
Abstract
Objective
Every patient has a perception about surgery and psychological preparation of the patient has an important impact on their postoperative recovery and outcome. In this study we looked at impact of a visual educational aid, in the form of a patient DVD on outcome following colorectal surgery within an enhanced recovery programme (ERP).
Design
We carried out a prospective analysis of a consecutive series of patients undergoing elective colorectal resection. All patients were given information about their operation in a clinic setting. Our intervention included a 15 minute patient educational video describing the preoperative assessment, post-operative recovery and advice on discharge. A questionnaire on patients’ views of ERP and video education was given on discharge.
Setting
University teaching hospital
Participants
Patients undergoing elective colorectal resection
Main Outcome Measures
Outcomes studied included length of hospital stay, patient perception of ERP, postoperative complications and readmissions:
Results
Thirty-two patients underwent elective colorectal surgery over a 3 month period. Median length of stay in hospital was 5 days. The questionnaire response rate was 100%. All patients thought they were well informed of the enhanced recovery programme. Eighty-eight percent responded that the video information provided about their operation was adequate, with 28% finding the video very helpful and more useful than other forms of patient information. There were no major postoperative complications and no readmissions.
Conclusion
Audiovisual presentation in the form of a patient video is a useful tool in the psychological preparation of patients undergoing colorectal surgery.
DECLARATIONS
None declared
The preparation of the video was funded by an educational grant from Coloplast UK
The study was approved by East Midlands Ethics Committee
SC
All authors have contributed to the research study and the preparation of this manuscipt
Tariq Ismail
Introduction
Psychological preparation for surgery has been shown to have a positive impact on short-term recovery. 1 It is beneficial in clinical and behavioural recovery pain management, length of hospital stay and patient satisfaction. Psychological preparation incorporates a range of strategies with dissemination of information as one of the key elements. It influences attitudes including confidence, degree of analgesic use and return to normal activities. 2 Patients give very high importance to the information given to them by health professionals. Information can be given orally (face-to-face), through printed information or through use of a video. Traditionally, reliance has been on the use of written material as an adjunct to patient education in clinic, but in the current era of digital media there is scope for its utilization for patient education.
Enhanced recovery programmes have become increasingly popular following major abdominal surgery. These programmes optimize preoperative, perioperative and postoperative factors to reduce the physiological and psychological stress of surgery with the aim of improving patient outcome and speeding up recovery after surgery. There is evidence that the clinical improvements resulting from the implementation of an enhanced recovery programme do not cause significant deterioration in quality of life or transfer costs to another component of healthcare. 3
Good patient information and education is an important part of all enhanced recovery programmes, and gives confidence and improves overall outcome. We studied the use of patient video as an educational tool on the outcome after colorectal surgery within an enhanced recovery programme (ERP).
Methods
We carried out a prospective study of a consecutive series of patients undergoing elective colorectal resection over a 3-month period. Patients who were excluded from the study were patients with severe physical disability and those who could not speak or understand English. Only 1 patient (3%) was excluded for this reason.
Patients were given information about their operation and recovery face-to-face in a clinic setting by doctors and nurses, along with printed patient information booklets. Our intervention included a 15-minute patient educational video that explained their preoperative assessment and recovery after surgery including postoperative advice on discharge. They were allowed clear fluids and carbohydrate drinks for up to 2 hours before their operation. Patients undergoing right hemicolectomy did not receive bowel preparation, while those having left sided surgery received a low residue diet with 3 days of senna tablets and phosphate enema on the morning of surgery. All patients received antibiotic and DVT prophylaxis and no nasogastric tubes were used.
Postoperative analgesia included either patient controlled morphine infusion or epidural analgesia for 48 hours. Patients were also given regular paracetamol and NSAIDs with tramadol used for breakthrough pain. Oral fluids were immediately commenced postoperatively and normal diet encouraged from day 1. Chest physiotherapy and active mobilization was commenced on day 1. Patients had to be fully mobile, apyrexial, passing flatus or faeces and using oral analgesics only for pain before being considered for discharge. A questionnaire was given to patients on discharge to complete. The questionnaire was used to obtain patient feedback on their perception of ERP, use of video education and their views on the best medium for patient education (Figure 1). The questionnaire was to be sent back by post or brought by patients to clinic at the 4-week review.
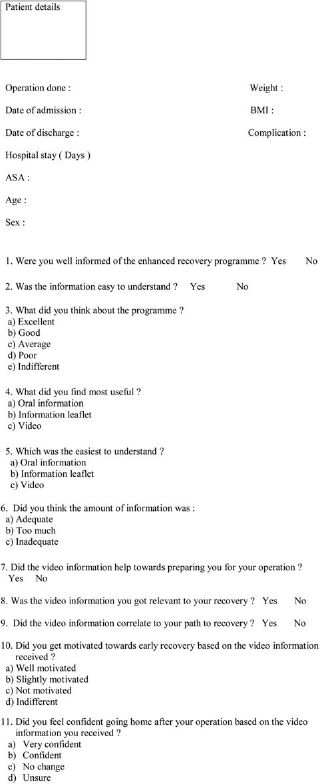
Patient Questionnaire
Results
During the study period, 32 patients underwent elective colorectal surgery and a fast-track recovery protocol was employed in all patients. Of these, 15 patients had laparoscopic assisted colorectal resection (4 right hemicolectomies, 4 left hemicolectomies, 3 anterior resections, 2 abdominoperineal resections, 1 proctectomy and 1 reversal of hartmann's) and 17 had open colorectal resection (3 left hemicolectomies, 7 anterior resections, 2 abdominoperineal resections, 2 proctectomies, 2 subtotal colectomies and 1 hartmann's). There were 20 males and 12 females with a median age of 62 yrs (Range 25–87). Median BMI was 27.5 (Range 22–35). Median length of stay in hospital was 5 days (Range 3–29 days).
We recorded 100% compliance rate for completing the questionnaires.
Table 1 summarizes the results for the various questions asked. All patients (100%) thought they were well informed of the enhanced recovery programme and the provided information was easy to understand. In terms of patient perception about ERR 14 (44%) patients thought the enhanced recovery programme was excellent, 14 (44%) thought it was good, 3 (9%) thought it was average and 1 (3%) thought it was poor.
Summary of result from the questionnaire
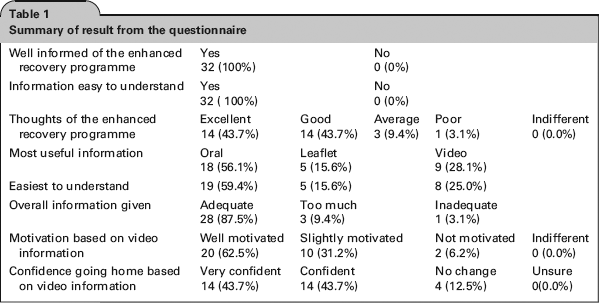
When asked about the effectiveness of different methods used for providing patient education, 18 (56%) patients found oral information as the most useful while 9 (28%) found the video most useful and 5 (16%) found printed information most useful. In terms of the easiest form of information to understand, 19 (59%) thought it was oral information while 8 (25%) thought it was the video and 5 (16%) thought it was printed information.
Overall, 28 (88%) patients thought all the information provided to them about their operation was adequate, 3 (9%) thought it was too much and 1 (3%) thought it was inadequate.
In terms of helping them prepare for their operation, 31 (97%) patients thought the video information was helpful, while 1 (3%) patient thought it did not help. A total of 29 (91%) patients thought the video information they got was relevant to their recovery while 3 (9%) did not think so. When asked if the video helped to motivate them to mobilize early, 20 (63%) patients felt well motivated, 10 (31%) patients felt slightly motivated and 2 (6%) patients did not feel motivated. When asked about confidence levels on discharge, 14 (44%) felt very confident, 14 (44%) felt confident and 4 (13%) felt no change in confidence.
Discussion
Psychological preparation and patient education are important aspects of a patient's experience of a surgical operation. The argument for adopting an effective pre-operative preparation is based around the improvements in patient recovery through reduced analgesic use, reduced complications, reduced hospitalization time, and enhanced quality of life and immune responses.1,4,5
With the introduction of the enhanced recovery programme, significant improvements in perioperative care have been reported. These programmes reduce the physiological and psychological stress of surgery with the aim of improving patient outcome and speed up recovery after surgery. This multimodal approach reduces hospital stay to 2–4 days. 6 The relative contribution of each of the single elements in the enhanced recovery programme remains uncertain. Patient education undoubtedly has advantages in terms of reducing anxiety. Good patient information gives confidence and improves overall outcome. Information can be given verbally, through use of printed material or use of audiovisual materials. Our intervention included use of a video. Preoperative educational video is effective in reducing anxiety and stress associated with surgery as well as reducing individual and overall medical costs7,8
Our study shows that most patients are well informed of the enhanced recovery programme and think it is beneficial. Oral information provided face-to-face in clinics was assessed as the best format, whilst video was a better source of information compared to printed material. Supplementing video education with both oral and printed information may well be better in preparing patients psychologically for surgery and help improve short-term outcomes in an enhanced recovery programme. Furthermore, in an ethnically diverse population, dubbing a video into different languages or using subtitles may also prove beneficial.
Surveying one's patients can lead to an overstated positive feedback and this can be looked at as a weakness of the study
Randomized trials are needed to prove the efficacy of video education as a component of the enhanced recovery programme and its subsequent incorporation into routine clinical practice.
Footnotes
Acknowledgments
None