
Abstract
This case report summarizes a diagnostic approach to unilateral hyperlucency in company with a rare case.
DECLARATIONS
None declared
None
Written informed consent to publication was obtained from the patient or next of kin
Both authors contributed equally
Robert Mallinson
Case Report
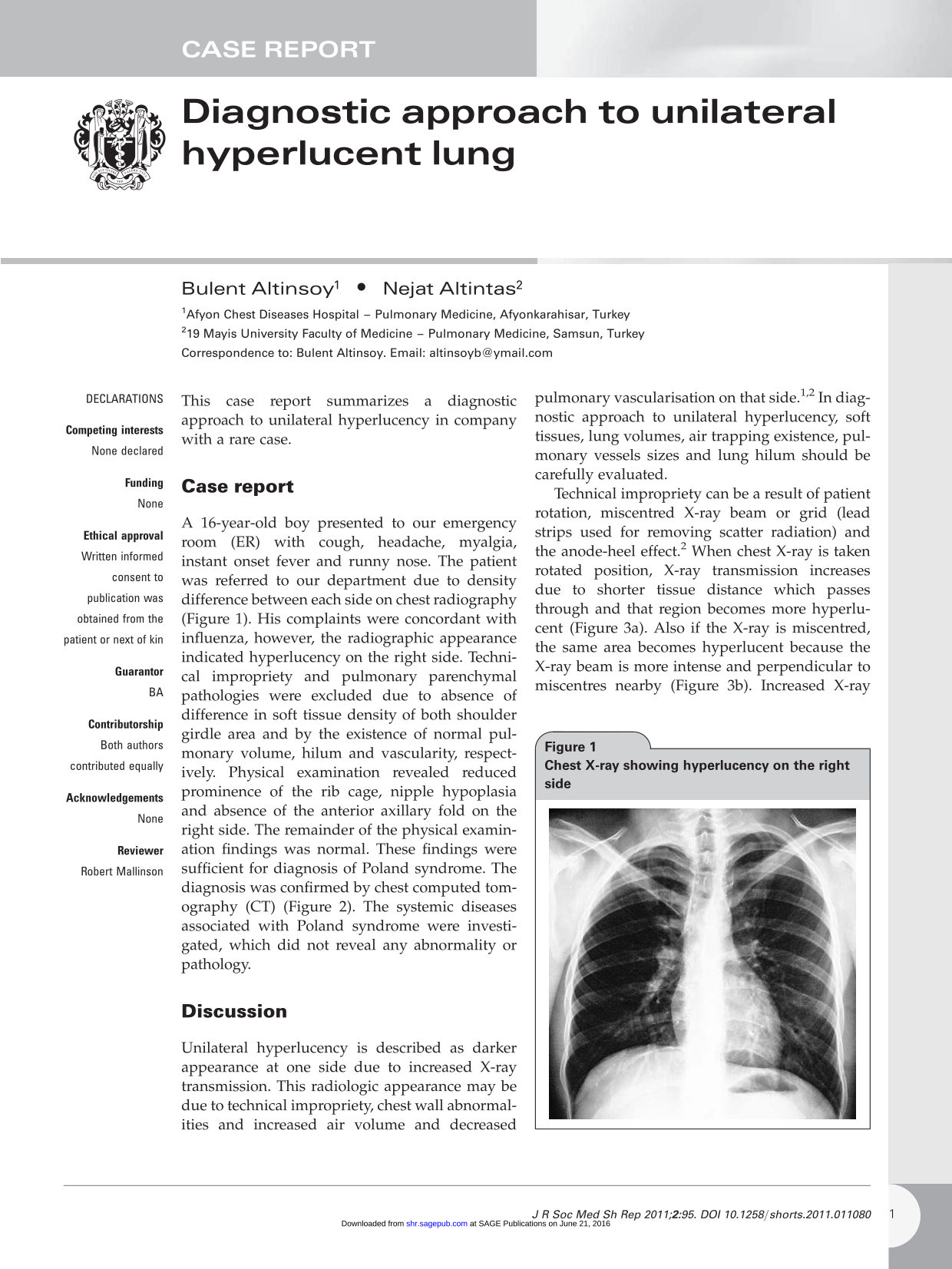
A 16-year-old boy presented to our emergency room (ER) with cough, headache, myalgia, instant onset fever and runny nose. The patient was referred to our department due to density difference between each side on chest radiography (Figure 1). His complaints were concordant with influenza, however, the radiographic appearance indicated hyperlucency on the right side. Technical impropriety and pulmonary parenchymal pathologies were excluded due to absence of difference in soft tissue density of both shoulder girdle area and by the existence of normal pulmonary volume, hilum and vascularity, respectively. Physical examination revealed reduced prominence of the rib cage, nipple hypoplasia and absence of the anterior axillary fold on the right side. The remainder of the physical examination findings was normal. These findings were sufficient for diagnosis of Poland syndrome. The diagnosis was confirmed by chest computed tomography (CT) (Figure 2). The systemic diseases associated with Poland syndrome were investigated, which did not reveal any abnormality or pathology.

Chest X-ray showing hyperlucency on the right side

CT scan of thorax showing agenesis of pectoral muscle in right hemithorax
Discussion
Unilateral hyperlucency is described as darker appearance at one side due to increased X-ray transmission. This radiologic appearance may be due to technical impropriety, chest wall abnormalities and increased air volume and decreased pulmonary vascularisation on that side.1,2 In diagnostic approach to unilateral hyperlucency, soft tissues, lung volumes, air trapping existence, pulmonary vessels sizes and lung hilum should be carefully evaluated.
Technical impropriety can be a result of patient rotation, miscentred X-ray beam or grid (lead strips used for removing scatter radiation) and the anode-heel effect. 2 When chest X-ray is taken rotated position, X-ray transmission increases due to shorter tissue distance which passes through and that region becomes more hyperlucent (Figure 3a). Also if the X-ray is miscentred, the same area becomes hyperlucent because the X-ray beam is more intense and perpendicular to miscentres nearby (Figure 3b). Increased X-ray absorption as a result of electrons arriving more parallel to the lower end of the anode target rather than upper end of the anode target results in decreased X-ray intensity in the direction of the anode than the cathode. This situation is defined as anode-heel effect (Figure 3c). In order to avoid this effect, while the cathode side is facing the patient's shoulders, the anode side is facing the abdomen. 3 To dicreminate unilateral hyperlucency relevant technical impropriety, position of mediastinum and the relative exposure of soft tissues in the affected side (especially around the shoulder girdles) should be checked out. 2

a. Rotated position; b. Miscentred X-ray beam; c. The anode-heel effect
Radiologic Features of some Causes of Hyperluceny

OHI = Obstructive hyperinflation, CHI = Compensatory hyperinflation, CVC = Congenital vascular causes, AVC = Acquired vascular causes
However, there are some exceptions concerning this scheme. For example, lung volume increase may not be prominent in such conditions if there is a compression atelectasis in adjacent lobe secondary to obstructive hyperinflation in one lobe or atelectasis in adjacent lobe secondary to compensatory hyperinflation in one lobe. 1 Furthermore, lung volumes stay small although there is an air trapping in dimunitive pulmonary vascu-larisation secondary to post-viral bronchiolitis during early childhood so called Swyer-James syndrome. 1
Poland syndrome is a rare congenital anomaly characterized by hypoplasia of the breast and nipple, scarcity of subcutaneous tissue, absence of the costosternal portion of the pectoralis major muscle, lack of the pectoralis minor muscle, aplasia or deformity of the costal cartilages or ribs, alopecia of the axillary and mammary region, and unilateral brachysyndactyly The extent and involvement of these components are variable. 4 In mild forms (especially non-associated with hand deformity) diagnosis can be overlooked. 5 These patient are generally diagnosed during radiologic screening test accidentally or when patients applied to a doctor for cosmetic purposes. It was shown that this malformation is associated with metabolic disorders, malignancies and organ anomalies.4,5 Thereof, this disease is not only important radiologically but also an important clinical entity.
In conclusion, unilateral hiperluceny is an important radiological finding in terms of diagnosis.