
Abstract
Pigs are frequently anaesthetized in animal research settings. Due to the unique laryngeal anatomy, endotracheal intubation is demanding in pigs. Several complications associated with endotracheal intubation have been reported in pigs, but laryngeal perforation following difficult intubation has not been documented so far. The present case report describes laryngeal perforation in a three-month-old pig following difficult intubation.
Pigs, like other mammals, are prone to respiratory depression under general anaesthesia. Furthermore they are prone to suffer from partial airway obstruction due to the species-specific reduced functional residual capacity of the lungs and the presence of excess tissue in the oropharyngeal region. This increases the likelihood of perianaesthetic hypoxia. 1 Intubation of the trachea maintains a patent airway during general anaesthesia, protects the airways from aspiration and helps to provide intermittent positive pressure ventilation (IPPV). 2 It has been shown that mortality rate decreases if pigs are intubated for surgical procedures. 3 However, due to their unique laryngeal anatomy, endotracheal intubation in pigs can be challenging and can have complications. 4–7
A three-month-old female hybrid pig, weighing 20 kg, was anaesthetized for a laparotomy for a surgical trainee course. This terminal procedure was approved by the institutional ethics committee and the national authority according to § 8ff of the Law for Animal Experiments, Tierversuchsgesetz (TVG) (BMWF-68.205/0028-II/3b/2011). Prior to anaesthesia the pig was fasted for 12 h and had free access to water. Clinical examination revealed no abnormalities.
The pig was premedicated with tiletamine/zolazepam (Zoletil 100®, Virbac, Carros, France) 2.5 mg/kg intramuscularly. The sedated pig was placed in sternal recumbency and preoxygenated for 5 min. Thiopental was administered intravenously to effect until optimal conditions for orotracheal intubation were achieved. Prior to intubation lidocaine spray (Xylocain®, Astra Zeneca, Vienna, Austria) was applied on the rima glottis. Intubation was performed under laryngoscopic control by two experienced anaesthetists.
An attempt to intubate the trachea with a 6 mm internal diameter (ID) polyvinylchloride (PVC) endotracheal tube (ETT) in a smooth clockwise rotatory movement was aborted because too much resistance was encountered at the level of the arytenoid cartilages. During a new attempt now with a 4.5 mm ID ETT laryngospasm allowed the tip of the ETT only to be advanced a few millimetres past the arytenoid cartilages. A PVC covered intubation stylet with a diameter of 2 mm was introduced alongside the ETT into the trachea. This stylet was used as a guide for the intratracheal introduction of a second 4.5 mm ID ETT while the first tube was simultaneously removed. The cuff of the ETT was inflated. The pig was now positioned in lateral recumbency, connected to a circle breathing system and treated with IPPV using 100% oxygen. Oxygen saturation, ECG and capnography were unremarkable. At the moment the pig was disconnected from the anaesthetic system to facilitate transition to dorsal recumbency which was required for surgery, the ETT moved 2–4 cm backwards. The cuff was deflated, the ETT gently advanced and following cuff inflation reconnected to the breathing system. From this moment on capnographic waveforms and chest movements were absent but cyclic enlargement of the perilaryngeal region was observed which was confirmed to be subcutaneous emphysema after palpation. The ETT was pulled back with deflated cuff and after several attempts to intubate under laryngoscopic control failed, the decision to euthanize the pig was made (intravenous T61®, Intervet, Unterschleissheim, Germany) allowing continuation of surgical training on the cadaver.
However subsequent dissection of the laryngeal area showed that the tube had perforated the larynx between the thyroid cartilage and the proximal part of the trachea (cricothyroid ligament) and was located subcutaneously (Figure 1). This finding is compatible with the clinical signs (no chest movement, cyclic subcutaneous emphysema) and the absence of capnographic waveforms. It is not possible to determine post hoc during which phase of the intubation process the cricothyroid ligament was damaged and perforated.
Ventral view to the caudal part of the larynx and the trachea showing perforation by the tip of the endotracheal tube (ETT)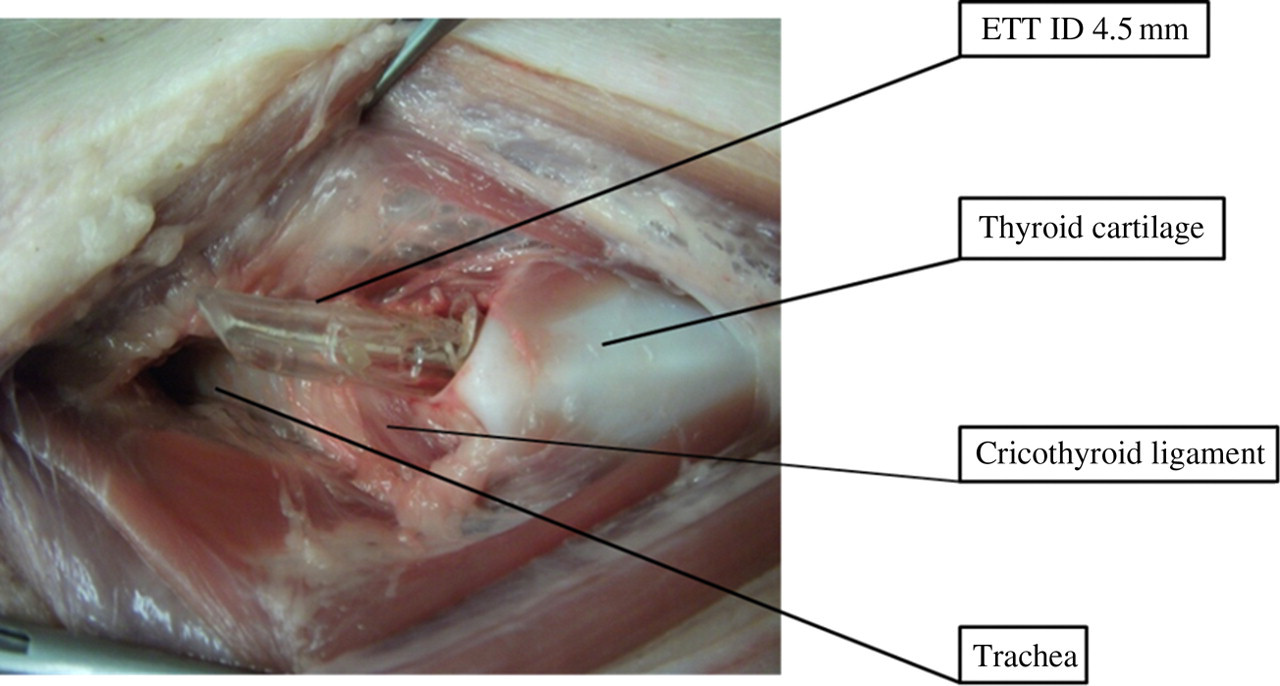
To the best of the authors’ knowledge perforation of the larynx during intubation attempts of pigs has not been reported. Tracheal intubation in pigs is described as being more difficult compared with other animals (e.g. cats and dogs). 8–11 The porcine mouth cannot be opened widely and the distance from planum rostrale to the larynx is long. As a consequence, visualization of the rima glottis is limited. The larynx is loosely attached, of small size and kinks ventrally which creates a sharp angle preventing straightforward insertion of the endotracheal tube. Furthermore, a pharyngeal diverticulum and blind sacs formed by the large ventral and two lateral ventricles make intubation more difficult. The diameter of the larynx and trachea is small in pigs compared with other animals of similar body weight; therefore, smaller endotracheal tubes are needed.
The pig was intubated in ventral recumbency. Both dorsal and ventral recumbency are described for endotracheal intubation. Ventral recumbency enables a smooth and fast intubation and reduces risk of airway obstruction provided overextension of the head is avoided. 12–15 Overextension will kink the airway between the larynx and trachea. Different techniques for endotracheal intubation are described in pigs which emphasize the necessity to visualize the rima glottis using an appropriate laryngoscope. 16 Techniques include the use of curved and straight tubes with and without rotational movements of the ETT. When a stylet is used, the ETT can be advanced over the stylet into the trachea without the need of rotation. The stylet should be inserted carefully into the trachea to avoid damaging mucosal membranes. 15 Difficulties and the impossibility to intubate pigs are reported in the literature. 17,18
Laryngospasm impedes tracheal intubation in pigs especially when the plane of anaesthesia is too light. 3,5,12,19–21 In our case endotracheal intubation was attempted twice in the presence of laryngospasm while executing rotary movements with the ETTs. These attempts were unsuccessful but it is possible that the cricothyroid ligament was perforated during these efforts. Using the over-the-wire technique allowed easy tracheal introduction of a tube, but the passage of its tip through the cricothyroid ligament laceration and the subsequent perilaryngeal position of the tip remained unnoticed during the process of reinsertion. The amount of pressure exerted during the intubation attempts cannot be quantified here. However, both anaesthetists were experienced on a daily basis with intubation of various species including pigs and were performing the intubation of the pig with great care avoiding excessive pressure application.
The endotracheal tubes used were curved and made of PVC. Endotracheal tubes made of PVC exert up to 10 times higher forces and pressures on distal objects when compared with silicon or armoured tubes. 22 It is possible that the choice of a straight type ETT made of softer material would have prevented laryngeal perforation in this case.
This case shows that perforation of the larynx caused by the ETT can occur in pigs during a standard intubation procedure. Therefore, all preventative measures must be taken in order to perform a successful and smooth intubation at first attempt. Straight tubes made of soft material may be advantageous in diminishing the risk of laryngeal trauma.