
Abstract
Purpose
The Avon Longitudinal Study of Parents and Children (ALSPAC) prospective cohort was used to determine the accuracy of the Paley multiplier method for predicting leg length. Using menarche as a proxy, physiological age was then used to increase the accuracy of the multiplier.
Methods
Chronological age was corrected in female patients over the age of eight years with documented date of first menses. Final sub-ischial leg length and predicted final leg length were predicted for all data points.
Results
Good correlation was demonstrated between the Paley and ALSPAC data. The average error in prediction depended on the time of assessment, tending to improve as the child got older. It varied from 2.2 cm at the age of seven years to 1.8 cm at the age of 14 years. When chronological age was corrected, the accuracy of multiplier increased. Age correction of 50% improved multiplier predictions by up to 28%.
Conclusion
There appears to have been no significant change in growth trajectories of the two populations who were chronologically separated by 40 years. While the Paley data were based on extracting trends from averaged data, the ALSPAC dataset provides descriptive statistics from which it is possible to compare populations and assess the accuracy of the multiplier method. The data suggest that the accuracy improves as the patient gets close to the average skeletal maturity but that results need to be interpreted in conjunction with a radiological assessment of the growth plates. The magnitude of the errors in prediction suggest that when using the multiplier, the clinician must remain vigilant and prepared to perform a contralateral epiphyseodisis if the prediction proves to be wrong. The data suggest a relationship between the multiplier and menarche. There appears to be a factorisation and when accounting for physiological age, one needs to correct by 50% of the difference between chronological and physiological age.
Introduction
Children have an ability to compensate for minor limb-length discrepancies; however, discrepancies of greater than 2 cm are thought to cause functional problems in many patients and discrepancies of less than this may cause long-term problems of the back, hip and knee.1,2
The general aim of management is to produce functionally equal leg-lengths at the time of skeletal maturity for which the most efficient surgical method is to arrest longitudinal growth in the peri-pubertal phase with an epiphysiodesis. From a technical perspective, this is a relatively straightforward procedure, but the main difficulty is the determination of the correct time for intervention.
Historic datasets have been used to estimate remaining growth in children. These calculations are usually based on data collected by Anderson and Green in a semi-longitudinal cohort study of 255 children, whose ages ranged from five to 18 years. 3 Of those children under surveillance, 84% had contralateral poliomyelitis with measurements taken from the unaffected ‘normal’ limbs. 3 This is a potentially significant confounding factor and with the additional effect of improvements in nutrition in the developed world over the last 50 years, there are concerns that these historic datasets are no longer relevant.
A number of techniques to estimate the leg-length difference at skeletal maturity have been described since the 1940s, each making different assumptions about the available data. Little et al, however, concluded that there was a ‘significant rate of poor outcomes’, irrespective of method used, when comparing Anderson and Green, and Menelaus and Mosley.4–7 All methods had a proportion of patients who had an error of up to 2 cm in the prediction of final leg-length.
Moseley introduced a graphic method of assessment which made important assumptions about the age of skeletal maturity.7,8 Based on a retrospective cohort of 30 children, Moseley's graph proved to be as accurate as that of Anderson et al in predicting remaining growth and more accurate in cases of high growth inhibition.3,5,7
Anderson's Growth Remaining Method and Moseley's Straight Line Graph both rely on annual radiographs involving individual bone, overall limb length or skeletal age measurements.5,7
Menelaus published a non-graphical arithmetic method, which was clinically based with no routine exposure to radiation. 6 The fundamental assumption with this system was that boys reached skeletal maturity at 16 years and girls at 14 years. The paper recognised that a previous publication estimated female skeletal maturity was reached at 15 years. 9
Menelaus highlighted the unpredictability of leg-length discrepancy due to variable pathology. It therefore cannot be assumed that the growth inhibition of the short leg or the annual increase in discrepancy of the leg-lengths is constant. 6
Recent improvements in methods of calculation have been based on more sophisticated mathematical algorithms, but the quality of the original data remains the rate limiting step. The multiplier method described by Aguilar and Paley is regarded as the most sophisticated and accurate method of assessment. 10 In their validation of the method, they assessed the mean error of the assessment of the lengths of the individual bones (tibia and femur) as being 1.1 cm.
The aims of this study are to assess the accuracy of the predictions of final leg-lengths using the multiplier method, both on a population and an individual level, and to identify if accuracy can be improved using a corrective factor for physiological age.
A prospective, longitudinal dataset of a large British population was used to assess both the accuracy of the multiplier and whether the multiplier method is independent of physiological age. We concentrated on female participants and used menarche as a proxy to investigate the effect of physiological age on the accuracy of prediction of leg length.
Ethical approval for the study was obtained from the Avon Longitudinal Study of Parents and Children of the 1990s (ALSPAC) Ethics and Law Committee.
Patients and Methods
The ALSPAC is a population-based cohort study of contemporary British families. 11 It is a birth cohort; women were recruited during pregnancy and an additional 713 children were recruited at the age of seven years. Mothers with expected dates between 31 December 1992 and 1 April 1999 were enrolled and the children had their development observed through to puberty. The phases of enrolment are described in more detail in the cohort profile paper. 12
Age and gender were recorded as dependent variables with leg-length as the independent variable. Standing and sitting height were assessed six times during childhood. Average age at each reading was 7.5, 9.5, 10.6, 11.5, 12.6 and 15.6 years, respectively. Staff were trained and assessed in the use of all equipment. Height was measured using the Harpenden Stadiometer and sitting height was measured using the Harpenden sitting height table anthropometer, both measured to the last complete millimetre. Subischial leg-length was taken as standing height minus sitting height.
Children were asked to give the date of their first period in a yearly questionnaire administered between the age of eight and 17 years. If patients responded in more than one questionnaire with different dates, an average was taken. The study website contains details of all the data that are available through a fully searchable data dictionary. 13
Radiographic assessments were not available as this was a population-based study with no indication to obtain radiographs.
Leg-Length Multiplier (LLM) was calculated for every recorded leg-length, in whom a final leg-length had been recorded over the age of 15 years, and plotted against the child's corresponding age using the method validated by Aguilar and Paley.
10

Lm = predicted leg-length at skeletal maturity
L = leg-length at their current age
Thus, when the child reaches skeletal maturity, LLM = 1 14
An identical calculation was performed using total height data.
Physiological age based on the date of menarche was substituted for chronological age to investigate the effect on accuracy of the leg-length and total height multiplier.
Physiological age = chronological age – (age at menarche - average age at menarche for ALSPAC cohort).
Chronological age was corrected for female patients over the age of eight years who had documented final height, final subischial leg-length and age at menarche.
The accuracy of the estimation of final leg-length discrepancy and final height was calculated from raw data.
Results
The ALSPAC study involved 15 247 pregnancies and 15 458 births, which were given a unique identification code on enrolment. (Data collection reduced after the age of 16 years and therefore data for boys who only reach skeletal maturity on average around the age of 16 years were not included in this study.) Of these, there were 7151 girls who were recorded as being alive at one year. The data were cleaned as shown in Figure 1.
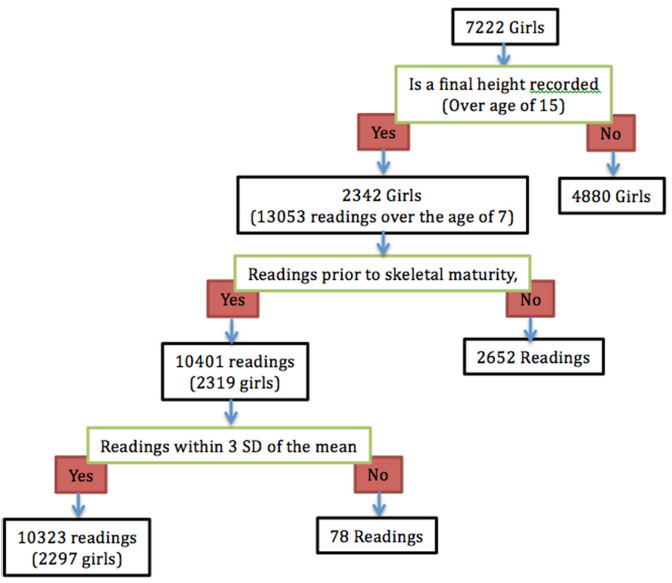
Details of the patient population and leg-length data analysis.
Final leg-lengths (after skeletal maturity) were available for 32% of females, with an average of 4.5 readings between the age of seven years and skeletal maturity.
LLMs were calculated for 10 323 readings with multipliers of greater than 1 (pre-skeletal maturity). The readings were then compared with the historical dataset, described by Paley, and are shown in Figure 2. 14
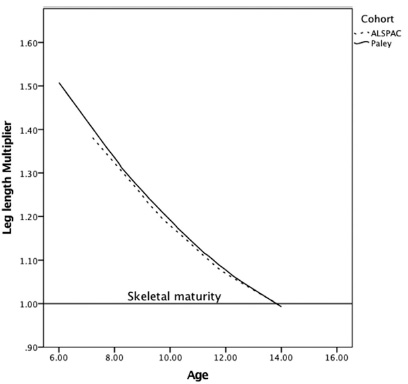
Comparison of multipliers derived from Aguilar and Paley 8 and the ALSPAC cohort. Line of best ft provided by the Loess method.
The distribution of the data points in the ALSPAC cohort is shown in Figure 3.
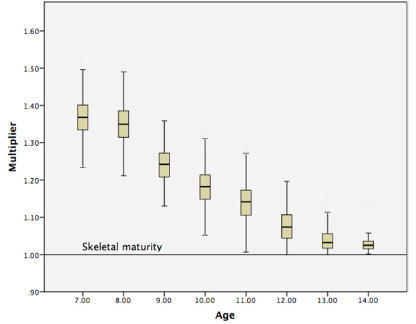
Box and whisker plot demonstrating leg-lenth multiplier (LLM) values in respect of age.
Figure 4 shows three groups of patients: those who went through menarche very early, at least two years earlier than the mean (on average 2.3 years earlier); those who were late, at least two years later than the mean (on average 2.3 years later); and those who went through at the mean age.
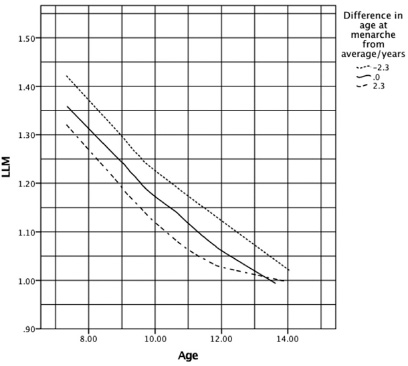
Graph showing the effect of differing ages of menarche on the leg-leng multiplier (LLM) (using a selection of cases split into three groups). Those who underwent menarche at the average time, those who underwent it at least two years early, and those who underwent it at least two years late.
Table 1 shows the effect of correcting for physiological age on the accuracy of multiplier for different age ranges.
Comparison of mean squared error (MSE) and its standard deviation (SD) in leg-length prediction using chronological and physiological age in females. Numbers that are highlighted show where accuracy has been improved by correction.
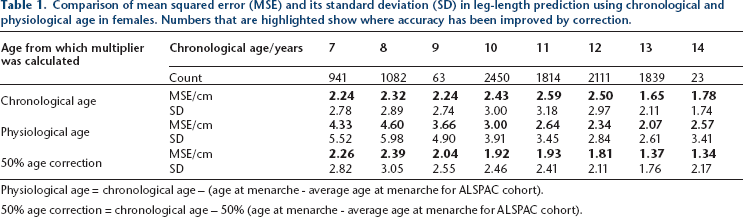
Physiological age = chronological age – (age at menarche - average age at menarche for ALSPAC cohort).
50% age correction = chronological age – 50% (age at menarche - average age at menarche for ALSPAC cohort).
Discussion
The initial component of this study was to assess the accuracy of the Paley multiplier with a contemporary population.
There is a strong association between the Paley multiplier using the Green and Anderson data3,14,15 when compared with data from the ALSPAC study as shown in Figure 2. Statistical comparison was not possible as the dataset from which the Aguilar and Paley multiplier was derived is no longer available. 10
There are, however, very clear similarities in appearance of the plots from each dataset and we are therefore confident that the Paley multiplier method for girls is robust. 10 This would suggest that the growth trajectory for girls has not changed over the time period between these two datasets (1940 to 1980).
The second component was to assess the accuracy of the multiplier at predicting the final leg-length of individuals in the ALSPAC cohort. Despite the similarity between the contemporary and historical datasets seen in Figure 2, it is important to note the wide range of individual data points, as shown in Figure 3.
The average error in prediction depended on the time of assessment and varied from 2.2 cm at age seven years to 1.8 cm at age 14 years, as seen in Table 1. These data are compatible with Aguilar's assessment of the accuracy of this technique, 1.1 cm error in each of the tibia and femur. 10
These data suggest that predictions only improve marginally as the patient nears skeletal maturity, as the multiplier may inaccurately predict the termination of growth. Radiographic assessment of the growth plate may allow a more accurate assessment of remaining growth in these patients.
In the clinical assessment of leg-length discrepancy, the actual error is likely to be a fraction of this, depending on the cause of the leg-length discrepancy. This study was only able to assess how accurate the multiplier is at assessing leg length at maturity not leg-length discrepancy at maturity. Nevertheless, the size of the mean error, 2.6 cm, at the time when one would be frequently performing epiphysiodesis at age 11 years, remains a concern.
The third component of this study was to see if the accuracy of the multiplier could be improved using a physiological age correction using menarche as a proxy. Figure 4 highlights the effect that menarche has on the LLM. The early menarche group appears to grow in a trajectory one year earlier than average, and the late menarche group one year later than average. This is despite their physiological age being two years different from the mean in both cases.
We therefore assessed the accuracy of the multiplier with a full correction for physiological age and with a 50% correction of physiological age. For example, a girl who underwent menarche two years earlier than average and is now aged 13 years, would have a physiological age of 15 years and 50% corrected physiological age of 14 years.
Table 1 shows how correcting for physiological age affects mean accuracy and standard deviation of the error at different ages. We have been able to demonstrate an improvement in the accuracy and the consistency of final leg-length discrepancy assessment using the multiplier method based on a partial correction of physiological age.
Using a 50% correction for age improved the accuracy and consistency of the final calculation up to 28% and improvement was greatest in the peri-pubertal age range (11 to 12) when epiphysiodesis is most commonly performed. A 100% correction did not lead to any improvement in the accuracy or consistency of the multiplier.
We believe that this observation may be related to the hormonal influence on rate of growth and termination of growth, rather than absolute growth.
There appears to have been no significant change in growth trajectories of the two populations who were chronologically separated by 40 years.
While the Paley data were based on extracting trends from averaged data, the ALSPAC dataset provides descriptive statistics from which it is possible to compare populations and assess the accuracy of multiplier method. 14
The data suggest the accuracy improves as the patient gets close to the average skeletal maturity, but that results need to be interpreted in conjunction with a radiological assessment of the growth plates.
The magnitude of the errors in prediction suggests that when using the multiplier, the clinician must remain vigilant and prepared to perform a contralateral epiphyseodisis if the prediction proves to be wrong.
The data suggest a relationship between the multiplier and menarche. There appears to be a factorisation, and when accounting for physiological age, one needs to correct by 50% of the difference between chronological and physiological age.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants/parents included in the study.
Acknowledgement
We are extremely grateful to all the families who took part in this study, the mid-wives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. The UK Medical Research Council and the Welcome Trust (Grant ref: 102215/2/13/2) and the University of Bristol provide core support for ALSPAC.