pseudo-subluxation potentially created by adducting the hips, and gonadal shielding is advised at our institution to reduce the radiation risk. All patients had an intact Shenton’s line at presentation, indicating concentricity of the hips. The AI is the angle formed between Hilgenreiner’s line and a tangential line drawn from the triradiate cartilage to the lateral border of the acetabulum. 21 Figure 1 illustrates the measurement technique of the AI on an anteroposterior pelvic radiograph. The AI was considered abnormal, and patients were put on PHs if it was equal to or above 30 degrees in either one or both hips.32,33 The first follow-up visit was done after 1 week to check the adequacy of PH application/position and femoral nerve function as well as to address any parental concerns. Then, all patients had serial follow-up visits every 6 weeks with a new X-ray to assess improvement.
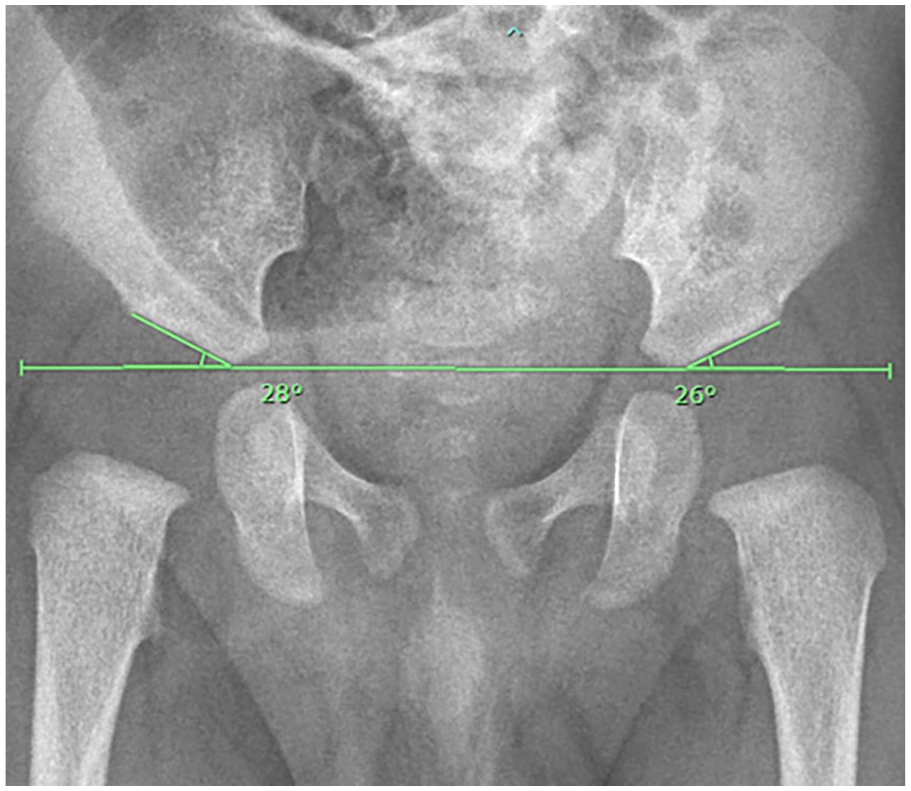
The measurement of the acetabular index (AI) on an anteroposterior pelvic X-ray. The horizontal line demonstrates the Hilgenreiner’s line.
Treatment was considered successful if the AI angle decreased to less than 30 degrees, which was defined according to the previous literature. NH Harris 34 considered an AI of 30° to be the upper limit for normal hip development at the age of 1 year. In addition, D Tönnis 32 reported that an AI of 30° at 1 year of age exceeded the range of 2 standard deviations (SD). The paper’s curves implied that an AI of 30° is within the 2 SD range for a child aged 6–7 months, whereas the mean value for infants aged 3–4 months is approximately 25°. This indicates that an AI of 30° at 1 year is relatively higher than the average values observed at younger ages. In patients with bilateral DDH, the treatment was successful if the AI of both hips became less than 30 degrees. Treatment was considered unsuccessful if the AI remained ≥30 degrees and/or required further non-surgical or surgical treatment.
The PH was applied to all infants by an experienced orthopedic technician under the supervision of the consultant pediatric orthopedic surgeon, with the posterior straps tightened to prevent adduction beyond a neutral position and the anterior straps holding the hips in flexion between 90° and 100°. The parents were given extensive instructions on the use of PH for at least 23 h a day and the importance of compliance for DDH improvement. In addition, frequent follow-up visits were scheduled to assess the size of PH and radiological improvement.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, version 28.0 (Chicago, USA). We summarized the characteristics of the sample using the count (frequency) to describe the categorical variables and the mean and standard deviation to describe the continuous variables. The results of Pavlik treatment were assessed in binary outcome groups (successful or unsuccessful). A chi-square test was performed to detect differences in treatment outcomes associated with age groups, gender, and bilaterality. An independent sample t-test was used to compare outcomes between continuous variables. Variables that showed potentially interesting associations from the univariate analysis were included in the binary logistic regression model in order to control for possible confounding factors, which were summarized using the adjusted odds ratio (AOR) (95% CI). A p-value < 0.05 was considered statistically significant.
The receiver-operating characteristic (ROC) curve analysis was used to determine the optimal cutoff scores. The optimal cutoff score was calculated using the Youden index (J), equal to the sensitivity plus specificity minus 1, which was maximized to quantify the cutoff values for the age and the initial AI. The accuracy of the test was measured by the area under the curve (AUC).
Results
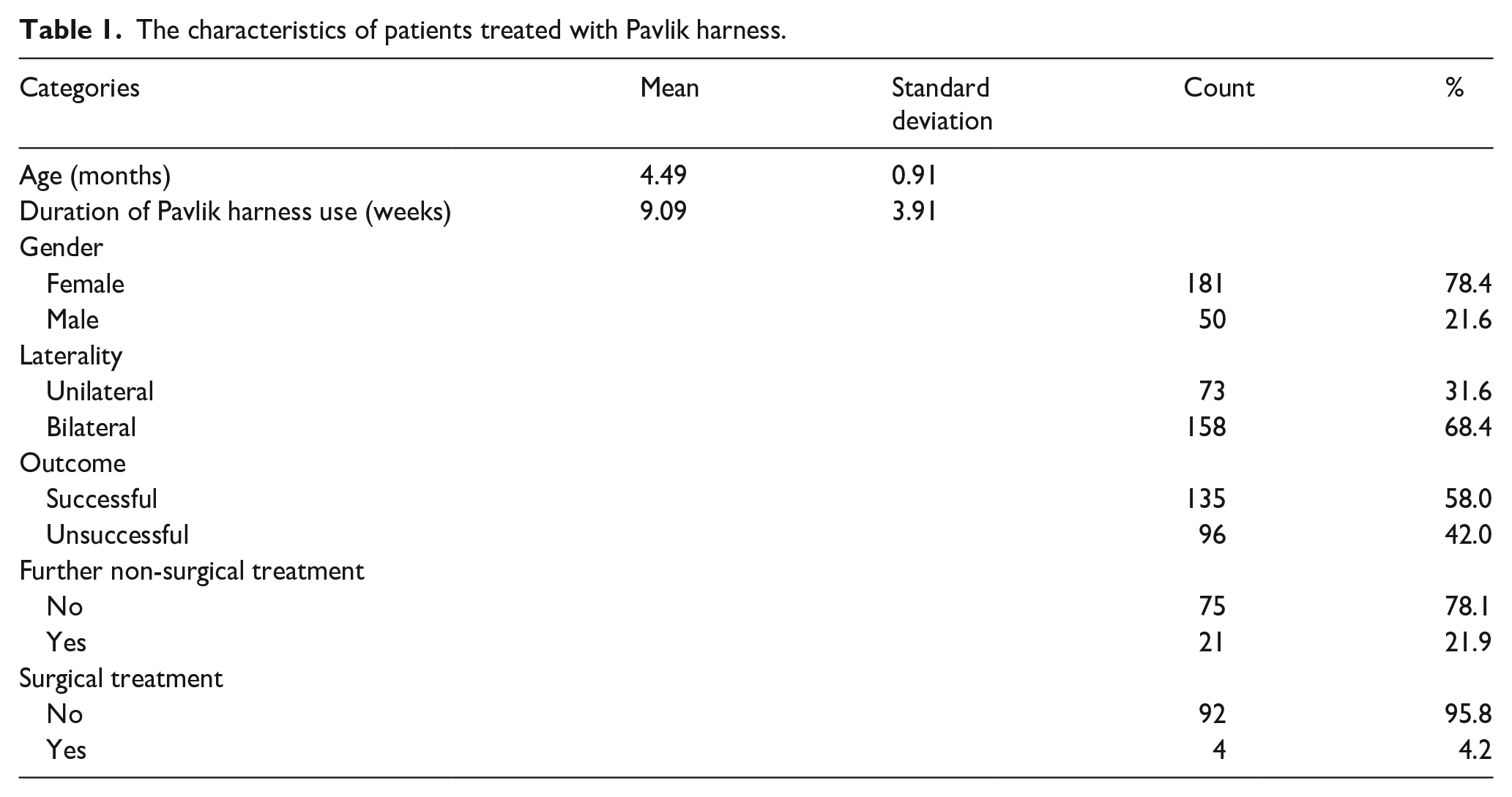
A total of 231 (389 hips) infants were included in the analysis. The infants were aged between 3 and 6 months and nearly three-quarters (78.4%) of the infants were female. The most common (42.2%) age of presentation was 4 months and the mean duration of the PH application was 9.09 ± 3.91 weeks. More than two-thirds (68.4%) of the 231 patients had bilateral DDH, resulting in a total of 389 hips (199 right, 190 left). Table 1 summarizes the characteristics of the infants.
The characteristics of patients treated with Pavlik harness.
Treatment with PH was successful in 135 (58.4%) patients. Of the 96 patients who had unsuccessful treatment, 21 had additional non-surgical treatment, and 4 had surgical treatment. Regarding the 96 patients who had unsuccessful treatment, the non-surgical treatment included different types of braces or spica castings based on the surgeon’s assessment and the degree of residual dysplasia. The surgical treatment was for the patient, who was followed up until the age of 1½ years and had significant residual dysplasia; therefore, they underwent some sort of pelvic osteotomy for correction. The patients who did not undergo further treatment were either because the residual dysplasia was minimal, they were regularly followed up, and they showed some improvement over time, but they might undergo surgery when they are older if necessary.
Our results showed a significant mean difference between the treatment outcome groups (unsuccessful and successful groups) and patients’ age (p < 0.001), with an age mean difference of 0.54 higher in the unsuccessful outcome group (95% CI = 0.30–0.77). We also found a significant difference in the duration of PH application (p < 0.001), with the unsuccessful outcome group showing a mean difference of 1.86 higher (95% CI = 0.86–2.86) than the successful outcome group. Furthermore, the initial AI displayed a significant difference (p < 0.001), with the unsuccessful outcome group having a mean difference of 3.21 higher (95% CI = 2.48–3.95) than the successful outcome group. In addition, the success rate was significantly higher in males (crude odds ratio (COR) = 2.74, 95% CI = 1.35–5.59, p = 0.004) and it was significantly lower in bilateral cases (COR = 0.30, 95% CI = 0.16–0.57, p < 0.001) (Table 2).
The association between the outcome of Pavlik harness treatment and the patient-related variables.
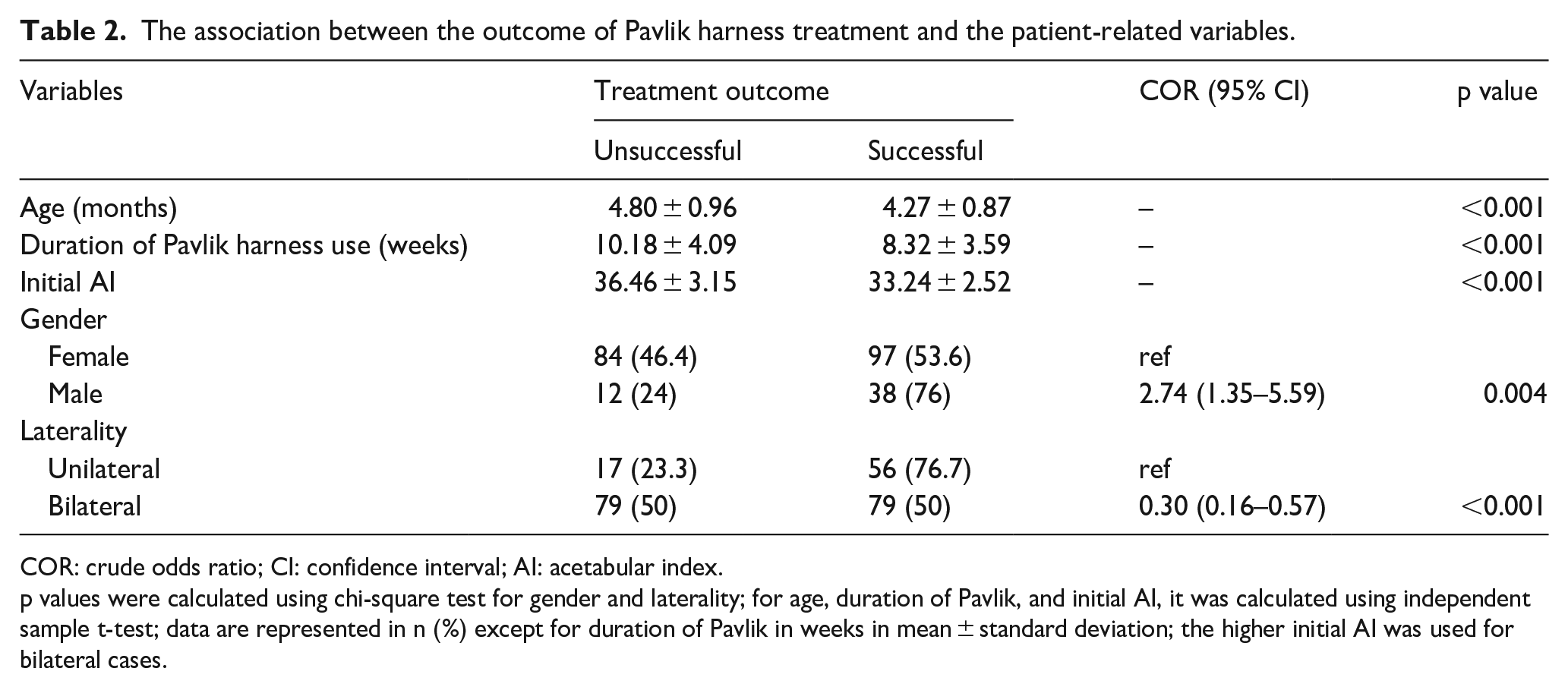
COR: crude odds ratio; CI: confidence interval; AI: acetabular index.
p values were calculated using chi-square test for gender and laterality; for age, duration of Pavlik, and initial AI, it was calculated using independent sample t-test; data are represented in n (%) except for duration of Pavlik in weeks in mean ± standard deviation; the higher initial AI was used for bilateral cases.
Table 3 shows multivariable logistic regression for the related variables that showed significant associations from the univariate analysis in order to control possible confounding factors. In the multivariable logistic regression analysis, it was found that the younger age at presentation (AOR = 0.43, 95% CI = 0.30–0.63, p < 0.001), initial AI (AOR = 0.70, 95% CI = 0.61–0.79, p < 0.001), and patients who had unilateral DDH (AOR = 0.40, 95% CI = 0.19–0.85, p = 0.018) were significant predictors for a successful outcome.
Multivariable logistic regression analysis for factors predicting success of Pavlik harness treatment.
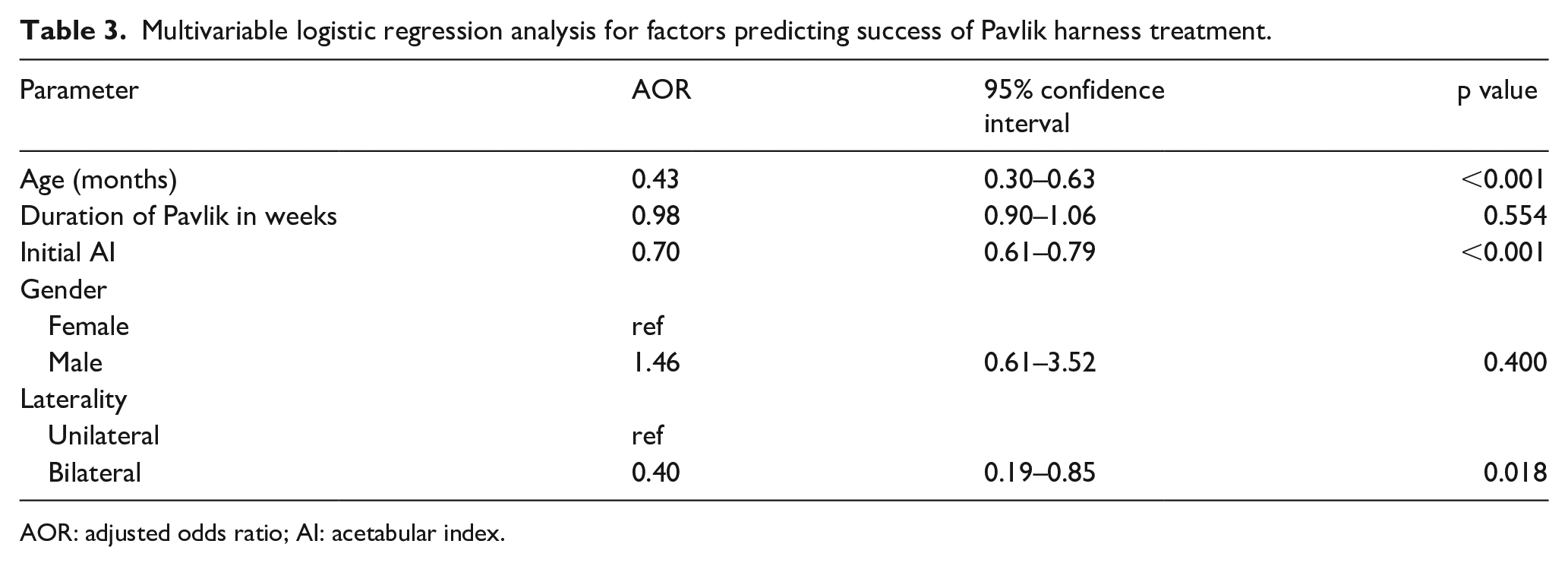
AOR: adjusted odds ratio; AI: acetabular index.
An age of 4.5 months or older was found to be the threshold for having an unsuccessful result following PH treatment, with a sensitivity of 65.2% (95% CI = 56.5%–73.2%) and specificity of 57.3% (95% CI = 46.8%–67.3%) (AUC = 0.652; 95% CI = 0.580–0.724) (Figure 2). An initial AI of 35.5° was found to be the threshold for having an unsuccessful result, with a sensitivity of 83.7% (95% CI = 76.4%–89.5%) and specificity of 61.5% (95% CI = 51.0%–71.2%) (AUC = 0.793; 95% CI = 0.724–0.851) (Figure 2).
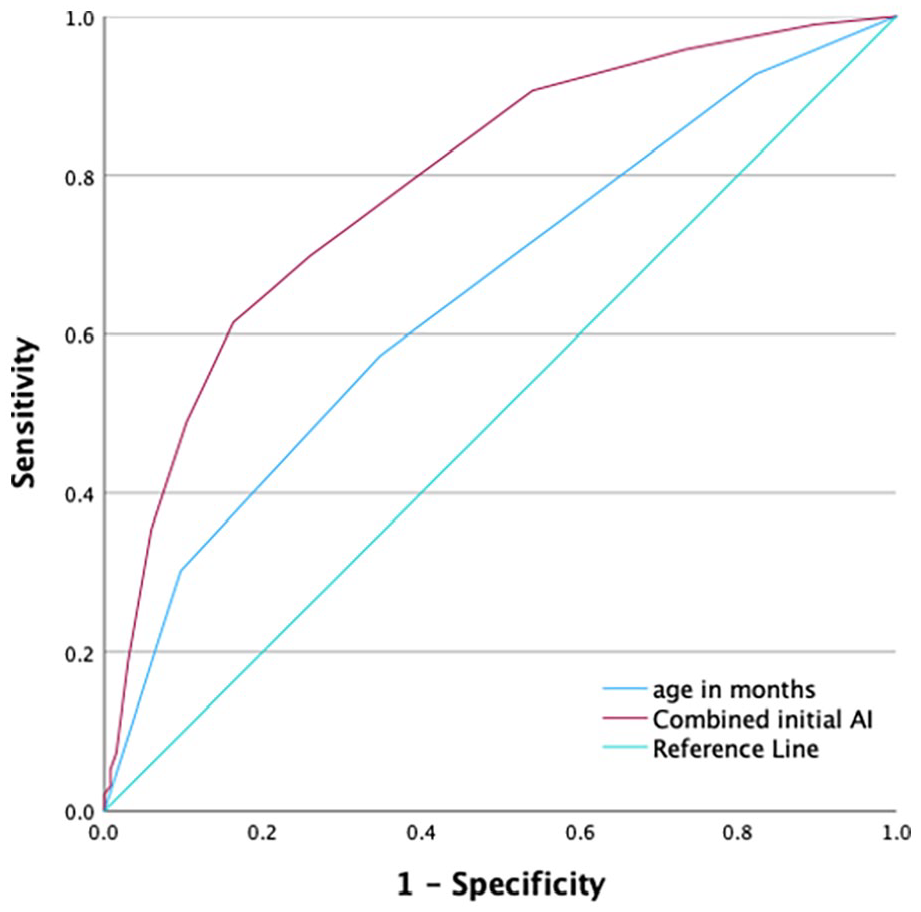
Receiver-operating characteristic (ROC) curve of the age of the infants and the initial acetabular index (AI).
Discussion
Our results demonstrated that initial AI, laterality, and age at presentation were significant predictors of Pavlik’s treatment success in acetabular dysplasia cases. However, gender and duration of PH treatment were not significantly associated with the treatment outcome. In addition, patients presenting at an older age had a worse outcome, and the thresholds for unsuccessful Pavlik treatment were an age of 4.5 months or greater with a sensitivity of 65.2% and a specificity of 57.3% and an AI of 35.5° or higher with a sensitivity of 83.7% and a specificity of 61.5%.
PH application is a popular and widely preferred method for DDH treatment in infants under 6 months of age.27,35 It is generally recognized that various patient-related factors, including the radiological grade of dysplasia, affect the short- and long-term success rates of Pavlik treatment. 36 Yet, there is limited evidence of its effectiveness in terms of AI improvement in clinically stable dysplastic hips, where the outcome is monitored via plain radiographs. This is extremely important, as residual acetabular dysplasia could lead to early degenerative joint disease and chronic disability. 37
Our data showed that PH treatment was effective in 58.4% of infants aged between 3 and 6 months, with several indicators identified for successful treatment. It falls within the reported range of 46%–97% of the PH’s overall success rate.27,29,38 –41 And although several studies revealed a higher success rate for PH than 58.4%, it is important to highlight that our definition of successful treatment was different. Instead of focusing solely on hip stabilization, our success criterion was achieving an AI of less than 30°. In addition, it is worth mentioning that many hips showed improvement, and their AI decreased significantly; however, they did not reach our defined threshold of 30°. Furthermore, it should be noted that the short-term success rates would likely be even higher if infants presenting at younger ages were included in our study. Younger age, male gender, a lower initial AI at presentation, and unilaterality were found to be associated with a better outcome. To add to this, upon regression model, laterality had the highest significant predictive value for successful Pavlik treatment, followed by age and initial AI.
Previous studies have demonstrated that initiating PH treatment before the age of 2–3 months can result in a noticeably increased success rate.39,42,43 In addition, patients presenting at a later age were at a higher risk of requiring surgical interventions. 3 Meanwhile, some other studies found that treatment failure was not related to the age of DDH diagnosis or the age of treatment initiation.44 –46 This could be explained by incomparable age groups across different studies, as the median age at treatment in the Lerman et al. 46 series was 7 days. In 130 ultrasonography-monitored DDH cases, Ömeroğlu et al. 29 found that the threshold for unsuccessful treatment was 4 months or more, with a sensitivity and specificity of 66% and 77%, respectively. Another study by Inoue et al. 43 also found that age at treatment initiation of 4 months or above was a risk factor for unsuccessful treatment. Similar findings were observed in our cohort; the threshold for unsuccessful Pavlik was 4.5 months or older in patients with clinically silent dysplasia, with a sensitivity of 65.2% and a specificity of 57.3%. In contrast, Atalar et al. 39 found that infants aged below 7 weeks had significantly higher chances of successful Pavlik treatment than older infants. These variations could be attributed to differences in outcome measurements and the severity of DDH cases in the included populations.
Several studies assessed the outcome of Pavlik treatment in terms of ultrasonographic features such as the α angle, β angle, and femoral head coverage.29,47,48 It was reported that the failure threshold of Pavlik treatment was an initial α angle of 46° and less, with a sensitivity of 47% and a specificity of 86%. 29 Similarly, Gou et al. 49 developed a predictive model of early Pavlik failure in infants below 6 months. Their nomogram was composed of age, α angle, and the presence of concomitant deformity and had good sensitivity and specificity (70.6% and 88.9%, respectively). In our series, we assessed the outcome using the AI, which showed a threshold of 35.5° or higher for unsuccessful Pavlik treatment in patients with clinically stable dysplasia, with a sensitivity of 83.7% and a specificity of 61.5%. This is consistent with a previous study of 100 hips where an acetabular angle of 36° or higher was a predictive factor of unsuccessful Pavlik treatment. 43 This finding is of significant importance as radiographic surveillance is essential to guiding the timing of surgical and further interventions to address residual dysplasia, which could minimize the need for early hip arthroplasty. 50 In fact, the AI is an essential objective measurement to evaluate hip dysplasia, namely in children from 4 months to 8 years old. 51
The optimal duration of PH treatment remains controversial;47,52 the individualization of the treatment is recommended for each hip without strict time limits. 11 Multiple studies reported the mean duration of PH treatment to be between 8 and 11.7 weeks.39,47,53 Therefore, infants with DDH in our cohort were followed up for a reasonable amount of time, with a mean duration of 9.09 weeks, given that the more severe subluxated or dislocated DDH cases were not part of our cohort. Furthermore, all infants treated at our institution are scheduled for follow-up visits after they begin walking, usually around 12 months of age. During these visits, a standing pelvic X-ray is routinely performed to assess the presence of any secondary dysplasia.
Although DDH is more common in females, 54 previous studies reported that the infant’s gender does not affect the success rate of Pavlik treatment,39,46,49 which is consistent with our regression model. Similar to our results, previous studies39,42 reported an increase in the likelihood of Pavlik treatment failure in patients with bilateral DDH. In contrast, Harding et al. 55 did not find such an increase in failure rates in bilateral cases. A noteworthy aspect of our study was the relatively high rate of bilaterality of 68.4% observed among our cohort. This finding aligns with a previous study from Jordan, where 57% of patients were diagnosed with bilateral DDH 56 and could be explained by environmental variables and other factors. 57
The maturity and growth of the acetabulum in DDH patients may result in the gradual normalization of the AI, improving hip stability and alignment over time. 58 However, for the sake of this study, we had to come up with a definition beyond which treatment is labeled as unsuccessful, although we are optimistic with regard to the natural maturation process and its ability to bring those hips to an acceptable range during follow-up at an older age.
Our study has several limitations that should be considered when interpreting the results. First, its retrospective nature necessitated the interpretation of clinical notes and occasionally encountering issues with incomplete records. Second, there was no control group for comparison, and other measurements to assess the course and outcome of dysplasia were absent. Third, there was no adjustment for some confounding variables, such as poor compliance or interobserver variation in AI measurement. Nonetheless, our study has significant strengths. At first, we used a consecutive series of patients, which we believe is representative of the general population of DDH patients presenting to the pediatric orthopedic clinic. Furthermore, the data collection method was the same for all patients and was concise, easy to understand, and easy to interpret. Finally, we included a sufficient number of patients with close follow-up and gained insight into the duration and AI improvement. Based on the findings of our study, we recommend starting treatment earlier, as we were able to conclude that treatment initiation at 4.5 months and above yielded worse outcomes and required further interventions.
An X-ray was used as a screening tool for the hip for all children in this study, which is not usually recommended before 3–4 months of age. This protocol leads to delayed diagnosis and increased radiation exposure, especially when having to undergo serial X-rays, even though Vogel et al. demonstrated the safety of repeated radiographs in DDH diagnosis and follow-up by calculating the effective radiation dose for infants with DDH that underwent seven serial pelvic X-rays during their treatment course. They reported a lifetime risk of malignancy of 1 in 50,000, which is classified as “very low risk.” 59 In our institute, selective hip ultrasound, in association with clinical examination, is considered a screening protocol for newborns at 6 weeks when risk factors are present. Previous literature has recommended that a neonatologist or pediatrician must examine their hips clinically, and an ultrasound examination should be done for all newborns between 4 and 6 weeks, regardless of the risk factors. 60 We stress the importance of conducting a multidisciplinary prospective study with a control group in the future and the need for a nationwide multicenter study with long-term data to develop a nationally standardized early screening protocol for DDH in our country.
Conclusion
In conclusion, this study provides evidence that the initial AI, laterality, and age at presentation were indicators of Pavlik’s treatment success in cases of clinically silent dysplasia. Patients presenting at an older age had a worse outcome, and the thresholds for unsuccessful Pavlik treatment were an age of 4.5 months or greater and an AI of 35.5° or higher. Clinical assessment with ultrasonography should be considered the primary screening technique for infants with DDH.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231199519 – Supplemental material for Acetabular index as an indicator of Pavlik harness success in grade I developmental dysplasia of the hip: A retrospective study
Supplemental material, sj-pdf-1-cho-10.1177_18632521231199519 for Acetabular index as an indicator of Pavlik harness success in grade I developmental dysplasia of the hip: A retrospective study by Mohamad Samih Yasin, Joud Al Karmi, Dara Osama Suleiman, Yusur Myasar Raja, Mohammad A Alshrouf, Ahmad Abu Halaweh, Mohammad Hamdan and Omar Samarah in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors appreciate the technical support of all the radiology staff.
Author contributions
Conceptualization: MSY, OS, and MH; methodology: DOS, JAK, and MAA; validation: JAK; formal analysis: MAA; investigation: MSY and AAH; resources, DOS and YMR; writing—original draft preparation, MSY, DOS, JA, MAA, YMR, OS, MH, and AAH; writing—review and editing: JAK, MSY, and MAA; visualization: MSY and JAK; supervision: MSY; project administration: MSY. All authors made substantial contributions to the conception and design acquisition of data and drafted the article or revised it critically for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are not publicly available but may be made available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.