
Abstract
Objectives
Chronic diseases are fast becoming the largest health burden in India. Despite this, their management in India has not been well studied. We aimed to systematically review the nature and efficacy of current management strategies for chronic obstructive pulmonary disease (COPD) in India.
Methods
We used database searches (MEDLINE, EMBASE, IndMED, CENTRAL and CINAHL), journal hand-searches, scanning of reference lists and contact with experts to identify studies for systematic review. We did not review management strategies aimed at chronic diseases more generally, nor management of acute exacerbations. Due to the heterogeneity of reviewed studies, meta-analysis was not appropriate. Thus, narrative methods were used.
Setting
India
Participants
All adult populations resident in India
Main outcome measures
1. Trialled interventions and outcomes
2. Extent and efficacy of current management strategies
3. Above outcomes by subgroup
Results
We found information regarding current management – particularly regarding the implementation of national guidelines and primary prevention – to be minimal. This led to difficulty in interpreting studies of management strategies, which were varied and generally of positive effect. Data regarding current management outcomes were very few.
Conclusions
The current understanding of management strategies for COPD in India is limited due to a lack of published data. Determination of the extent of current use of management guidelines, availability and use of treatment, and current primary prevention strategies would be useful. This would also provide evidence on which to interpret existing and future studies of management outcomes and novel interventions.
Keywords
Introduction
The recent and rapid increase in the prevalence of chronic disease is a global concern, but a particular threat to health systems in developing countries. Rising prevalence of chronic diseases could destabilize not only health systems but entire state economies, which has been acknowledged at the highest levels.1,2
DECLARATIONS
None
This review forms part of a project for which funding was awarded to AJM by the Association of Commonwealth Universities and the Royal College of Physicians of London. The funders played no role in study design, data collection or interpretation, the writing or dissemination of this review. The Department of Primary Care & Public Health at Imperial College London is grateful for support from the NIHR Collaboration for Leadership in Applied Health Research & Care (CLAHRC) Scheme, the NIHR Biomedical Research Centre scheme and the Imperial Centre for Patient Safety and Service Quality
As a review of existing data, ethical approval was not required
AJM
AJM, MPA and AM contributed to study design. Data were collected and analysed by AJM and RKKP. AJM, MPA and AM drafted/revised the article. The final version has been approved by all authors
Chronic obstructive pulmonary disease (COPD) is one of several diseases contributing to the rise of chronic illnesses. Typically it results from accumulated environmental exposure to particular irritants – the best established links being with smoking, and domestic and outdoor pollution. More recently, interactions between tuberculosis, HIV and smoking have become of increasingly greater concern, as aetiological factors, as cases of HIV, tuberculosis and co-infection have risen. 3
That COPD is largely environmentally-driven, and thus potentially preventable, is particularly important in the face of unfavourable epidemiological reports. COPD accounted for 5% of deaths globally in 2005, with most of these occurring in low- and middle-income countries, 4 and it is predicted to become the third leading cause of death by 2030. 5 The outlook may become even worse if COPD associated with HIV/tuberculosis-related lung disease proves to be relatively resistant to existing treatments, and if issues associated with poor nutrition (which appears to be associated with poorer outcomes) cannot be resolved. 6 As a chronic disease, COPD also accrues vast numbers of disability-adjusted life years (DALYs). Most of these arise in the World Bank's ‘South Asia’ and ‘East Asia’ regions. 7
India suffers among the highest number of DALYs due to COPD. 8 The prevalence of COPD in India is not well understood, but we recently suggested the best existing estimates for chronic bronchitis (a commonly used proxy) indicate that prevalence is between 6.5% and 7.7% in the adult population – although it is unlikely that this estimate would apply to all Indian subpopulations. 9 World Health Organization (WHO)-Government of India COPD management guidelines were produced in 2003, 7 but the extent of their implementation, and effect, are unknown. Outcomes have not obviously been reviewed or audited, and the guidance was largely drawn from similar international documents – based on outcomes from trialled interventions in populations from other, generally more developed countries.
Review aims
We aimed to review the current quality of management of COPD in India by addressing the following questions:
How is COPD in India currently managed? How effective is the current management of COPD in India?
Methods
The Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects (Cochrane Library), Database of Promoting Health Effectiveness Reviews (Evidence for Policy and Practice Information Centre) and Medline (via PubMed) were searched before conducting the review, on 30 October 2010, to ensure that there were no recent or ongoing reviews in the subject area. The review was then conducted according to the relevant aspects of the PRISMA guidance 10 and the guidance of the Centre for Reviews and Dissemination, York. 11
Following scoping searches a review protocol was developed describing the search strategy and methods for data collection and analysis. The review questions above were deconstructed to identify PICOS elements used to generate search terms (see Table 1). The search strategy was trialled before use to determine that existing related well-cited articles would be returned, and adaptations made where necessary.
PICOS identifiers from research questions (‘key terms’) and database – and thesaurus-derived alternatives (‘additional terms’) used to generate database searches
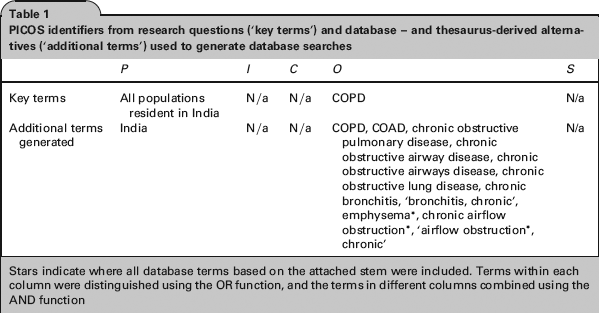
Stars indicate where all database terms based on the attached stem were included. Terms within each column were distinguished using the OR function, and the terms in different columns combined using the AND function
Search
The PICOS identifiers and related terms (Table 1) were used to search the Medline (via PubMed) and Embase (via Ovid) databases on 1 August 2011 (updated 22 December 2011), the IndMED database on 15 July 2012, Cochrane Central Register of Controlled Trials on 16 July 2012, and the CINAHL database on 24 July 2012. No restrictions were placed on language of publication, study design, publication type or publication status. Only studies published since 1980 were included, as our interest was in the recent situation, and earlier publications were also relatively few and difficult to access.
In addition, the available online contents (from 1980 onwards) of the journals Lung India and Indian Journal of Chest Diseases and Allied Sciences were hand-searched on 19 August 2011. Reference lists of included papers were scanned, as well as the references of relevant review articles/editorials identified in the search. Finally, we contacted experts in the field with the aim of identifying any additional or unpublished data. We did not include unpublished results available on trial databases as we felt unable to assess the data in a sufficiently useful manner, due to lack of information such as location and dates of study, methodology, length of follow-up and general analytical approach. Many of the trials recruited from multiple countries and data for India alone were not available. We also felt unable to interpret data regarding adverse events sufficiently well.
Selection
Inclusion/exclusion criteria for the results of the search are listed in Table 2.
Inclusion/exclusion criteria

COPD, chronic obstructive pulmonary disease
Two subsets of results pertaining to Question 1 were acquired – studies of primary and secondary prevention. The number of primary prevention studies returned was limited and we included them even though the interventions were not conceived to target COPD alone. In the series of secondary prevention studies returned, we made no exclusions based on intervention type, so long as the study pertained to the management of chronic, stable COPD, rather than acute events. Indeed, observation of the types of intervention pursued was of interest in itself. Similarly, regarding Question 2, we included studies of all measured outcomes, other than those relating to acute exacerbations alone.
To determine study eligibility, the titles and abstracts of all papers returned from the search were screened by one reviewer. The studies accepted at this point were reviewed fully, and progressed either to data extraction or exclusion. Those excluded were: reviews/editorials without additional analysis, studies wherein data were not COPD-specific, where populations were not representative of the general population, interventions were of acute management and/or studies were without actual trialled intervention, were not relevant, or not available (see Figure 1).
Flow chart demonstrating handling of papers returned by Searches 1 and 2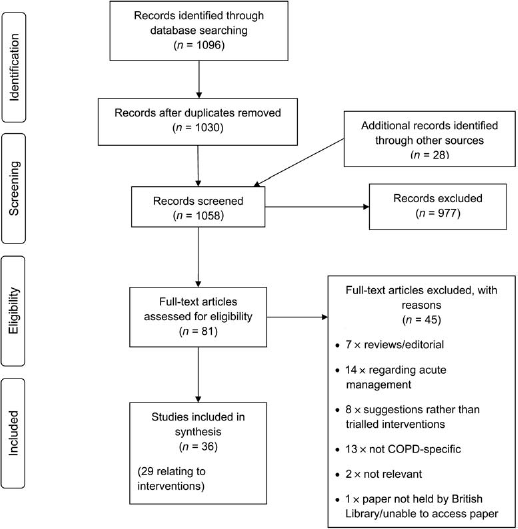
Data extraction
Data extraction was performed using two proformas – one for extraction of basic study data, one for quality assessment. The basic study data proforma was a modified version of the checklist recommended by the Centre for Reviews and Dissemination, York. 11 Our quality checklist has been used previously 9 and includes the ‘component ratings’ of the Effective Public Health Practice Project Quality Assessment Tool 12 and the bias assessment as recommended in the Cochrane Handbook. 13 It was used for all study types, with items omitted where not relevant. The proformas were tested on a subset of the papers, and iterations made, before being used for final data collection. The broad headings under which information was recorded for each study are listed in Box 1.
Data extraction and quality assessment checklists
The numbers beside the quality assessment criteria are used to indicate how quality for each criterion has been rated, in Tables 3–5.
Studies relating to primary prevention strategies for chronic obstructive pulmonary disease in India

Reviewed studies regarding primary prevention strategies relevant to chronic obstructive pulmonary disease (COPD). Study entered in italics of quality concern (see Methods), with the main reasons for concern noted in the ‘Quality’ column. The numbers following the different quality ‘levels’ (G, P, N) indicate the aspect of quality assessment (see Box 1), rated as good (G), poor (P) or not-assessable (N) WHO, World Health Organization; DALYs, disability adjusted life years
Studies relating to secondary prevention strategies for chronic obstructive pulmonary disease in India

Reviewed studies regarding secondary prevention strategies relevant to non-acute management of chronic obstructive pulmonary disease (COPD). Population characteristics are entered as available. Studies of quality concern (see Methods) are entered in italics, with the main concerns being noted in the ‘Quality’ column. The numbers following the different quality ‘levels’ (G, P, N) indicate the aspect of quality assessment (see Box 1), rated as good (G), poor (P) or not-assessable (N)
RCT, randomized controlled trial; SD, standard deviation; GOLD, = Global Initiative for Chronic Obstructive Lung Disease; WHO, World Health Organization; 6MWD, six-minute walk distance; 12MWD, 12-minute walk distance; CCQ, clinical COPD questionnaire; CRQ, chronic respiratory questionnaire (includes 4 domains: dyspnoea, fatigue, emotion and mastery); SGRQ, St George's respiratory questionnaire (designed to assess quality of life: impaired health and perceived wellbeing); MIP, maximum inspiratory mouth pressure; FVC, forced vital capacity; FEV1, forced expiratory volume in one second; PEFR, peak expiratory flow rate; ABG, arterial blood gas; CRP, C-reactive protein
Review of chronic obstructive pulmonary disease management outcomes in India

Reviewed studies regarding management outcomes relating to non-acute management of chronic obstructive pulmonary disease (COPD). All were cross-sectional studies. Population characteristics are entered as available. Studies of quality concern (see Methods) are entered in italics, with the main concerns being noted in the ‘Quality’ column. The numbers following the different quality ‘levels’ (G, P, N) indicate the aspect of quality assessment (see Box 1), rated as good (G), poor (P) or not-assessable (N)
GOLD, Global Initiative for Chronic Obstructive Lung Disease; PHQ-9, Patient Health Questionnaire-9; PEFR, peak expiratory flow rate; CB, chronic bronchitis
One reviewer carried out the data extraction for basic study data. The results were checked by a second reviewer and any concerns remedied by re-checking to reach a consensus decision. Two reviewers independently performed the extraction of quality data, before the results were collated. Inconsistencies were resolved as above.
Quality assessment
The extracted quality data were used to grade each aspect of the assessment as ‘good’, ‘poor’ or ‘nonassessable’. Again this rating was independently carried out by two reviewers. Disagreements were resolved by discussion and consensus decision. Where the combination of the number of ‘poor/non-assessable’ ratings and main reasons for concern were deemed sufficient to question the reliability of the study, the study was excluded from a secondary analysis (see below).
Data synthesis
As anticipated on preliminary searching, study designs were too heterogeneous to allow useful meta-analysis. Thus, a narrative approach was used. The data were summarized in tables, and analysed twice (before and after exclusion of studies where quality was of concern).
We aimed to assess each set of studies with regard to:
Number of studies and time-trends in production and quality.
We wanted to examine the management intervention studies to determine:
Types of intervention trialled and levels of success; Any peculiarities of intervention effect by subgroup (age, sex, urban/rural location, smoking status and exposure to domestic fuels).
And we aimed to examine the management outcome studies to determine:
Outcome measures used; Extent and efficacy of current management strategies; Any differences in outcomes by subgroup.
Proposals were formed based on general initial analysis outcomes, and inconsistencies examined. Finally, comparisons between results of the analyses were made before and after studies with quality concerns were excluded. Where data were insufficient to allow narrative synthesis, display and discussion of the data was used.
Results
The search produced 1096 papers for review. Figure 1 displays the handling of the search results.
The data extracted from each of the studies are summarized by question theme in Table 3 (primary prevention management interventions), Table 4 (secondary prevention management interventions) and Table 5 (management outcomes). The data excluded from the second analyses (due to quality concerns – see Methods), are italicized, and the main quality concerns noted.
Management I – interventions
Twenty-nine studies of interventions were identified – two relating to primary prevention and 27 to secondary prevention. Other than two studies published in the 1980s, and three in the 1990s, all had been published within the last decade. Generally, more recent studies had higher-quality scores.
Regarding the two primary prevention studies – neither was a clear, trialled and audited study, and neither was conceived to address COPD alone. Although one 14 scored well on quality assessment, it was a theoretical study, with the associated uncertainties. The second 15 was a conference abstract, with poor-quality scores, and difficulty in interpretation limited its use.
The 27 studies investigating secondary prevention interventions showed much variety in intervention type, study setting and outcome measures. There were 17 pharmacological interventions, three pulmonary rehabilitation interventions, five others involving exercise training, one trial of influenza vaccination and one study of the World Health Organisation-Government of India guidelines. All were assessed using intermediate clinical outcome measures. The guidelines and vaccination interventions were assessed using a quality-of-life questionnaire and exacerbation frequency, respectively. The other categories of intervention were each assessed by a combination of spirometry, exercise capacity and other physical measures, as well as quality-of-life scores.
Of the trialled interventions, only six had negative outcomes,21,25,27,32,35 and of those with positive outcomes, only the implementation of the WHO-Government of India guidelines was potentially still ongoing. Indeed, in several cases the follow-up was so limited that the relevance of the intervention was unclear.21,23,35,38,41 The clinical relevance of the changes rendered by some studies20,23,32,33,42 was also unclear.
Discounting these studies of questionable relevance, and those with quality concerns, only 10 studies of relatively high usability were left.16,18,19,24,26,29,30,34,37,40 Notably, all of these studies had positive outcomes, but they were of varied intervention type (5 pharmacological, 2 pulmonary rehabilitation, 2 other exercise interventions and 1 regarding vaccines), and each was confined to a particular geographical area. Their generalizability was therefore limited. Four of the studies (of bronchodilator use and pulmonary rehabilitation) were of interventions already recommended in Indian guidelines. Although subgroup outcomes are of interest with regard to disease patterns and targeting interventions, the low number and heterogeneity of studies did not permit such investigation.
Management II – outcomes
Seven studies relating to outcomes were identified – two from the 1980s, one from the 1990s and four more recent. Again fewer quality concerns were associated with more recent studies. Many outcomes were considered: prevalence of depression, cor pulmonale, osteopaenia and osteoporosis, disability and distress scores, mortality data and management of smoking. The only process measures investigated were some relating to management of smoking.
COPD was associated with relatively high levels of depression, disability and distress.43,46 It was the second commonest cause of death generally, and the highest in older age groups. 45 The observed extent of right ventricular failure/cor pulmonale was low – but both of the investigating studies were relatively dated.48,49 The prevalences of osteoporosis and osteopaenia were insufficiently different from estimates of general populations of the same age to be able to convincingly suggest a difference in the absence of a control group. 44 The study relating to education and treatment of smoking had some quality concerns, but suggested that only 88.7% of patients received cessation advice, and one-third of patients were unaware of the association between COPD and smoking. 47 Excluding studies with quality concerns, only those investigating depression, disability and distress remained.
Discussion
Principal findings
We planned an investigation to determine the extent and efficacy of the management of COPD in India. An important observation was the paucity of data and inconsistency in study setting and population characteristics. This is in contrast to some other states, such as in England, where national studies have demonstrated the availability/efficacy of current management across the region. 50 Study quality was also variable and of concern in 19/36 cases, but improved in recent years. These issues so impacted on analysis that we were unable to draw conclusions regarding efficacy of management under current strategies, and the extent of applicability of trialled interventions.
Data regarding management outcomes were particularly lacking. Of the few available studies, many were not conceived with this in mind, the studies were few and disparate and only two were deemed of reliable quality. They were certainly suggestive that outcomes are suboptimal, but being carried out on various ill-defined management backgrounds and varied populations, over an extended time-period, their degree of general applicability is relatively unknown.
Uncertainty is again an issue in interpretation of the review of management interventions – almost all of which showed success in at least some outcome measures. This is especially so when, for example, pulmonary rehabilitation (a component of current guidelines) remains a subject of investigation and generates a positive response. Such data – and the one study of process measures suggestive that smoking cessation advice (another component of the guidelines) is not consistently delivered 44 – emphasize the need for the extent of current guideline implementation to be understood, before studies such as those reviewed can be most usefully applied.
The issue of the optimal extent of generalization of trialled interventions is in many respects premature. However, subgroup differences in disease prevalence, nature and course will exist, differential management strategies may be useful, and this can be usefully borne in mind as investigations continue.
Strengths and weaknesses of this study
Although the low number and heterogeneity of the reviewed studies were a notable outcome in themselves, they did have a considerable effect on the extent to which this review could be undertaken as planned. Further limitations on our results were imposed by (1) aspects of the review methodology and (2) our decision not to include unpublished data from trial databases.
The methodology was constrained in particular by the subjective nature of the quality assessment, and the lack of appropriateness of data for meta-analysis. The data were insufficient even for narrative synthesis in some areas of investigation. Regarding our decision not to include data from trial databases, we accept that our thus relatively constrained inclusion criteria may have increased the possibility of reporting bias. Indeed the observed outcomes regarding management interventions would allow that these data may have been at risk of publication bias.
We hope, though, that our thorough, systematic approach has identified most of the available data, and helped to provide a useful, clear summary, demonstrative of where the gaps in knowledge lie.
Interpretation of findings in relation to previously published work
Comparing outcomes of COPD management in India with those elsewhere is hindered mainly by the paucity of data. The management guidelines utilized in India are based on those recommended by international bodies and utilized elsewhere. They reflect disease pattern and context in India to an extent, 51 but do not really reflect that the included strategies tend to have been developed from study of populations resident in more developed states, and that the extent to which they can be similarly applied to other populations – including Indian populations – is unclear. The reviewed intervention and outcome studies are indicative that aspects of the current programme should be beneficial, but further study is required to determine that the guidelines are sufficiently effective in this population, and to investigate any subpopulation subtleties with regard to treatment outcomes. For example, the nature of the disease associated with domestic, and other environmental, pollution (relatively prevalent in this population) – rather than that associated with smoking – is less well characterized. Similarly, the nature of the disease when associated with HIV/tuberculosis is unclear, 3 and issues such as poor nutrition may well be of relevance to management. 6
Study of primary prevention was conspicuously lacking. The existing management guidelines do include reduction of risk factors, but these need to be implemented as more general societal measures (i.e. as primary rather than secondary prevention), and it is not clear that this is being achieved. Although a smoking ban was introduced in India in 2008, media reports of successful implementation of the ban are mixed. Ensuring achievement of the ban is a priority, and additional programmes such as those modelled by Wilkinson et al. 14 and further demotion of smoking activities, would be of use. The reviewed study of a smoking cessation programme 15 was difficult to interpret, but it is likely cessation programmes would be usefully applied – particularly when associated with an education component – for which there is an evident need.47,52 A review of smoking cessation programmes in India, their outcomes and associated research, would probably be useful.
Implications for future research, policy and practice
Although many of the studies reviewed here do contain potentially useful management strategies, these options, and others, could be better assessed and implemented if the distribution and success of current management was better understood. It might be useful to initially:
Achieve a better understanding of disease prevalence and likely trends in prevalence, as we have recently suggested;
9
Audit the use of guidelines – in terms of both process and clinical outcomes – across the country; Estimate the proportion of the population accessing healthcare services, and the proportion to which optimal/guideline care is available and taken-up.
This information would provide a useful background on which study of more subtle themes – such as those relating to the nature of disease among subgroups, and how best to target resources – could be based.
In the interim, the lack of data should not preclude the implementation of potentially useful interventions. Our review has shown that many secondary prevention methods would be beneficial, and that primary prevention methods are especially needed, and could be usefully implemented with ongoing review. In addition to consideration of change in domestic fuel use and tackling the extent of smoking, occupational health is another important primary prevention issue. In our review, we excluded studies investigating occupational groups alone, but several occupational groups are understood to be at relatively great risk, 53 and need particular attention, especially in terms of preventive interventions.
Conclusions
Investigation of the current extent of management of COPD in India is hindered by the number and nature of studies available. High-quality current data from a cross-section of the population is required if the current quality of management is to be determined at a level useful for policy considerations. An understanding of the extent of implementation of national guidelines would be particularly useful, and it would also be helpful to understand the current use of important preventive measures, particularly those targeting smoking, domestic fuel use and occupational risk. This would provide a useful background on which the efficacy of further management strategies – including some of those successfully trialled to date – could be usefully examined. The specific needs of subgroups could also then be further investigated and addressed.
In addition, optimal longterm solutions will require provision of more comprehensive prevalence estimates than are currently available, review of the changing context of service delivery and implementation of a more general approach to chronic disease management.
Footnotes
Acknowledgements
The authors would like to thank Lambert Felix, who kindly performed the CINAHL database search
Appendix
QUOROM Statement checklist