
Abstract
Purpose
Achondroplasia is the most common form of skeletal dysplasia, affecting more than 250 000 individuals worldwide. In these patients, the developing knee undergoes multiple anatomical changes. The purpose of this study was to characterise the intra-articular knee anatomy in children with achondroplasia who underwent knee arthroscopy.
Methods
Records of achondroplasia patients who underwent knee arthroscopy between 2009 and 2014 were reviewed. Demographic data, operative reports, follow-up notes, MRI and arthroscopy images were reviewed. Bony, cartilaginous and ligamentous changes were noted. The trochlea sulcus angle was measured from intra-operative arthroscopic images.
Results
A total of 12 knee arthroscopies in nine patients were performed. The mean age at surgery was 16.9 years (12 to 22). In all patients, the indication for surgery was knee pain and/or mechanical symptoms that were refractory to non-operative treatment. Three anatomical variations involving the distal femur were found in all knees: a deep femoral trochlea; a high A-shaped intercondylar notch; and a vertically oriented anterior cruciate ligament. The average trochlea sulcus angle measured 123°. Pathology included: synovial plica (one knee); chondral lesions (three knees); discoid lateral meniscus (11 knees); and meniscal tears (six knees). All patients were pain-free and returned to normal activity at final follow-up.
Conclusion
Children with achondroplasia have characteristic distal femur anatomy noted during knee arthroscopy. These variations should be considered normal during knee arthroscopy in these patients. Arthroscopic findings confirmed previous MRI findings within this specific population with the addition of a deep trochlear groove which was not previously reported.
Introduction
Achondroplasia is the most common form of skeletal dysplasia. 1 Its incidence is 0.5 to 1.5 per 10 000 births, affecting more than 250 000 individuals worldwide. 2 This condition is characterised by disproportionate short stature, lordotic lumbar spine, 2 genu varum, internal tibial torsion and ligamentous laxity. 3 This autosomal dominant disorder is caused, in over 95% of cases, by mutations in the type 3 receptor for fibroblast growth factor (FGFR3), which is necessary for bone elongation as well as craniofacial, vertebral and neurological development. 4
Knee pain is a common reason for orthopaedic consultation in these patients. It is well-known that the knee joint undergoes multiple changes secondary to a combination of bone deformity and dynamic changes. 5 In addition, tibial bowing is often considered a hallmark of achondroplasia 2 and may be associated with genu recurvatum, genu varum, internal tibial torsion or internal derangement of the knee. 3 Moreover, knee pain may be referred from ipsilateral hip or lumbar spine pathology.
Historically, the study of these knee deformities has been limited to plain radiographs. These radiographic findings include an inverted V-shaped distal femoral physis, prominent tibial tubercle, and distal femoral and proximal tibial angulation. 6
Knee MRI findings in children and young adults with achondroplasia 6 have been recently reported. Described deformities included increased knee flexion, patella baja, deep A-shaped intercondylar notch, increased anterior cruciate ligament (ACL)-Blumensaat line angle, a taut posterior cruciate ligament (PCL) and discoid lateral meniscus. To our knowledge, characteristic knee arthroscopy findings in this population have never been reported.
The purpose of this study was to characterise the common, intra-articular knee anatomy in children with achondroplasia. Moreover, we aimed to corroborate our findings with previously published radiographic findings in these patients.
Patients and methods
After obtaining the approval of our Institutional Review Board, a prospectively collected database of all children with achondroplasia who underwent knee arthroscopy at our institution between 1 January 2009 and 31 December 2014 was retrospectively reviewed. Demographic data, operative reports, MRI and radiographic imaging, follow-up notes and arthroscopic images were reviewed. Morphologic changes of the bone, cartilaginous and ligamentous structures were noted. Routine diagnostic arthroscopy (using anterolateral viewing and anteromedial working portals) was performed, making note of any chondral, meniscal or ligamentous pathology.
Arthroscopic images were obtained during surgery and uploaded to the hospital imaging system. These images were then used to measure the trochlea sulcus angles at the level of maximum depth on each patient. Arthroscopic images from similarly aged non-achondroplasia patients were also uploaded, and the trochlea sulcus was measured from maximum depth for comparison.
Results
We performed 12 knee arthroscopies in nine patients with achondroplasia (three bilateral). Five of the patients were males and six arthroscopies were performed on the right knee. Mean age at surgery was 16.9 years (12 to 22). The indications for surgery were knee pain with or without mechanical symptoms that were refractory to non-operative treatment.
Three anatomical variations were found consistently in all knees: a deep femoral trochlea (Fig. 1), a high A-shaped intercondylar notch (Fig. 2) and a vertically oriented ACL (Fig. 3; Table 1). The average trochlea sulcus angles measured at 123° (119° to 132°).
Findings in knee arthroscopies
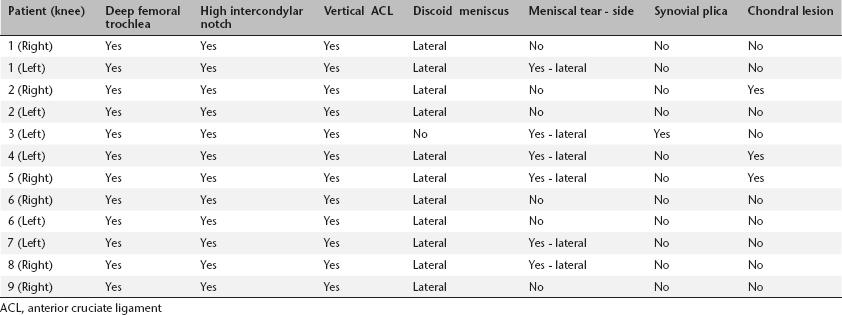
ACL, anterior cruciate ligament
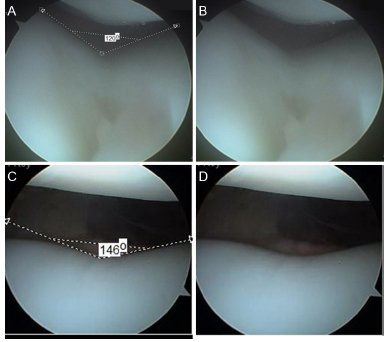
Femoral trochlea.
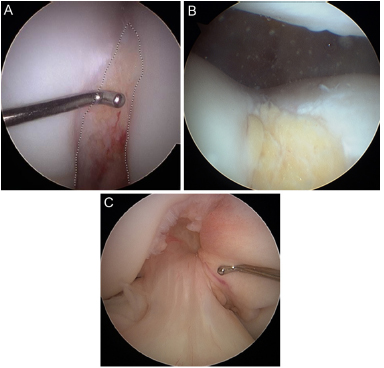
Intercondylar notch.
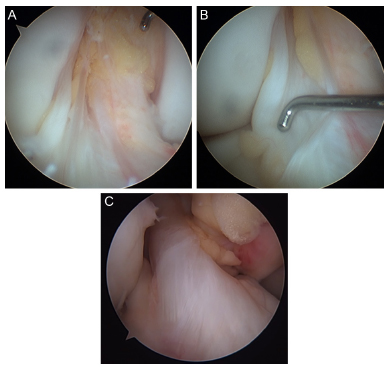
Anterior cruciate ligament, femoral insertion.
Clinical findings
All patients presented with knee pain as their chief complaint. Many patients also presented with mechanical symptoms of clicking or popping with or without locking. On physical exam, patients had joint-line tenderness as well as pain and/or popping with McMurray's testing. Degree of range of motion was not reported for all patients; however, none were reported to have a limitation to motion. Interestingly, all patients had an increased anterior tibial translation and a grade I pivot shift with an intact ACL. Overall alignment of the lower extremities was genu varum consistent with achondroplasia patients. Patients were initially treated with conservative management, consisting of physical therapy, activity modification and anti-inflammatories. Surgery was indicated after adequate conservative measures failed to relieve symptoms.
MRI findings
Axial imaging demonstrated both the A-shaped intercondylar notch as well as the deep femoral trochlea (Fig. 4a and b). Discoid lateral meniscus was seen in 11 of 12 patients (Fig. 4c and d). Sagittal imaging showed an intact anterior cruciate ligament with a more vertical alignment (Fig. 4e).
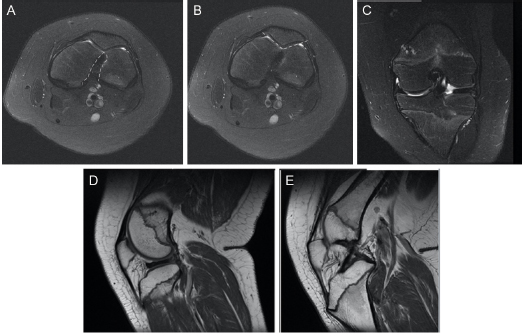
MRI of a 12-year-old female with achondroplasia.
Noted intra-articular pathology
A discoid lateral meniscus was confirmed in 11 of 12 cases (Fig. 5a and b). Meniscal tears were found in 50% of knees (6 of 12) and were all seen in the lateral meniscus. Five of these tears occurred in discoid meniscus and one tear in a normal meniscus. Saucerisation and debridement were performed to treat three tears (Fig. 5c). Meniscal repair was performed (two all inside and one inside-out) to treat the other three tears. A synovial plica band was found in one knee and was excised with the shaver. In three knees, chondral lesions were found: two knees with patellar cartilage fibrillation and one knee with an osteochondral defect in lateral femoral condyle.
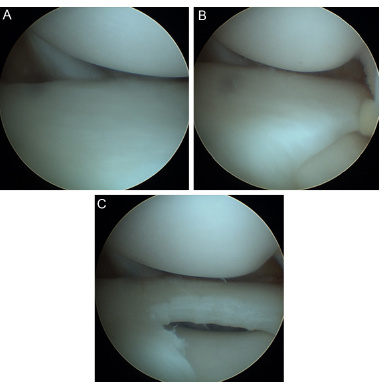
Lateral discoid meniscus.
At final follow-up of at least 18 months (18 months to 6 years), all patients were pain-free and able to return to previous level of activity. There were no minor or major complications noted in this patient cohort.
Discussion
Multiple anatomical abnormalities of the knee have been described in children with achondroplasia. Historically, knowledge about these deformities has been limited to physical examination findings and radiographic imaging. However, since these patients have characteristic anatomy, it may be difficult to differentiate between their ‘normal’ anatomy and intra-articular pathology at the time of arthroscopy. 6
In our study, three anatomical variations were found in the distal femur. First, the femoral trochlea was deep and V-shaped (Fig. 1). This bony structure consists of the lateral and medial facets of the femoral sulcus and aids in patellar tracking. 7 In the normal knee, the sulcus angle usually varies in the range of 138° ± 6°, but it may be higher in cases of trochlear dysplasia where it may be almost flat. 8 In our patients, the sulcus angle was much steeper at an average of 123°. This feature appeared to be consistent in all our patients. Although there were no patients in our cohort with patellofemoral pain or instability, the biomechanical implications of this anatomic variation on the patellofemoral joint are unknown.
Second, the intercondylar notch had consistent morphology. Typically, the intercondylar notch is a deep depression in the distal femoral region between the two femoral condyles. This area has very precise anatomical features which are of particular importance in reconstructive surgery of cruciate ligaments.9–11 In our series, all patients had a very high, A-shaped intercondylar notch, rather than the characteristic inverted U appearance seen in normal knees (Fig. 2).
Third, the ACL was found to be vertically oriented in all patients. The ligament appeared longer due to its orientation (Fig. 3). The femoral insertion of the ligament was observed to be higher (more anterior) than normal without other variations. Surprisingly, the tibial insertion of the ACL was normal in all patients. The ACL appearance, consistency and tension were normal as well. Interestingly, all the patients had increased anterior translation of the tibia in relation to the distal femur on physical examination. Although all patients had at least a grade I pivot shift on examination, no patient had reported subjective complaints of knee instability during athletic activity. It is well documented that a vertically oriented ACL can lead to decreased rotational stability and a subjective feeling of instability.12,13 The ACL appearance, consistency and tension were normal in our patients when probed during arthroscopy. This suggests that the laxity on pivot shift seen pre-operatively was more likely secondary to the vertical orientation of the ACL. One potential explanation for lack of subjective knee instability could be related to the length of their lower extremities in relation to their overall body length. It is possible that with their disproportionate limb-length, their knees are not subjected to the same rotational forces as average stature individuals. As a result, the ACL in these patients may not be as necessary to maintain rotational stability during cutting and pivoting activities. It is also important to note that while the ACL tension appeared normal during intra-operative examination, overall laxity of the soft tissue and hypermobile joints are present in patients with achondroplasia. 14 It is unknown whether this hyper mobility and generalised laxity could lead to over-movement of the joints and eventual wear or stretching of the ACL over time. Further studies would be needed to compare ACL laxity over time in patients with achondroplasia secondary to their joint mobility.
Interestingly, all three variations observed were on the femoral side of the knee. This could be secondary to the fact that the distal femur has the most growth in the lower extremity and achondroplasia directly affects the proliferative zone of the growth plate. Another possible reason is that the distal femoral physis has a natural undulation of the growth plate and, additionally, achondroplasia is known to radiographically have an inverted V-shaped physis, which could explain why these changes were found exclusively in the distal femur.
The presence of discoid lateral meniscus was almost universal in this series (11/12 knees). Although it appears to be highly prevalent, it should be noted that all children included in the study presented with knee pain with or without mechanical symptoms. A case series of six patients with achondroplasia and their clinical outcomes after knee arthroscopy has recently been reported. 15 It should be noted that all of these patients had a discoid lateral meniscus, regardless of other observed pathology. The exact prevalence in asymptomatic patients with achondroplasia is unknown. Although unlikely, it is entirely possible that the findings of discoid menisci in our series were purely coincidental. The number of patients with discoid lateral meniscus in our study could lead to a selection bias; however, all patients that were treated at our institution were reviewed. A future study assessing the prevalence of discoid menisci in patients with achondroplasia would be useful.
The previously reported 6 MRI findings in patients with achondroplasia were confirmed. As seen in that study, the presence of a discoid lateral menisci is consistent (11 of 12 patients). The A-shaped intercondylar notch as well as the vertically oriented ACL was also visualised during arthroscopy.
This study has limitations that should be noted. First, the study design was retrospective in nature and had a small sample size of 12 knees which could have been predisposed to selection bias. Although we observed consistent distal femoral anatomic variations in all patients, more knees would have to be evaluated to say definitively that these changes are present in all achondroplasia patients. Despite this, the fact that the same changes were noted in all patients is highly suggestive that these findings could be consistent in this population. Second, all patients presented with knee pain or mechanical symptoms. There were no asymptomatic patients included in this study. It is possible that the observed anatomic changes are not ‘normal’ for achondroplasia patients, but rather could have predisposed them to the intra-articular derangement they presented with. Future studies evaluating the knee anatomy in a large cohort of asymptomatic achondroplasia patients is warranted.
Children with achondroplasia have characteristic distal femur anatomy noted during knee arthroscopy. This study is the first report to confirm intra-articular knee anatomy in these patients that has been previously described by MRI. In addition, it is the first to identify the deep trochlea sulcus in these patients, which has not, to our knowledge, been previously reported. Surgeons who may perform knee arthroscopies in achondroplasia patients should be aware of the characteristic, intra-articular knee anatomy in these patients. Future, prospective studies are warranted to better characterise the true prevalence of these anatomic findings in these patients.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
No funding was received for this study.
Author William Mackenzie, MD has the following board membership: Non-payment Medical Advisory—Little People of America & MPS Board. Author William Mackenzie, MD has the following consultancy: BioMarin—Paid to Honorarium. Author William Mackenzie, MD has the following expert testimony: BioMarin.
Authors Maria del Pilar Duque Orozco, Nicole C. Record, Kenneth J Rogers, Michael B. Bober and Alfred Atanda Jr. declare that they have no conflicts of interest.