
Abstract
Summary
Objectives
We set out to evaluate the impact of Foundation Year (FY) training on the doctors who had been through this training system.
Design
Doctors in training were surveyed using a structured web-based questionnaire.
Setting
Postgraduate training in the UK has been the subject of much upheaval in recent years.
Participants
A total of 1065 doctors in training were surveyed in late 2011 and early 2012, of which 638 were current FY doctors.
Main outcome measures
The survey was both quantitative and qualitative, focusing on selection, working hours, training quality, training assessments and the regulation of training.
Results
A majority of current FY trainees worked extra weekly hours with the breakdown being: 5–10 hrs (54%), 10–15 hrs (17%), >15 hrs (9%) and no extra weekly hours (20%). All current FY trainees wanted to work for more than 40 h a week with the following breakdown of desired hours: per week 40–48 (22%), 48–60 (50%) and 60–70 h (19%). The average hours per week spent clerking emergency admissions by current FY trainees were as follows: zero hours (11%), 0–5 h (37%), 5–10 h (30%), 10–15 h (11%) and greater (11%).
A large majority (90%) felt that it was possible for incompetent trainees to obtain satisfactory results from assessments and that the FY training program was poor at identifying failing trainees. There were high levels of dissatisfaction with the selection process.
Conclusions
FY training appears to be failing in several key areas with the lack of emergency exposure a particular area of concern. It is essential that any future reforms of training address these problem areas.
BD was a committee member of Remedy UK from 2008 to 2009. The authors declare no other competing interests
None
The survey did not require ethical approval according to the NRES guidelines
BD
BD and PD have been involved in all the following aspects of the work: conception and design, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published
Jeremy Brown
Background
Medical training in the UK has undergone many significant reorganizations in recent years and these look set to continue with Andrew Lansley's unpopular Health Bill, 1 although the consequences of this Bill for training remain unclear. 2 A crescendo moment in training reform came in 2007 when the Medical Training Application Service (MTAS) and Modernizing Medical Careers (MMC) provoked a march of junior doctors organized by Remedy UK. As part of MMC pre-registration house officer (PRHO) year had been replaced with two years of Foundation Year (FY) training, while the regulatory powers have shifted from the Royal Colleges to the GMC.
Prior to MMC's introduction of FY training, all medical graduates undertook basic PRHO training in both medicine and surgery whereby progress was assessed using logbooks and consultant reports. Proposals for competence-based training were conceived together by the Department of Health MMC Group, the Royal Colleges and then recently formed Postgraduate Medical Education and Training Board (PMETB) predicated upon tenets of trainee-centred, service-based, quality-assured, flexible, coached, structured and streamlined training.
The progression of a doctor through FY training seems now largely based upon gaining satisfactory competencies in various workplace-based assessments (WPBAs), including ‘mini’ clinical evaluation exercises (mini-CEX), case-based discussions (CbD), direct observation of procedural skills (DOPS) and 360° appraisals using ‘mini’ peer-assessment tools (mini-PAT). Such assessments are administered using the E-Portfolio which involves an online portfolio, including learning and educational agreements and the curricula relevant to this stage of training.
There have subsequently been many reviews of medical training, including those by Professors Tooke 3 and Collins, 4 with the latter focusing specifically on FY training. It has also recently been announced by National Health Service: Medical Education England that there is to be another independent review of medical training by Professor Greenaway.
In order to evaluate the impact of the FY training, an independent survey of doctors was undertaken. Certain aspects of the survey were specifically designed to test whether FY training was likely to be achieving the stated outcomes of the FY curriculum: 5
Foundation year 1 (Fl) enables medical graduates to begin to take supervised responsibility for patient care and consolidate the skills that they have learnt at medical school…. Foundation year 2 (F2) doctors remain under clinical supervision (as do all doctors in training) but take on increasing responsibility for patient care.
Methods
An Internet-based questionnaire was constructed and made available online (http://www.remedyuk.org). Likert items in five-ordered response levels were used where appropriate 6 and in addition there were some open spaces for free comment. The questionnaire was accessible for a four-month period from November 2011 to February 2012, details being distributed to doctors throughout the UK via email contacts, the medical Deaneries and other website notifications. Eligible participants were doctors in the UK who were either in training or involved in training. Demographic information regarding respondent grade of seniority, current specialty and UK region (training Deanery) was also gathered. Data was collated using established online survey design software (http://www.surveymonkey.com) and analysed. The survey was not of patients and therefore did not require ethics committee approval.
Results
Figure 1 illustrates the breakdown of respondents by grade. A total of 1065 doctors in training responded and 1042 of these doctors had been through FY training, of these 638 were current FY1 or FY2 doctors. Those responders who had not been through FY training were excluded. The results for the current FY doctors (n = 638) have been separated out from the remainder in several of the results sections and when this has been done it has been clearly mentioned. Respondents were also given the chance to comment in an open fashion and some of these comments have been selected for inclusion in the results section.
Grade of doctor in training
Response rates were evenly spread across the current FY1 and FY2 years. All Deaneries were represented, the greatest responses being received from London and the West Midlands. The majority of doctors in training who responded had started their FY1 year in either 2010 or 2011 (60%).
The FY selection process was rated by all past and present FY trainees (n = 1042) in the following areas: (1) fairness, (2) ease of use, (3) scoring system for word limited questions, (4) ability to reflect a candidate's abilities and (5) ability to apply for specific jobs of interest. General levels of dissatisfaction were high relating to all areas of the selection process other than ‘ease of use’. The ‘ability to reflect a candidate's abilities’ and the ‘scoring system for word limited questions’ received particularly poor feedback with 76% and 54% of respondents rating these as either ‘poor’ or ‘very poor’. The following respondent comments reflected how frustrated some doctors were with the selection process:
The MTAS application system is currently woefully inadequate as a method of actually scoring candidates on their ability.
And
See you all in Australia, where jobs are allocated on the basis of CV, references and interview – not on answering abstract questions on a form….
As regards working hours most current FY trainees (n = 638) reported that they worked their rostered hours or less than 10 extra hours of work per week (74.3%), while the majority of extra hours were related to service commitments (72%). Figure 2 shows the level of hours that current FY doctors (n = 638) would be prepared to work at most, assuming payment for extra hours worked. As regards maximum desired hours, not a single FY doctor wanted to work less than a 40 h week and the vast majority (78.3%) wanted to work beyond the European Working Time Directive (EWTD) limit of 48 h. The majority desire to work greater than 48 hours was common to doctors of all specialties including surgery, medicine, emergency medicine and general practice. This comment from one respondent reflected the desire to work more hours:
The maximum weekly hours desired by current Foundation Year doctors
Please put an end to the EWTD as it is severely detrimental to our Foundation training.
Figure 3 shows the average weekly number of hours spent clerking emergency admissions during the FY1 year for the different year of graduation. Overall 11% spent no time clerking emergency admissions and 37% spent less than five hours per week. There appears to be a worrying trend in this regard with an increasing proportion of FY doctors getting no emergency experience or less than five hours per week. The frustration with the lack of emergency exposure was reflected by the comment of this respondent:
Average weekly hours spent clerking emergency admission during Foundation Year 1 year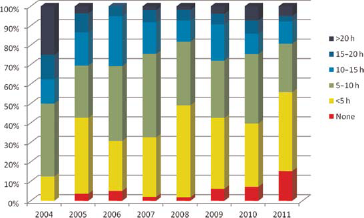
Where I work FY1s clerk very little, they get terrible experience. We have utterly lost our way in educating doctors.
Figure 4 shows the value attributed to the FY WBPAs (miniCEX, CbD, DOPS and miniPAT) by all past and present FY doctors (n = 1042). The general feeling regarding the WPBAs was mixed. Overall a small majority of doctors felt they were of ‘some’, ‘moderate’ or ‘great’ value (61.2%). However a significant minority felt the WPBAs to be of ‘little’ or ‘no’ value (38.8%). The emphasis on paperwork was remarked upon by one respondent:
The level of value attributed to the Foundation Year assessment tools
More focus seems to be put on the ability to fill in forms than actual clinical competence
The vast majority (90%) of past and present FY doctors (n = 1042) felt that incompetent trainees could obtain satisfactory results from the FY WPBAs. This comment from one respondent reflected the overall sentiment of many doctors:
It is all too obvious that trainees in my years of Foundation training and those going through it now are able to pass through even if they are not competent to pass.
Figure 5 shows the opinion of all past and present FY doctors (n = 1042) in training on the adequacy of the FY regulatory process.
Does the Foundation Year regulatory process give you an adequate opportunity to highlight any problems with your training?
Figure 6 shows respondents’ ratings (n = 1042) of the FY training process in the following areas: (1) training content, (2) relevance of job specialties, (3) sufficient clinical autonomy, (4) formal teaching, (5) supervision levels and (6) ability to identify failing trainees. Most aspects of FY training were rated reasonably well by trainees other than the ‘ability of the training program to identify failing trainees’ which over half (52.4%) felt was ‘weak’ or ‘poor’. The lack of training continuity was mentioned in a negative manner by some respondents:
Trainee satisfaction with different aspects of Foundation Year training
We get shipped around in a random fashion and never get to really know a team because the rotations are so short.
Discussion
In our understanding this is the largest independent survey of FY training ever undertaken, with over 1000 doctors with FY training experience responding. According to the GMC there are just over 50,000 doctors in training in the UK, of whom approximately 15,000 are FY doctors. Our survey does have some weaknesses. Firstly our response rate among FY doctors is around 5%, only a minority of the UK total, and there is consequently a significant sampling bias. One reason for this is the lack of cooperation offered by official training organizations such as Deaneries; for example, the high response rate in the West Midlands Deanery was likely related to their kind cooperation. Secondly, there is inevitably a significant selection bias given the methods of survey distribution via email contacts and the Internet. Those who participated are self-selecting and it is arguable that this group is more likely to be dissatisfied with FY training than those who did not respond.
Nonetheless our survey has highlighted several key problem areas in FY training which include the reduced working hours, a lack of exposure to emergency work, the selection process, the regulatory process and the use of the WPBAs. The most worrying finding was the significant proportion of FY doctors who were getting zero or minimal levels of emergency experience during their FY1 year. Certainly progress is being made in terms of using simulation in order to develop clinical skills at both an undergraduate and postgraduate level. 7 9 However it is vital that this progress is supported by a robustly regulated amount of core emergency exposure for trainees at both FY1 and FY2 level.
The Foundation curriculum's outcomes and measures of training quality are inherently vague, 5 meaning that there currently appears to be no formal mechanism for recognizing the fact that a large number of trainees are getting such minimal levels of exposure to emergency work. Prior to MMC the PRHO year was regulated robustly by the Royal Colleges in order to ensure that all house officers obtained core experience in the common medical and surgical emergencies. Our data would suggest that the shift of regulatory responsibility to the GMC, 10 in combination with an over emphasis on chronic disease management 3 have led to this core emergency experience being neglected.11,12 This is even more worrying given the concerns being raised about the acute care component of undergraduate medical training in the UK. 13 It is arguable that routine regulatory workplace visits need to be re-introduced to ensure that trainees are getting the necessary emergency exposure. 10 Certain vested interests groups appear to be indirectly lobbying for more input into the undergraduate and postgraduate medical curricula; 14 this has the potential to further dilute the emphasis on the core of acute medicine and surgery.
It is no surprise that a significant majority of FY doctors want to work in excess of the EWTD limit of 48 h per week and this is consistent with other survey data.15,16 The GMC national trainee survey has repeatedly shown that a significant percentage of both doctors in training and trainers feel the EWTD is continuing to have a significant negative impact upon training.12,17 The EWTD has resulted in reduced continuity for FY doctors both in terms of educational supervision and in terms of clinical training; when this is combined with the short nature of FY placements then one has a potential recipe for disaster both in terms of training and patient care. 12 The Temple report's remedy to the EWTD relies upon a significant service re-configuration and a large consultant expansion; 18 this is arguably completely impractical in the NHS's current financial situation.
The desire to work longer hours is surely related to the motivation of doctors in training to improve their training. Improving the continuity of training is important in order to maximize the valuable learning opportunities present during clinical work such as ward rounds and night shifts.12,19,20 The valuable formative element of WBPAs 21 is likely to be increased by increasing levels of training continuity. Another great area of concern is the apparent deficiencies in terms of identifying the ‘failing FY doctor’. A large majority felt that incompetent trainees could achieve satisfactory results from the WBPAs, while a large percentage of FY doctors felt that the regulatory process did not give them an adequate opportunity to highlight any training problems. This adds weight to the argument that the current WBPA process appears to lack integrity 22 and that WBPAs should not be relied upon to certify competence. 21
Doctors appear fairly content with FY training in certain areas; FY doctors are generally satisfied with formal teaching, levels of supervision, the training content of jobs and their level of clinical autonomy. There are notably high levels of engagement with the e-Portfolio and the E-Learning systems. 23 The exposure of FY doctors to primary care has also provided valuable learning opportunities. 24 These positive aspects of FY training undoubtedly deserve praise. The obvious failings of the selection process identified by our study are currently being addressed by the introduction of a situational judgment test (SJT) and an educational performance measure (EPM). It remains to be seen whether these changes will have a significant positive effect and it will be important to adequately survey all FY doctors as they are introduced. 25
In conclusion our survey has highlighted several key problems in FY training which include a lack of exposure to emergency work, training hours, the selection process, the regulatory process and the WPBAs. It is arguable that the current reliance upon competency-based methods of training such as WBPAs is not supported by any robust evidence26,27 and that the best means of improving training is to increase workings hours beyond the EWTD's 48 hour limit. The current emphasis on competency-based paperwork over clinical competence appears to be frustrating doctors. 27 In our opinion working hours should be increased beyond the current EWTD limit to a sensible level in the 50–60 hour/week region. Increasing hours would increase training continuity by enabling more of a team-based approach with more frequent trainer contact; it could also improve the continuity of care and consequently standards of care. Most importantly increased hours would lead to greater levels of experience and greater trainee confidence, both of which would likely result in more highly competent doctors of tomorrow. 12
A clearer separation of powers between the provision and regulation of training is needed to minimize the effects of potential conflicts of interest; the line between the provision and regulation of training appears too blurred in the current system. 10 We would argue that the regulatory system needs to be reformed so that it is inherently more democratic and more responsive to those involved in training on the frontline. There needs to be a renewed focus on emergency work for FY doctors and this can only be done with better regulation; the issue of the ‘failing FY doctor’ can arguably be addressed by increasing training continuity in tandem with a more effective system of regulation. It also appears that there need to be better mechanisms in place for FY doctors to feedback any problems that may be, whether they relate to low quality training posts or the selection procedure, so that they can be effectively acted upon. The reliance upon competency-based assessments to assess trainee and training quality is no substitute for training continuity and high quality educational supervision.
Overall the current level of trainee frustration with several aspects of FY training is concerning and should be acted upon. The government's current ‘unintelligible’ Health Bill 28 promises to further complicate the already confused regulation of medical training, meaning that any real solutions to these problems seem a long way off at the moment.
Footnotes
Acknowledgements
We would like to thank anyone who helped distribute the survey in particular the participating doctors in training and the West Midlands Deanery