
Abstract
Purpose:
We investigated the medium-term clinical results and revision rate of arthroscopic rim-preserving saucerization for symptomatic lateral discoid meniscus in children.
Methods:
A single-centre, retrospective study was conducted on patients treated with arthroscopy for symptomatic discoid lateral meniscus between December 2005 and May 2019. Eligibility criteria were patients <16 years at the time of surgery and a minimum follow-up of 5 years. Preoperative data (age, sex, symptoms and physical examination), arthroscopic findings (Watanabe and Ahn classifications, meniscal instability and the presence of meniscal tear), treatment (saucerization ± stabilization ± meniscal repair), patient-reported outcome measurements (Lysholm, Tegner and Ikeuchi scores) and arthroscopic revision rate were recorded.
Results:
In all, 47 (72%) of the 65 eligible patients replied to the questionnaires and were therefore included (9 bilateral cases). The mean age at the time of surgery was 8.6 ± 3.3 years. Patient-reported scores were all improved after a mean follow-up of 10.5 years (5–15.9): Ikeuchi (64.2% excellent–good versus 3.6%), Lysholm (90.5 versus 72.9) and Tegner (5 versus 4.3). Two patients developed osteochondritis dissecans of the lateral femoral condyle which healed following non-operative measures. There was no other complication. An arthroscopic revision was performed in 10 patients (17.9%) after a mean follow-up of 2.7 years.
Conclusion:
The medium-term results of rim-preserving arthroscopic saucerization are favourable, yet with a substantial arthroscopic revision rate. Risk factors for failure and revision should be further investigated.
Introduction
Discoid lateral meniscus (DLM) is a congenital malformation. 1 The estimated incidence of symptomatic DLM is 3.2 per 100,000 person-years, although the exact number is unknown because the majority remain asymptomatic.2,3 The DLM is abnormal in its shape, volume and also structure which predisposes it to breakage and cleavage. 4 Recommended treatment includes ‘saucerization’, which consists of trimming out the central meniscal tissue to restore normal shape and volume, and repair when needed.5,6 Repair is indicated in the case of peripheral detachment of the meniscal rim and when central meniscectomy has revealed a meniscal tear in the remaining tissue. Meniscectomy is only appropriate in case a tear is irrepairable. 7 Arthroscopic management allows excellent short-term results according to the literature.6,8 However, some studies reported a decline in clinical scores in the longer term 9 and up to 40% arthroscopic revision for DLM-related symptoms after a minimum of 15 years follow up. 10
The purpose of this study was to evaluate the medium-term clinical outcome of rim-preserving arthroscopic management of symptomatic DLM in children. We hypothesized that DLM-related symptoms would occur after 2 years of follow-up in some patients, requiring arthroscopic revision.
Material and methods
A single-centre, retrospective study was conducted on patients treated with arthroscopy for symptomatic DLM between December 2005 and May 2019. Eligibility criteria were patients <16 years at the time of surgery and a minimum follow-up of 5 years.
In total, 65 patients met the inclusion criteria. Forty-seven patients (72%) responded to the follow-up questionnaire either by email or telephone interview and were therefore included.
The following parameters were recorded:
Age at the time of surgery, sex, side
Preoperative symptoms and physical examination of the knee (comparative range of motion, effusion and the presence of a clunk)
Arthroscopic findings: Watanabe type, Ahn’s classification in case of rim instability, 8 presence of a meniscal tear (type, site and size) and treatment.
Complications, revision arthroscopy and patient-related outcome measurements (PROMs).
DLM was classified according to their shape using Watanabe classification as type I (complete discoid), type II (incomplete) and type III (Wrisberg).
In the case of rim instability, DLM was categorized into three types depending on the tear site: anterior horn type (MC-A type), posterior horn type (MC-P type) and posterolateral corner (PLC) loss type. 8
The procedure started with a meniscus inspection and probing followed by a central meniscectomy using a basket punch and then a shaver. The aim was to obtain normal or near-normal shape and volume. Careful inspection and probing were repeated to check for meniscal tears and to evaluate the stability of the peripheral rim. In case of instability, the rim was sutured to the capsule and/or to the popliteus tendon when needed. Any residual tear was repaired whenever possible or treated with a partial meniscectomy otherwise. In case of a horizontal tear with equal or near equal size femoral and tibial flaps, ‘hay bale’ type vertical sutures were placed. In case 1 side was clearly thinner, it was simply resected using a punch or shaver. Repair consisted of all inside and/or outside techniques depending on the location. All inside repairs included RapidLoc™, Omnispan™ (Mitek) and Fast Fix™ (Smith & Nephew) implants, and outside repairs used 2.0 PDS sutures (Ethicon) and Meniscus mender™ (Smith et Nephew). Five different surgeons from the same Paediatric Orthopaedics Department were involved, all using the same surgical strategy described above.
Postoperative course varied depending on the surgical procedure. In case of an isolated saucerization, full weight bearing was encouraged, and an extension brace was placed for 3 weeks. In the case of meniscal repair, partial weight bearing was allowed with an extension brace for 4–6 weeks. For individuals younger than 10 years with a meniscal repair, an above-the-knee cast was placed, non-weight bearing for 4–6 weeks.
Clinical outcomes and scores were recorded by the patients and his/her family and included the Ikeuchi grading system, 11 Lysholm score 12 and the Tegner activity scale. 13
Statistical analyses were performed using R Studio software (R version 4.2.2).
Categorical variables were described by the number and percentage of each level, and numerical variables by the mean (standard deviation) and median (Q1 and Q3).
The relationship between the dependent categorical variable (e.g. surgical revision or the binarized Ikeuchi score: Bad + medium versus good + excellent) and the independent variables (continuous or categorical) was analysed using logistic regression models. Odds ratios with 95% confidence intervals were calculated to quantify the strength of associations.
To study associations between categorical variables (e.g. Ikeuchi scores and other categorical variables), the chi-square test of independence with continuity correction (Yates correction) was used. For variables with more than two levels, post hoc tests were performed with Holm–Bonferroni correction.
When comparing numerical variables (e.g., Lysholm, Tegner scores) between groups, an analysis of variance (ANOVA) from a linear regression model was used. If an overall difference was detected, post hoc comparisons were performed using Tukey’s procedure. If the model was invalid or if group sizes were very small, a Kruskal–Wallis test was performed, followed by pairwise Wilcoxon rank-sum tests with Holm–Bonferroni correction. For paired analyses, Bowker’s test (nominal symmetry), with continuity correction, was applied to compare the matched proportions of Ikeuchi scores between periods (before versus after), as this is a categorical variable with more than two levels. When Bowker’s test indicated a significant association, McNemar’s test was used for post hoc comparisons with Holm–Bonferroni correction. Similarly, paired numerical variables (e.g. Lysholm, Tegner scores) were compared using paired t-tests if the differences followed a normal distribution; otherwise, the Wilcoxon signed-rank test was applied. Corrections for multiple comparisons, such as Holm–Bonferroni or Tukey’s procedure, were systematically applied where necessary. The significance level was set at p = 0.05.
Results
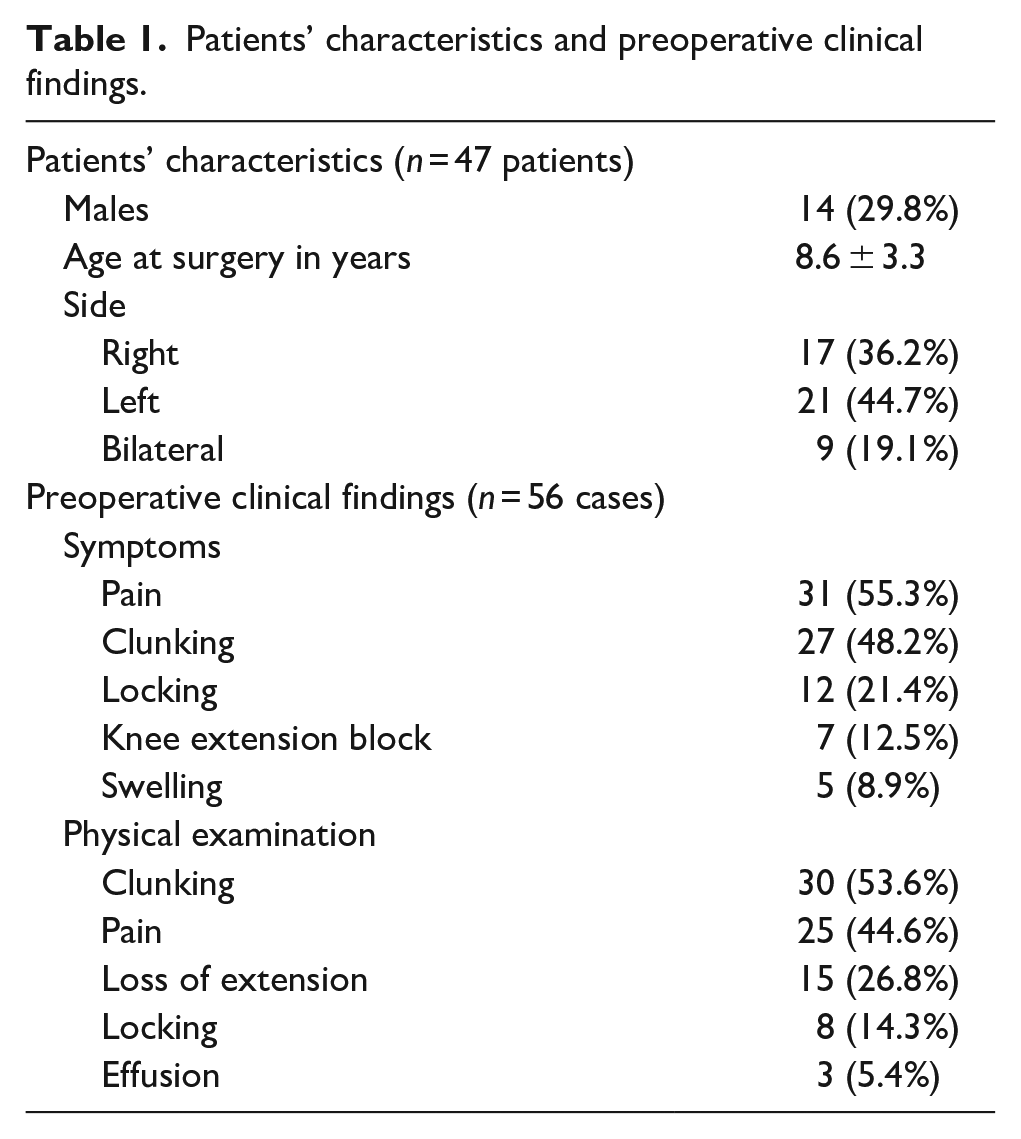
In all cases, the diagnosis of DLM was confirmed preoperatively by an MRI scan. Amongst the 47 patients, 38 were operated on 1 knee and 9 on both knees, always sequentially (19.1%). The mean age at the time of surgery was 8.6 ± 3.3 years (2–15) and the sex ratio was 0.30. The most frequently reported symptom was pain (n = 31), followed by clunking (n = 27). Physical examination revealed clunking when passively mobilizing the knee (n = 30) and tenderness over the lateral knee joint line on palpation (n = 25). Patients’ characteristics and preoperative clinical findings are listed in Table 1.
Patients’ characteristics and preoperative clinical findings.
Arthroscopy confirmed the diagnosis of lateral DLM in all cases with 34 Watanabe type I, 10 type II and 12 type III. There were 12 cases without rim instability, 23 MC-A types, 17 MC-P types and 4 PLC types, according to Ahn’s classification. A meniscal tear was found in 19 cases, most often on the posterior horn (n = 9). Fourteen cases combined rim instability and meniscal tear, 33 cases had rim instability only, 5 cases had meniscal tear only, and 4 cases had neither rim instability nor meniscal tear. A saucerization was performed in all cases, a rim fixation in 48 cases and a meniscal repair in 15 cases (Table 2). Complex tears included two or more tear patterns but were essentially horizontal. They were managed with the principle of saving as much meniscal tissue as possible. Any loose flap was resected and then ‘hay bale’ vertical sutures were applied. The number of sutures used was variable: 1 (n = 24), 2 (n = 14), 3 (n = 8), 4 (n = 4) or 5 (n = 2). There was no case of total/subtotal meniscectomy.
Arthroscopic findings and treatment.
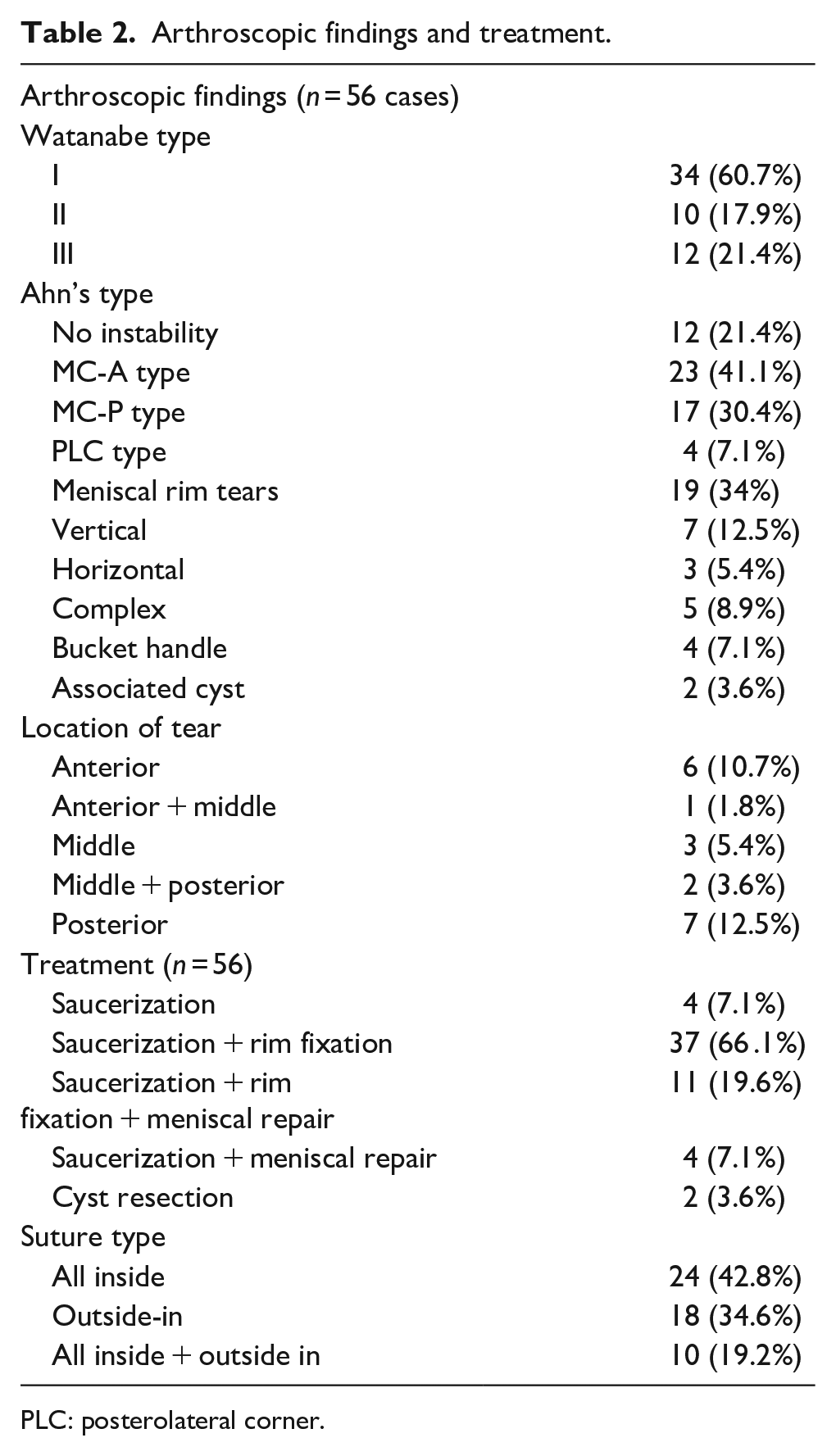
PLC: posterolateral corner.
Osteochondritis dissecans of the lateral condyle was diagnosed in two patients (one bilateral), after 1.8, 4.4 and 5 years postoperatively. The diagnosis was made on knee radiographs and MRI when the patients became symptomatic. All three cases were managed non-operatively with sports restriction with a satisfactory clinical and radiographical outcome within 6–12 months.
No postoperative infection was reported. Ten patients (17.9%) underwent arthroscopic revision after a mean of 2.7 years (0.9–5) post-surgery for recurrence of symptoms. There were eight girls and two boys and their mean age at the time of initial surgery was 8.7 ± 2.9 years. Seven patients presented a horizontal meniscal tear of the posterior horn, two patients had a complex tear of the anterior horn, and one patient had a loose meniscal fragment. Arthroscopic management consisted of meniscal repair and partial meniscectomy in four cases, partial meniscectomy alone in three cases, meniscal repair alone in two cases and removal of the loose body in one case.
Patient-reported scores were all improved after a mean follow-up of 10.5 years (5–15.9): Ikeuchi (64.2% excellent–good versus 3.6%, p < 0.0001), Lysholm (90.5 versus 72.9, p < 0.0001) and Tegner (5 versus 4.3, p = 0.06) (Figure 1).
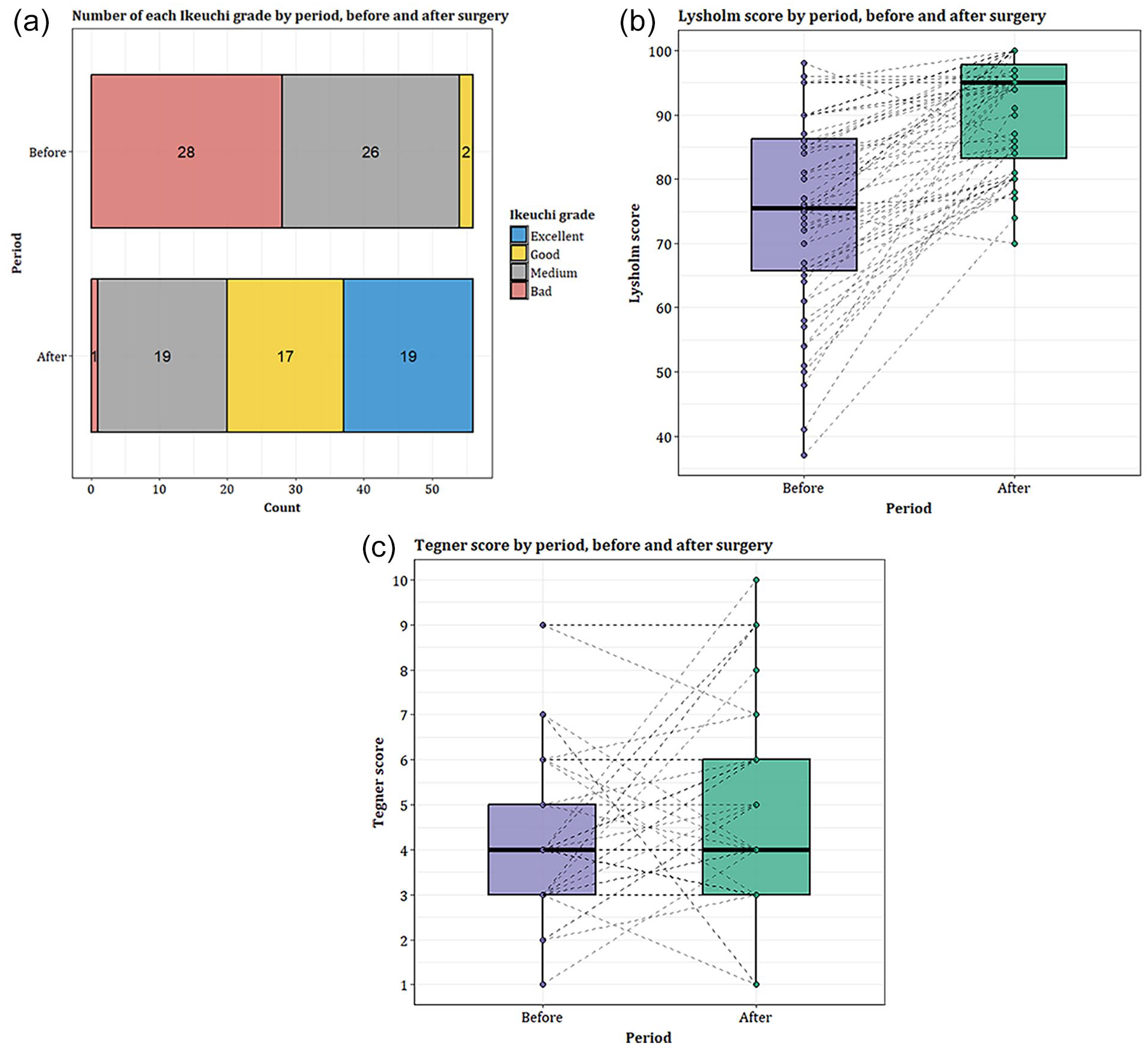
Preoperative and latest follow-up PROMs. (a) Ikeuchi grade, (b) Lysholm score and (c) Tegner activity score.
No factors associated with revision surgery were found. There was no association between Watanabe classification, Ahn’s arthroscopic classification and operative procedure and PROMs. There was no association between the postoperative Ikeuchi score and the presence of preoperative rim instability (p = 0.12) or meniscal tear (p = 0.9).
Discussion
This study showed that patients operated by rim-preserving saucerization have a satisfactory functional result with a substantial medium-term surgical revision rate of 17.9%. Other studies have reported even higher rates. Lee et al. found a 33% revision rate in patients evaluated with a mean of 10 years after the initial intervention. 14 Haskel et al. confirmed the decline of functional outcomes over time. 9 While juxtaposing distinct paediatric study populations has inherent limitations, a higher percentage of patients required additional surgery on the affected knee at 20-year follow-up 10 compared with 11-year follow-up, 9 and 10-year follow-up in the current study (44%, 20.6%–17.9%, respectively). This reported decline of the clinical outcome over time is not insignificant and could be related to early onset degenerative changes. The relatively low mean Tegner score in the current series may also suggest a degree of activity avoidance. According to a study by Yoo et al., age at surgery was negatively associated with the clinical outcome at 4.7 years follow-up evaluation, with patients younger than 10 years at surgery having a 2.37 times higher probability of having excellent Lysholm scores. 15 A study by Ohnishi et al. confirmed that children aged ≤13 years had significantly higher IKDC scores than patients aged ≥13 years at 30 months of mean follow-up. 16
We failed to identify factors associated with revision surgery. None of the factors studied were associated with revision, namely age at surgery, physical examination findings, type of discoid, instability of the remnant rim, meniscal tears, surgical technique and PROMs. These results are consistent with the research from Ng et al. 17 and Bauwens et al. 18 who concluded there was no association between clinical outcome and instability of the DLM. However, it should be noted that all patients who had revision surgery in our study had rim stabilization and/or meniscal repair. DLM treated with any kind of repair may be more prone to failure and thus to revision arthroscopy. Our study may have been underpowered to demonstrate it. Of the 10 patients who required revision arthroscopy, 9 had a meniscal tear, including 5 recurrences. The vulnerability of the DLM to tearing is related to its poor vascularization and decreased number and abnormal arrangement of its collagen fibers. 4 This accounts for a higher failure rate of repair in DLM than in normal menisci with a traumatic injury. Hence, we believe that suture density should be higher in DLM than in normal menisci. All five patients reoperated for failed initial stabilization or repair had a single stitch repair at the initial procedure. In the series from Bauwens et al., a minimum of three sutures were placed with a revision rate of 18% at 41.5 months of median follow-up. 18
A majority of patients in our series were females (70%) which is consistent with a recent national epidemiologic survey from South Korea, reporting on 55% females. 19
This study has some limitations: its retrospective nature which limits the ability to collect data completely and exhaustively; the relatively small number of cases did not allow to highlight risk factors for revision surgery; and finally, during the long period of inclusion (13 years), repair techniques have evolved. Recall bias must be considered, given the retroactive completion of relatively complex questionnaires by adolescents and adults who were children and pre-adolescents at the time of surgery. The lack of systematic imaging in the follow-up did not allow us to investigate meniscal healing and morphology or the presence of early osteoarthritis. Outcome evaluation only relied on the need for surgical revision and questionnaires.
Conclusion
The medium-term results of rim-preserving arthroscopic saucerization are favourable, yet with a substantial arthroscopic revision rate. We currently run a multicentre prospective study to better investigate the predictive factors of the medium- and long-term outcomes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251325030 – Supplemental material for Arthroscopic management of discoid lateral meniscus in children: 5-Year minimum follow-up clinical outcome
Supplemental material, sj-pdf-1-cho-10.1177_18632521251325030 for Arthroscopic management of discoid lateral meniscus in children: 5-Year minimum follow-up clinical outcome by Rebecca Bonny Obro, Joe Rassi, Clara Flumian, Jérôme Sales de Gauzy and Franck Accadbled in Journal of Children’s Orthopaedics
Footnotes
Authors’ contributions
Rebecca Bonny Obro: Data acquisition, Data analysis and interpretation, manuscript writing.
Jo Rassi: Data analysis and interpretation, critical revisions, manuscript review.
Clara Flumian: Statistical analysis.
Sales de Gauzy Jerôme: Critical revisions, manuscript review.
Accadbled Franck: Study design, data interpretation, critical revisions, manuscript review and edition, technical and material support, study supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The study was registered by the Institution Review Board and informed consent was obtained from all participating patients and families
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.