
Abstract
Objective:
Obesity-associated diabetes causes aging-like changes to skin physiology in animal models, but there have been no clinical studies focusing on human obese diabetic patients. The purpose of this study was to examine the hypothesis that obesity-associated diabetes accelerates aging-like skin changes in Japanese people.
Methods:
This cross-sectional study enrolled obese-diabetes patients (body mass index ≥ 25 kg m−2) and healthy volunteers (body mass index < 25 kg m−2) as controls. Skin physiology parameters relating to aging (stratum corneum hydration, transepidermal water loss, skin pH, advanced glycation end-products, and dermal collagen density) were evaluated in the two groups.
Results:
About 37 subjects participated (16 in a control group and 21 in an obese-diabetes group). Age was not significantly different between the groups. The stratum corneum hydration level was significantly lower in the obese-diabetes group. Transepidermal water loss and levels of advanced glycation end-products were significantly higher in this group. Skin pH was not significantly different between groups. Dermal collagen density decreased in the obese-diabetes group.
Conclusion:
We showed that obese-diabetes patients have decreased stratum corneum hydration, increased transepidermal water loss, higher skin advanced glycation end-products and decreased dermal collagen fiber density compared with normal-weight subjects. These results indicate that the ordinary age-related physiological skin changes seen in the elderly can also occur in obese-diabetes patients aged in their 40s.
Introduction
The prevalence of obesity has increased globally. Obesity plays a major role in the pathogenesis of several metabolic diseases, with type 2 diabetes being the most common complication. 1 Furthermore, obese individuals are 20–38 times more likely to develop type 2 diabetes than non-obese individuals. 2 Therefore, it is reasonable to consider that the increased prevalence of obesity would be associated with an increase in obese patients with diabetes.
Obesity and diabetes are both conditions associated not only with visceral diseases but also with changes in skin physiology.3–7 Previous studies reported that obese diabetic mice show a reduction of stratum corneum water content and lipid content in the skin and a decrease in dermal thickness and dermal collagen and elastic contents.8–12 These skin changes appear similar to those seen in aging. Aging-like skin changes commonly result from (1) dry skin due to decreased stratum corneum water content and increased transepidermal water loss (TEWL),13,14 (2) changes in skin pH due to a decrease in sebum secretion, 15 (3) a thinner dermal layer and decreased collagen content,16–19 and (4) increased advanced glycation end-products (AGEs) in skin. 20 However, previous studies have evaluated only some of these parameters in obesity-associated diabetes. In addition, these studies investigated animal models, and there has been no reported clinical study investigating human obese diabetic patients.
Although the World Health Organization defines obesity as a body mass index (BMI) ≥ 30 kg m−2, “obesity in the Japanese” is defined as a BMI ≥ 25 kg m−2 because Japanese people are at high risk of hypertension and diabetes at comparatively low BMI. Most cases of obesity seen in Japan correspond to overweight people with 25 ≤ BMI < 30 kg m−2. 21 Furthermore, previous studies of obese Japanese people with BMI in this range have reported changes in skin physiology. 22 In this study, we focused on obese Japanese patients with diabetes and examined the hypothesis that this condition causes aging-like skin changes.
Materials and methods
Study design and setting
This was a cross-sectional study conducted between February and July 2015. Data collection and all analyses were performed at the diabetic metabolic outpatient department and campus of the Yokohama City University Hospital.
Subjects
The subjects included obese patients (BMI ≥ 25 kg m−2) with diabetes who visited the diabetes metabolism internal medicine outpatient department. Healthy volunteers (BMI < 25 kg m−2) who were staff members of the university or employees of a nonfinancial company were also included as the control group. The age range of subjects was 20–64 years, and those with systemic skin disease such as atopy or psoriasis and those with smoking habits were excluded. The sample size of this study was set to about 20 subjects in each group, referring to the previous study evaluating the skin physiology of obese people. 23
Characteristics of the study population
Information regarding age, sex, height, anamnesis, intake of diabetic medications, and other oral medications and smoking habits was collected from subjects’ medical records or by oral consultation. Body weight, body fat ratio (%), and BMI were measured using a multi-frequency body composition monitor (Tanita, Tokyo, Japan). Waist circumference was determined using a measuring tape.
Measurement of skin physiological parameters
After resting for 5–10 min at room temperature, between 24°C and 26°C, with ambient humidity between 34% and 60%, the subjects were investigated in a face-up position. The right forearm at the mid-point between the cubital fossa and the radius was examined for aging-like skin changes using the parameters of stratum corneum hydration (Mobile Moisture HP10 N®, Courage + Khazaka, Cologne, Germany), TEWL (Tewameter® TM300, Courage + Khazaka), pH (Skin pH Meter HI99181 N®, HNNA Instruments, Chiba, Japan), AGEs (TruAge scanner®, Diagnoptics Technologies, Groningen, The Netherlands), and dermal collagen density (Derma Lab®, Cologne, Germany). Dermal collagen density was evaluated using high-resolution ultrasonography (Derma Lab®). The resolution was 60×130 µm, and ultrasound penetration was to a depth of 10 mm, according to the manufacturer’s information. Scanning conditions were fixed at −1. Collagen fibers were detected as hyperechoic signals, the intensity of which represents collagen density.24,25 Each parameter was measured three times in every individual and the mean value was calculated.
Analysis
Descriptive data are expressed as the mean ± standard deviation (SD) for continuous variables and n (%) for categorical variables. The subjects were classified into two groups, obese-diabetes (BMI ≥ 25 kg m−2) and controls (BMI < 25 kg m−2). These two groups were compared using independent t-tests, Mann–Whitney U tests, and Fisher’s exact tests. In the comparison of the physiological function of the skin between the two groups, stratum corneum hydration, and TEWL were assessed using Student’s t-test, and pH and AGEs were assessed using the Mann–Whitney U test. IBM SPSS Statistics 22.0 software (IBM, Armonk, NY, USA) was used. Values of p < 0.05 were considered statistically significant.
Ethical considerations
The study was approved by the Ethics Committee of the Yokohama City University School of Medicine (B150108030). Written informed consent was obtained from all participants. The objectives and methods of the study were explained to subjects using documentation. We also explained that no disadvantage would be incurred by refusing to participate and that genomic information would not be disclosed. Data obtained from subjects were anonymized and could not be used to identify individuals. The data were kept strictly in a place that could be locked.
Results
Characteristics of the study population
A total of 37 subjects was recruited (Table 1), with 16 controls (mean age, 46.31 ± 10.3 years) and 21 obese-diabetes subjects (mean age, 49.00 ± 9.5 years). There was no significant difference between their ages. The mean BMI of the control subjects was 20.90 ± 2.0 kg m−2 and that of the obese-diabetes subjects was 35.24 ± 8.9 kg m−2, which was significantly higher than the control group. The proportions of subjects who had hypertension (p = 0.01) and hyperlipidemia (p < 0.01) in the obese-diabetes group were significantly higher than in the control group. The types of diabetic medications in the obese-diabetes group included biguanide in 17 (80.9%) subjects, thiazolidine in 4 (19.0%), dipeptidyl peptidase-4 (DPP-4) inhibitors in 7 (33.3%), and a sodium-glucose co-transporter 2 inhibitor in 1 (0.05%).
Characteristics of subjects.

BMI: body mass index; HbA1c: hemoglobin A1C; DPP-4: dipeptidyl peptidase-4; SGLT: sodium-dependent glucose transporter.
Values are shown as mean (SD).
Student’s t-test.
Values are shown as n (%).
Chi-square test.
Mann–Whitney U test.
Fasting blood glucose level ≥ 110 mg dL−1 and drug therapy.
Systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure 90 mm Hg and/or drug therapy.
Fisher’s exact test.
Serum triglyceride ≥ 150 mg dL−1 and/or high-density lipoprotein cholesterol < 40 mg dL−1.
Skin physiology parameters
Table 2 shows the skin physiology parameters measured for the two groups. We first measured stratum corneum hydration and TEWL as indicators of dry skin. The stratum corneum hydration levels were significantly lower in the obese-diabetes group than in the control group (p = 0.014). The TEWL levels were significantly higher in obese-diabetes than in the controls (p = 0.020). The AGEs levels were also significantly higher in obese-diabetes than in the controls (p = 0.019). Skin pH levels had a non-significant tendency to be increased in the obese-diabetes group compared with the control group (p = 0.075).
Skin physiology parameters.
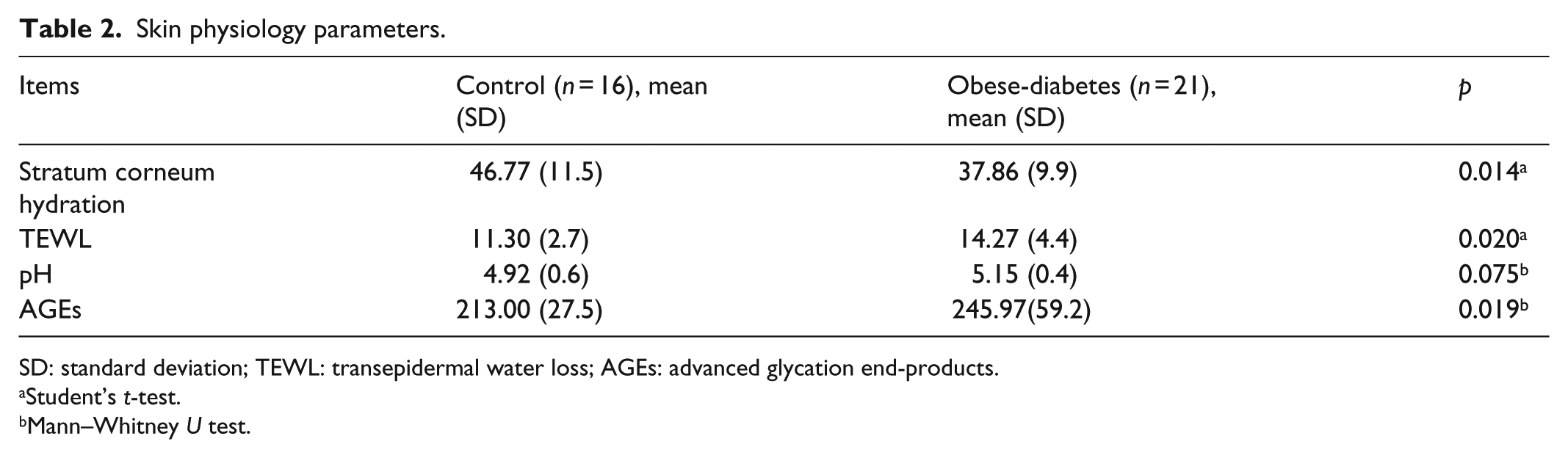
SD: standard deviation; TEWL: transepidermal water loss; AGEs: advanced glycation end-products.
Student’s t-test.
Mann–Whitney U test.
Figure 1 shows an ultrasonographic image of dermal collagen density. Collagen fibers were detected as hyperechoic signals, the intensity of which represents collagen density. Figure 2 shows representative ultrasonographic images for the control and obese-diabetes groups. The echogenicity of the dermis was lower in the obese-diabetes group than in the control group.

Ultrasonographic image showing typical structure of forearm skin. Collagen fibers in the dermis were detected as hyperechoic signals. Their intensity represents collagen density.

Representative ultrasonographic images of the control and obese-diabetes groups. The hyperechoic signals of the dermis were lower in the obese-diabetes group than in the control group.
Discussion
This is the first study to examine aging-like skin physiological changes in Japanese obese-diabetes patients. Keratinocytes and intercellular lipids such as ceramide and cholesterol play an important role in normal skin barrier function, maintaining epidermal hydration. 26 Previous studies reported that aging leads to decreased stratum corneum hydration and increased TEWL, leading in turn to dry skin.13,14 Dry skin is a skin barrier defect and is mainly attributed to a reduction in intercellular lipid and the consequent loss of water from the stratum corneum. TEWL is the most direct indicator of skin barrier function. Our results showed that stratum corneum hydration was significantly decreased and TEWL was increased in obese-diabetes patients compared with the control group. These results suggest that obese-diabetes patients have a disrupted skin barrier function that leads to dry skin. In contrast, Sakai et al. 27 reported that decreased stratum corneum hydration was seen in diabetes mellitus patients but TEWL did not change, suggesting that hyperglycemia reduces skin hydration, but does not impair skin barrier function. However, Loffler et al. 23 reported that obese subjects showed significantly increased TEWL compared with control subjects. Together, these results suggest that the reduction of skin barrier function may be caused not only by diabetes alone but also by combined obesity and diabetes. Yamane et al. 28 reported that increasing body fat in rats fed a high-fat diet is associated with a decrease in adiponectin production by adipocytes and of ceramide in corneocytes. In our study, the obese-diabetes group had significantly more body fat than the controls, which might indicate that excessive fat accumulation resulted in lower levels of adiponectin secretion and ceramide production. It will be necessary to clarify the detailed mechanism by which obesity-associated diabetes causes dry skin in future studies.
Skin pH is mildly acidic, depending on the amount and composition of sebum. 29 The acidity is responsible for the bacteriostatic action of skin. Previous studies reported that aging reduces sebum content and increases skin pH. 15 In our study, although there was no significant difference in the skin pH between the obese and control group, it had a tendency to be increased in the former. A previous study reported that hyperinsulinemia caused modification of sebaceous glands and sweat glands, 30 and these factors may have changed skin pH. However, the precise mechanism remains unknown. Further studies are needed to analyze the sebaceous and sweat glands of obese-diabetes patients.
Skin AGEs are non-enzymatic glycation products of collagen, and indicate the relationship between collagen glycation and changes in connective tissue associated with aging, diabetes and smoking.31–33 Accumulation of AGEs is regarded as an indicator of skin aging as it leads to skin hardening and wrinkle formation.34,35 In our study, the levels of AGEs in the obese-diabetes subjects were significantly higher than in the control group. A previous study reported that there was no difference between skin the AGE of patients with and without central obesity. 36 However, patients with metabolic syndrome, which is a condition involving simultaneous central obesity, diabetes and hypertension, did have higher skin AGEs than participants without metabolic syndrome. 36 This result was consistent with the results of our study. Together, these results suggest that obesity combined with metabolic diseases such as diabetes has a greater effect on the increase in skin AGEs than obesity alone. However, since our study did not evaluate obesity-only subjects, further analysis of such subjects is necessary.
Ultrasound imaging is an effective method for assessing higher density areas of dermal collagen fibers.24,25,37 Collagen fibers comprise approximately 70% of the dermal layer, which is the thickest part of the skin and provides its mechanical strength. 38 Previous studies reported that aging leads to a decrease in collagen fibers,16–18,39 resulting in decreased skin resistance to external force and increased susceptibility to skin disorders. We observed lower ultrasound signal intensities in the obese-diabetes group than in the control group, indicating decreased collagen density. This result is similar to the findings in a previous study for a group of patients in their 70s. 25 In another previous study using obese mice, an increase of the subcutaneous adipose layer decreased the number of dermal fibroblasts and decreased dermal layer thickness and elasticity. 40 Furthermore, there is a negative correlation between increased subcutaneous fat and skin elasticity in humans, and deterioration of skin elasticity reportedly worsens cheek sagging, which is an index of aging. 41 Although the mechanism of this phenomenon is not clear, it has been shown that increasing oxidative stress and the expression of collagen-degradation enzymes in the subcutaneous adipose tissue of obese diabetic mice is related to decreased dermal collagen density.8–10 These results suggest that the accumulation of subcutaneous adipose tissue may affect dermal fragility via a paracrine pathway. Further investigation is required to elucidate these mechanisms in humans.
There were some limitations to this study. First, the obese-diabetes group had significantly more people with hypertension and hyperlipidemia. Hypertension, especially, has been reported to lower blood flow in the skin. 42 It has been reported that decreases in skin blood flow reduce the recovery of skin barrier function. 43 Therefore, it will be necessary to analyze individuals matched for factors such as hypertension in the future. Second, we compared only the control group and an obese-diabetes group. Therefore, it was not clear which of obesity and diabetes more strongly influenced the changes in skin physiology. A future study should analyze four groups, including obesity alone and diabetes alone in addition to the control and obese-diabetes groups analyzed in this study. Third, the subjects of this study included those using DPP-4 inhibitors, which are anti-diabetic agents. It was reported that skin disorders such as bullous pemphigoid, desquamation, and epidermolysis may occur in diabetic patients taking DPP-4 inhibitors. DPP-4, which is identical to leukocyte differentiation antigen CD26, is ubiquitously expressed in various tissues, including skin keratinocytes, and is responsible for regulation of immune function. Therefore, changes in the immune function of the skin are thought to be involved in the onset of skin disorders by administration of DPP-4 inhibitors; however, the detailed mechanisms remain unclear. In this study, we confirmed that no subjects had skin disorders at the time of the survey, and we believe that it is unlikely that internal oral administration of DPP-4 inhibitors affected the results of this survey. However, considering the possible effects that anti-diabetic drugs may have on skin physiology, we believe that careful selection of subjects is necessary in the future.
In conclusion, we showed that obese-diabetes patients had decreased stratum corneum hydration, increased TEWL, higher AGEs, and decreased dermal collagen fiber density compared with normal-weight subjects. These results indicate that changes in skin physiology, which are similar to aging-like skin changes, occur in Japanese obese diabetic patients. The results suggest that the ordinary, age-related skin changes seen in elderly subjects can also occur in obese diabetic patients in their 40s.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.