
Abstract

Pubic rami fractures are common; if pain and lack of mobility are disproportionate further investigations should be considered.
DECLARATIONS
None declared
None
Written consent to publication has been obtained from the patient or next of kin
AG
Both authors contributed equally
Ian Wallace
Case report
A 65-year-old woman was admitted acutely via the Accident & Emergency Department (A&E) with severe pelvic pain. Plain radiographs performed on admission revealed right-sided pubic rami fractures and discontinuity of the sacral alae suspicious of sacral fractures (Figure 1.) On questioning she gave a history of sudden onset pelvic pain with no prior history of trauma. She was a smoker, had previously consumed excessive amounts of alcohol as well as not following a particularly well-balanced diet. Since being widowed she had suffered an anxiety disorder which had prevented her from leaving the residential home she lived in. Following her menopause at the age of 47 years she had commenced hormone replacement therapy (HRT) which was discontinued 4 years later. Routine bloods taken on admission were all normal including the initial C-reactive protein (CRP). Subsequent additional blood tests revealed normal vitamin D, parathyroid hormone and thyroid function.
Plain radiograph of pelvis. There is an obvious fracture of the right inferior pubic ramus and more subtle discontinuity of the sacral alae bilaterally
Due to the severity of symptoms, the patient experienced pain disproportionate to that expected with a simple pubic rami fracture and lack of mobility despite analgesia and physiotherapy; an isotope bone scan was performed. Increased uptake was noted in the right pubic bone and both sacral alae consistent with both pelvic and sacral insufficiency fractures. A further area of increased uptake was identified in the lower thoracic spine representing a vertebral crush fracture (Figure 2), which was confirmed with plain radiographs of the thoracic spine. Initial management was with analgesia and subcutaneous injections of calcitonin. These were later changed to two infusions of pamidronate and subsequently alendronate with calcium and vitamin D supplementation. Following a 2-week period of titrating analgesia and intensive physiotherapy, our patient was mobile with a Zimmer frame.
The classic Honda sign (H-shaped tracer uptake) is demonstrated on bone scintigraphy over the sacrum. This confirms the presence of bilateral sacral insufficiency type fractures. Increased tracer uptake is also observed at the site of right pubic ramis fracture and in the lower thoracic vertebrae which when correlated with a plain radiograph of the thoracic spine revealed a vertebral crush fracture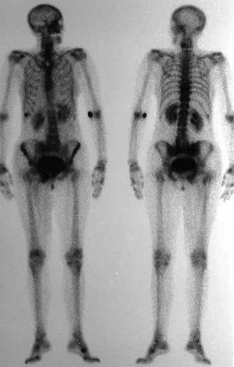
Unfortunately days later she began to complain of a supra pubic mass and associated discomfort. Examination revealed a 5 × 5 cm fluctuant swelling to the right side of her vulva. Ultrasound imaging performed the same day supported the surgical opinion that this was likely to be a haematoma and it was therefore managed conservatively. Forty-eight hours later the vulval lesion began to discharge subcentimeter bone fragments (Figure 3) mixed with yellow pus that cultured Staphalococcus Aureus. Bilateral sacral insufficiency fractures (Figure 4) and osteomyelitis of the pubic rami fractures was diagnosed and confirmed by CT imaging the following day. Fragments of bone were visible extending into the vulva.
Subcentimeter bone fragment discharged from the vulval abscess
CT pelvis, with bone windows clearly demonstrates the bilateral sacral insufficiency fractures
The patient was managed conservatively on a medical ward with input from surgical, gynaecology, microbiology and orthopaedic consultants. A prolonged course of intravenous flucloxacillin and fusidic acid was commenced. CRP and white cell count monitoring showed a slow decline and the patient's pain began to settle. Following two weeks of treatment with intravenous antibiotics she began to experience further severe pain around her sacrum. On rolling the patient to exam her pelvis was felt to move out of alignment. Minutes later venous bleeding was noted from the site of the unhealed vulval abscess. Urgent imaging and orthopaedic opinion was sought confirming a pelvic diastasis. Later that evening, she had an external fixation device fitted in theatre. Following application of this device her pain settled instantaneously as did the bleeding. For the remainder of her hospital stay she was treated with continuing antibiotics at the recommendation of the microbiologist. The external fixation device remained in situ for four weeks. Following its removal she underwent an intense period of physiotherapy and 12 weeks following initial admission was discharged to a nursing home mobile with a Zimmer frame and assistance from one nurse. Six months later she remains clinically stable.
Discussion
This patient was very unfortunate to develop infection following pelvic insufficiency fractures. We can only assume this occurred because of a bacteraemia, with no obvious source of infection other than cannula sites. Osteomyelitis on the background of multiple insufficiency fractures, osteoporosis and subsequent pelvic diastasis rendered this woman's management a major challenge. She was extremely fortunate to survive the above events and be discharged mobile to a nursing home. A case report exists of insufficiency fractures following pelvic abscess and sepsis in a patient with rheumatoid arthritis treated with high dose steroid. 1 However there are no reported cases of infection following pelvic insufficiency fractures nor any presenting with vulval abscess and bone fragment extrusion.
In general medicine, the discovery of a pubic ramus fracture in A&E or medical assessment ward would not usually generate concern. Patients may be discharged with analgesia and instructions to ‘mobilize’. When osteoporosis is present, the initial fracture heralds instability of the pelvic ring and further fracture may exist or follow. The ‘Honda’ sign is when bilateral sacral alae fractures occur and appear as an ‘H’ on isotope bone imaging. These fractures may be present without obvious signs or symptoms and are frequently not identified on plain radiographs.
One clinical concern when managing insufficiency fractures is with the use of bisphosphonates. Although our initial use of calcitonin is not evidence-based, there are anecdotal reports of calcitonin alleviating pain as well as stimulating both bone formation and healing. By suppressing osteoclast activity, bisphosphonates rapidly reduce bone turnover, suggesting caution when fracture healing is required. There remains a delicate balance here between preventing further fractures occurring while at the same time allowing the existing fractures to heal properly. We would still suggest calcitonin initially where pain is a major issue followed by bisphosphonates either orally or intravenously.
The incidence of insufficiency fracture is estimated to be in the range of 1–5% depending on referral population. 2 The first report of spontaneous fractures of the sacrum were made by Lourie in 1982. 3 The main site of insufficiency fractures tends to be the pelvic ring although they can occur in all bones of the lower limb. As previously stated the major risk factor for these types of fractures is osteoporosis. Other important factors include previous radiotherapy to the affected area, previous corticosteroid therapy and rheumatoid arthritis. 4
Lower limb insufficiency fractures are well documented to be associated with considerable pain and loss of independence. Insufficiency fractures of the proximal femur are associated with loss of mobility and independence in 25–75% of those formerly self-sufficient. 5 Pelvic fractures are frequently considered benign, although a study by Taillander et al. showed only one-third of patients to have the same level of self-sufficiency post fracture. In their study 25% patients were discharged to institutions, 6 as with our case.
The history of severe lower back pain, worsening on standing leads the clinician to suspect a fracture and therefore request a plain radiograph. Insufficiency fractures by definition occur spontaneously or after trivial trauma. Due to the intense amount of pain suffered by our patient and the initial radiograph, an isotope bone scan was requested early in her admission. This demonstrated the classic Honda sign, pathognomic of sacral insufficiency fractures.7,8 CT scanning is helpful in diagnosing sacral insufficiency fractures and confirmed these along with extensive soft tissue infection around the site of the pubic rami fractures. If the diagnosis is uncertain or there is clinical concern regarding fracture healing, follow-up CT imaging after several months is recommended. 9 Some authors advocate MRI imaging as investigation of choice as it can help identify early medullary oedema as well as the fracture line. 10
The aims of treating established osteoporosis is to alleviate symptoms and reduce the risk of further fractures in the future. Analgesia and bed rest usually result in improvement in pain. 11 Gradual mobilization versus early mobilization has been debated over the years in the literature with no clear consensus. One case report, like ours, describes an external fixation device being applied to obtain rapid pain relief and early mobilization. 12 External fixation reduces and stabilizes the anterior ring of the pelvis but does not prevent disruptions of the vertical or posterior ring.
General advice on diet including calcium, vitamin D and protein intake; taking regular weight-bearing exercise, smoking cessation and decreasing alcohol consumption is standard for osteoporosis. Calcium and vitamin D supplementation has been shown to decrease the risk of both non-vertebral and hip fractures in elderly women living in nursing homes.13,14
More recently two publications have disputed this when they failed to demonstrate the benefit of such dietary supplementation over placebo in primary or secondary prevention of osteoporotic fractures in women over the age of 70 years. 15
Bisphosphonates are widely used to treat osteoporosis in older women. They are adsorbed by the hydroxyapatite crystals present in bone, slowing the rate of bone turnover. This group of drugs are anecdotally used to reduce pain and prevent further spinal fractures. Many trials have shown that they significantly reduce vertebral, nonvertebral and hip fractures in postmenopausal women. 16 Evidence produced by Clarita et al. however suggests that alendronate therapy may produce severe suppression of bone turnover, hence resulting in susceptibility to delayed healing of non-spinal fractures. 17 Calcitonin and pamidronate have also been used for pain relief in osteoporotic fractures.
Newer drugs available for treatment of osteoporosis include both strontium and parathyroid injections. At the time this patient was admitted and treated these were not available.
Summary
Our patient presented to A&E and was diagnosed with pelvic insufficiency fractures. Imaging demonstrated pubic rami and sacral insufficiency fractures, which were treated with analgesia, early mobilization, calcitonin and pamidronate. Subsequently she developed vulval swelling which later discharged bone fragments from an infected insufficiency fracture. As the admission progressed she required orthopaedic intervention and an external fixator device to be positioned to stabilize her pelvis. Despite all of the above, she made a slow but steady recovery and was discharged to a nursing home mobile with a Zimmer frame plus assistance from one person.
After an extensive literature review we have found no other documented case of infection and abscess formation following insufficiency fractures of the pelvis. We present an unusual, complex case and highlight the management difficulties we encountered throughout this patient's hospital admission.
Footnotes
Acknowledgements
None