
Abstract
Vascular involvement in Behçet’s disease (BD) occurs in up to 50% of patients. The main mechanism of thrombosis is inflammation. Thus, immunosuppressants (IS) are the mainstay of therapy, and adding anticoagulation (AC) is controversial. In daily practice, we observed that patients who received AC in combination with IS experienced less recurrent thrombosis and decided to investigate our BD patients retrospectively. We hypothesized that adding AC to immunosuppressive therapy may lower the risk of recurrent thrombosis. Treatment at the time of first or recurrent thrombotic events was recorded. Events under the only IS and IS + AC treatments were compared. There were 40 patients (33 males). The most common types of first vascular events were deep vein thrombosis (77.5%) followed by pulmonary embolism (PE) (52.5%). One patient did not receive any treatment. Among the 39 patients, 32 received glucocorticoid and at least one of the azathioprine, or cyclophosphamide, anti-TNF, 5 received monotherapy with azathioprine, 1 received monotherapy with corticosteroid, and the remaining 1 received monotherapy with cyclophosphamide. In total, 22 patients (55%) experienced 27 recurrent venous thromboembolism (VTE) events. Two (7.4%) events while only on AC, 2 (7.4%) events while on AC + IS, and 15 (55.5%) events occurred while on only IS. Eight (19.6%) patients were not receiving any treatment during relapses. The recurrence rate was statistically significantly lower in the IS + AC treatment group compared to IS alone. In conclusion, IS are the mainstay of treatment for BD, and adding AC may help to lower the recurrence risk of thrombotic events.
Introduction
Behçet’s disease (BD) is a systemic inflammatory disease. Vascular involvement occurs in up to 50% of patients. 1 Venous thrombosis is the most common form of vascular Behçet’s disease (VBD). 2 Vascular wall inflammation results in thrombi formation, which is attached to the vessel wall. This is called “thrombo-inflammation.” 2 The main mechanism of thrombosis is inflammation rather than hypercoagulability, and the risk of embolization is low; thus, immunosuppressants (IS) are the mainstay of therapy. Adding anticoagulation (AC) to IS is controversial. 3
However, in daily practice, we observed that adding AC to IS decreases the recurrence rates. Here we present the clinical characteristics and recurrence rates in VBD.
Methods
In this retrospective study, the medical files of patients with VBD were analyzed. BD was defined according to the International Study Group for Behçet’s Disease (ISGBD) 4 diagnostic criteria and the International Team for the Revision of the International Criteria for Behçet’s Disease (ITR-ICBD) diagnostic criteria. 5 The diagnosis of first and recurrent thrombosis was based on Doppler ultrasound and/or computed tomography pulmonary angiography (CTPA). Venous thrombosis recurrence was defined as a propagation in the extent of thrombosis or the development of new thrombotic events.
Statistical analysis
Categorical data were expressed as numbers (%). Treatment at the first or recurrent events was recorded as IS, IS + AC, AC, or no treatment. Events under the only IS and IS + AC treatments were compared. The association between groups was examined by the chi-square test for categorical data. Data entry and analysis were performed using the IBM SPSS Statistics (Version 22.0., IBM Corp., Armonk, NY, USA). The statistical significance level was expressed as p < 0.05 for all tests.
Results
There were 40 patients (33 males). The ages at diagnosis were 15–47 years. The median follow-up time was 72 months (12–192). Five patients had a family history of BD. Three patients were receiving IS due to other organ involvement during the first vascular event.
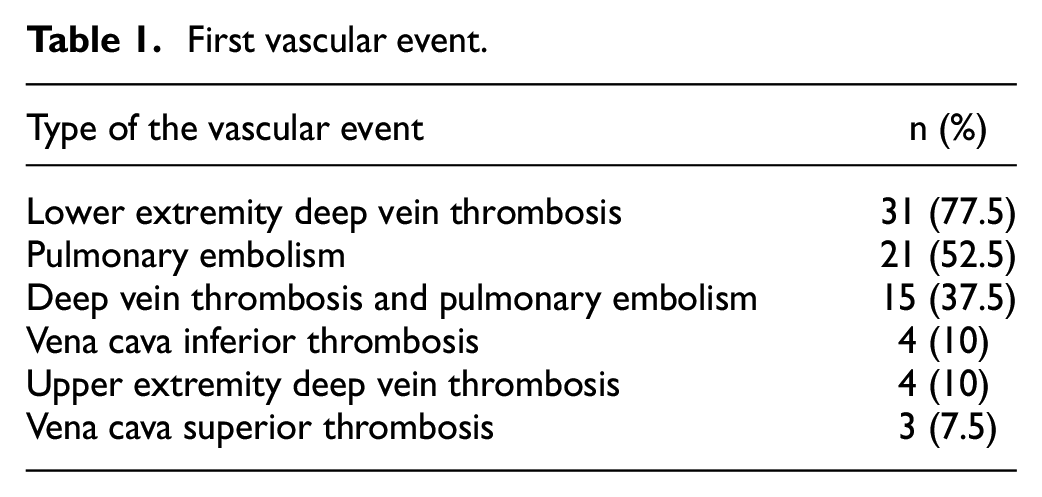
The most common type of first vascular event was deep vein thrombosis, followed by pulmonary embolism (PE). 37.5% of patients had concomitant deep vein thrombosis (DVT) and PE (Table 1).
First vascular event.
In all, 24 patients were tested for thrombophilia. Five patients (20.8%) had genetic mutations: one combined homozygous factor V Leiden (FVL) and homozygous prothrombin (PT) gene mutation, one homozygous FVL gene mutation, one heterozygous FVL gene mutation, and two heterozygous PT gene mutations. All of these patients had recurrent thrombosis under IS treatment. None of the patients had any other major risk factors like recent surgery, active cancer, etc.
One patient did not receive any treatment. Among the remaining 39 patients, 32 received glucocorticoid and at least one of the azathioprine, or cyclophosphamide, anti-TNF, 5 received monotherapy with azathioprine, 1 received monotherapy with corticosteroid, and the remaining 1 received monotherapy with cyclophosphamide. In total, 22 received AC in different durations.
Eighteen (45%) patients did not experience recurrent thrombosis. Among them, 7 patients received IS, and 11 received IS + AC. Total of 22 patients (55%) experienced 27 recurrent venous thromboembolism (VTE) events. Two (7.4%) events while on AC, 2 (7.4%) events while on AC + IS, and 15 (55.5%) events occurred while on only IS. At the time of relapses, eight (19.6%) patients did not receive any treatment (Figure 1). The recurrence rate was statistically significantly lower in the IS + AC treatment group compared to IS alone (Table 2). Ten recurrent events occurred as DVT + PE (three without treatment, five on IS, and two on AC treatment).
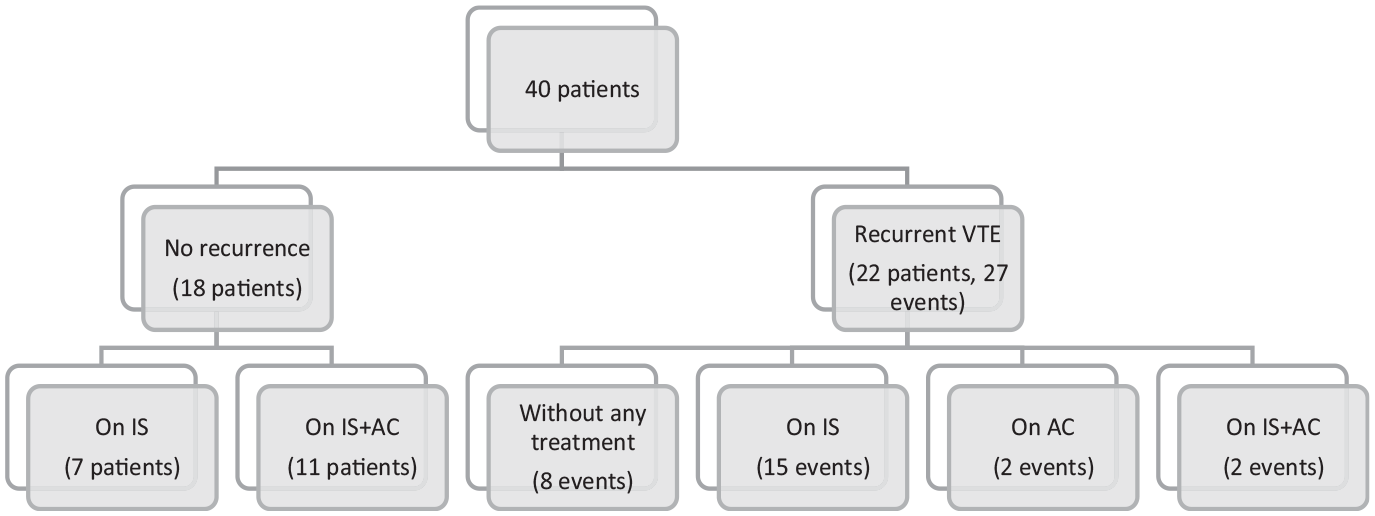
Distribution of patients.
Recurrence rates on immunosuppressive treatment with and without anticoagulation.
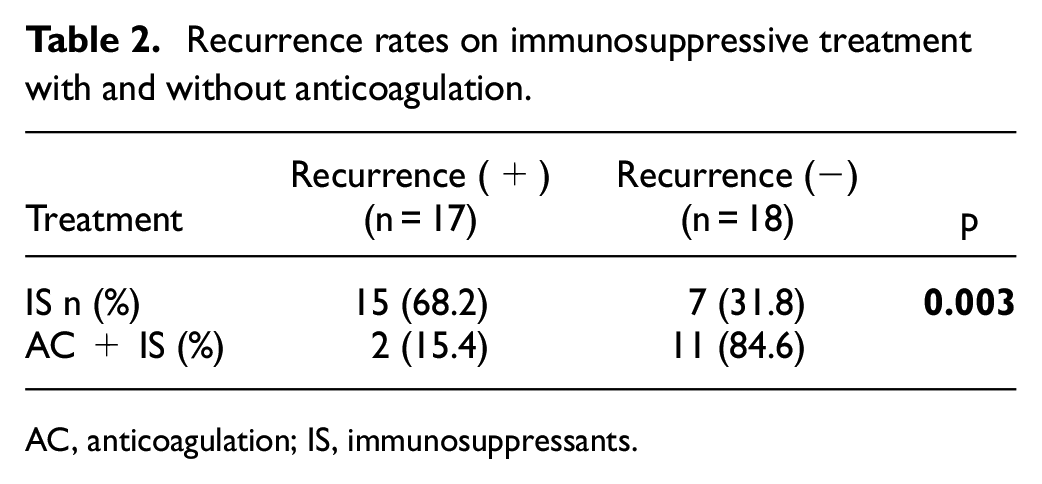
AC, anticoagulation; IS, immunosuppressants.
There were seven patients with vena cava (VC) thrombosis. Five of them were treated with AC in addition to IS, and two patients experienced thrombosis (one with AC and one without AC). One PE patient required systemic thrombolytic therapy due to massive PE. Six patients had hemoptysis. None of these patients had pulmonary aneurysms. One patient had minor gastric bleeding under AC treatment. None of these patients require hospitalization, treatment change, or blood transfusion due to complications. During follow-up, three patients died. One due to cancer, one due to sepsis, and the last one found dead at home possibly due to PE. However, the definitive cause of death could not be identified.
Discussion
In VBD, the role of IS therapy is well acknowledged. None of the previous studies showed any benefit of anticoagulation in preventing recurrent VTE.6–9 However, contrary to these studies, we found that adding AC to IS statistically significantly reduces recurrent thrombotic events.
There may be some explanations for different results. Tshumi et al. showed 10 that the risk of pulmonary embolization derived from DVT may be higher than expected. Also, some previous studies reported concurrent DVT and PE7,11–13 despite IS treatment. In line with these studies in our cohort, 5 of the 15 recurrent events on IS treatment were concomitant DVT and PE. One of these patients experienced clinical worsening despite corticosteroid therapy, and CTPA showed progression of PE (Figure 2(a) and (b)). EULAR 2018 update 3 recommends glucocorticoids and immunosuppressives such as azathioprine, cyclophosphamide, or cyclosporine-A for managing acute DVT. Thus, monotherapy with glucocorticoids may not be considered adequate treatment.
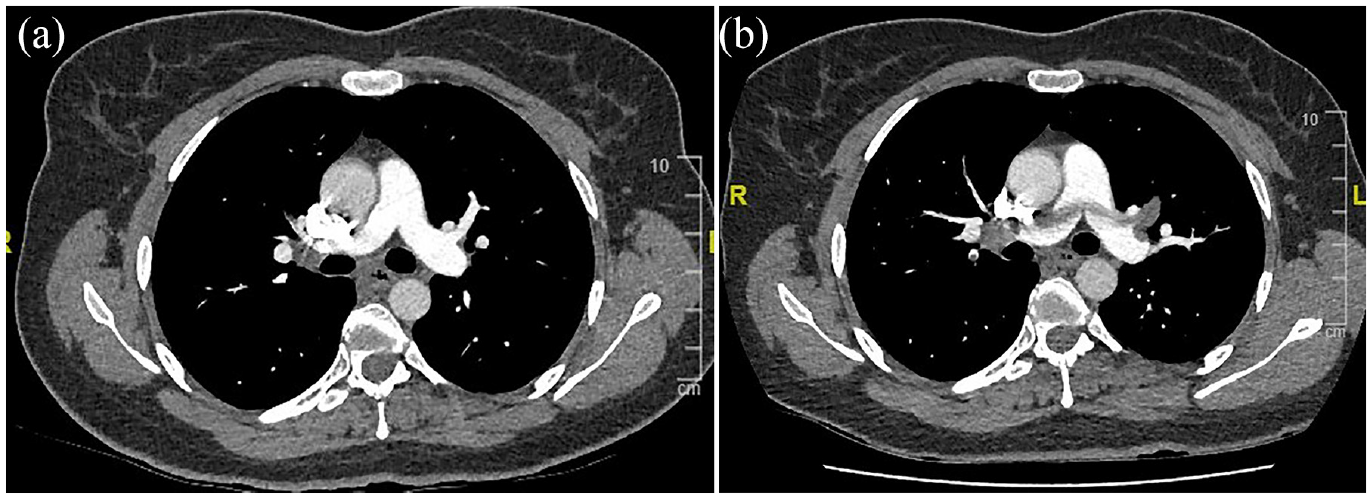
(a) A 36-year-old female patient with known VBD had concomitant DVT and PE. She was started on corticosteroid treatment. (b) One month later, she was admitted to emergency service with worsening dyspnea. CTPA showed saddle PE and anticoagulation was added to IS treatment.
Of course, as Emmi et al. stated, 15 concomitant DVT and PE might be due to an inflammatory process that affects both arteries and veins. However, concomitant recurrent DVT and PE without accompanying pulmonary artery aneurysm despite IS treatment increases the possibility of hypercoagulability and embolization from venous thrombosis.
Furthermore, some studies reported risk factors for VTE. Rates of provoked VTE were 17.8% 11 and 8% 14 in these studies. There were not any major risk factors such as surgery, cancer, or trauma for VTE in our study population at the time of thrombosis. However, it is possible that minor risk factors were not questioned or written, and due to retrospective design, we were unable to identify them. In some studies, patients had underlying thrombophilia.8,9,11 Combined forms of these thrombophilias may have a role in recurrent thrombotic events. 15 In our study, there were five patients with gene mutations, and all of them had recurrent thrombosis. The role of thrombophilia, especially heterozygous mutations, in the recurrence is controversial. However, thrombophilia with systemic inflammation might increase the risk of thrombosis. Inflammation itself is a procoagulant factor, and active autoimmune diseases have an intermediate (3%–8% per year) risk of recurrent VTE. 16 Ahn et al. 6 and Wu et al. 12 showed that patients who experienced recurrent VTE had increased acute phase reactants. So, increased systemic inflammation may be triggering both thrombi-inflammation and hypercoagulability. Case reports and recent studies17,18 report successful prevention of recurrence of VTE with AC. As a result, these findings support the possibility of embolization and hypercoagulability during the vascular event. Possibly due to growing evidence provided by recent studies, the French position statement recommends consideration of anticoagulation during the acute phase. 19
In seven patients, bleeding occurred in our study. None of them required hospitalization or blood transfusion. Previous studies also reported low rates of bleeding complications due to anticoagulation.7,8,11,14,17,18 It seems that BD does not increase the risk of bleeding. However, we have to mention that patients with artery aneurysms did not receive anticoagulation in most studies.
The VC is one of the atypical sites where venous thrombosis occurs. The EULAR recommendations are similar for VC and DVT. 3 Anticoagulation, in addition to immunosuppressive treatment, may lower the recurrence in these patients as reported by Hamzaoui et al. 20 In this study, the outcome was good in 12 cases. However, in four cases, an extension of thrombosis occurred. In our study, out of seven patients with VC thrombosis, two experienced recurrent thrombosis: one with AC and the other without AC.
The main limitations of the study are the limited number of patients and the retrospective design. The identification of treatment duration and adherence, drug dosage, or provoking factors for thrombosis is difficult in retrospective studies. Thus, for evidence-based recommendations, we need randomized, well-powered controlled trials.
In conclusion, though IS are the mainstay of treatment for VBD, adding AC may help to lower the recurrence risk of VTE.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.