
Abstract
In vivo research with animal models has been a preferred experimental system in bone-related biomedical research since, by approximation, it allows relevant data gathering regarding physiological and pathological conditions that could be of use to establish more effective clinical interventions. Animal models, and more specifically rodent models, have been extensively used and have contributed greatly to the development and establishment of a wide range of translational approaches aiming to regenerate the bone tissue. In this regard, the calvarial defect model has found great application in basic and applied research, nonetheless the controversial rationalization for the use of critical size defects – defects that are unable to report spontaneous healing – or subcritical size defects in the proposed applications. Accordingly, this work aims to review the advantages and limitations of the use of rodent models in biomedical bone-related research, emphasizing the problematic issues of the use of calvarial critical and subcritical size defects. Additionally, surgical protocols for the establishment of both defects in rat calvarial bone, as well as the description and exemplification of the most frequently used techniques to access the bone tissue repair, are portrayed.
Keywords
Bone tissue is characterized by an adequate capacity to regenerate itself following the establishment of a lesion or a defect, when the physiological stimuli converge to establish a proper response. Nevertheless, determined conditions associated with an unfavourable microenvironment, suboptimal surgical techniques or biomechanical instability can lead to a poor prognosis on bone tissue regeneration. 1 Furthermore, large orthopaedic defects, in which the physiological regenerative capabilities are exceeded, rely on the application of mechanically- and biologically-suited biomaterials, including ceramics, metals, polymers and composites, for adequate tissue reconstruction. 2 The reported situations are established major clinical and socioeconomic burdens with serious implications in patients lifestyle and life quality. 3 Furthermore, several systemic conditions are known to affect bone physiological equilibrium and may contribute to the impairment of an adequate healing process. 4–6
Regenerative medicine and tissue engineering approaches to the bone tissue enclose a wide range of applications that aim to repair, augment, substitute and regenerate lost tissues. 2 De novo bone formation relies on the recruitment, transplantation, homing or modulation of progenitor or differentiated cells. These cells require the availability of an adequate substrate to play their biological function by adhering, proliferating and differentiating in a controlled way, giving rise to a mature tissue with adequate biomechanical properties. 2,3
The design of experimental models to evaluate the efficacy and biosafety of these regenerative strategies – which encompass cells, materials and modulators – requires both methodical control and modulation of specific variables – situations that cannot be met in a single model. According to Muschler et al., 7 in order to achieve the clinical translation of bone tissue engineering strategies, used models should meet several criteria: mimic the clinical and biological environment in which the experimental methodology will be assessed; allow quantifiable parameters to access the success, in a quantitative and qualitative way, and functional performance of the regenerated tissue; and identify and foresee relevant differences in the biological performance between assayed methods.
In vitro assays give great contribution to the comprehension of fundamental biological mechanisms (i.e. transcription, translation, intracellular signalling events, regulation of the cell cycle, ligand–receptor interactions, etc.), screening of the biological activity, toxicity and immunogenicity of specific compounds, and evaluation of the direct or indirect cell response to a seeded material. 8,9 Additionally, in vitro models of higher complexity have been developed, enclosing the use of bioreactors to access the biological response of three-dimensional (3D) constructs and co-culture models with different cell populations, to further recreate the complexity of multiple cell interactions. 10,11 Even so, in vitro assays reveal significant limitations in their capacity to recreate the intricacies of the in vivo milieu, and are incapable of predicting clinical output and performance.
In vivo research with animal models has been a preferred experimental system since, by approximation, it provides relevant data regarding physiological and pathological conditions that could be of use to establish more effective clinical interventions. In vivo research establishes a link between in vitro studies and clinical trials. Experimental animal models are essential to provide an adequate approximation to the real settings. Accordingly, the selection of the appropriate design and model relies, in the very end, in the therapeutic modality that is being tested. 7 In this context, and in relation to the bone tissue, one may consider five domains of biological activity: (1) osteogenesis – associated with the cellular function – i.e. the biological process by which committed cells at different stages of differentiation are recruited, activated, and proliferate and differentiate in order to produce de novo bone tissue; (2) osteoconduction – associated with the support function – i.e. the process by which a specific volume of tissue is preserved from the infringement of neighbouring tissues and allows osteogenic cells to play their biological role; (3) osteoinduction – associated with the modulator function – i.e. the process by which soluble or matrix-associated molecules influence the biological fate of osteoblastic cells; (4) mass transfer; and (5) biophysical effects – processes that are mainly associated with biochemical and biomechanical events that contribute to the establishment of an adequate tissue healing. 12
Animal models, and more specifically rodent models, have been extensively used and have contributed greatly to the development and establishment of a wide range of approaches to regenerate the bone tissue. For instance, and focusing on osteogenesis, rodent models have provided great amount of data regarding the cellular behaviour of multiple populations relevant to bone regeneration. 13–15 Moreover, and in regard to osteoconduction, rat and mouse models have also proven to be of great importance regarding the assessment of the biocompatibility of granular, scaffolds or bulk materials, in the evaluation of the surface osteoconduction and specific toxicity, and degradation rate of synthetic materials used for bone repair. 7,15,16 These models have also been used for the evaluation of the biosafety profile of the osteoinduction process, following the administration of biomodulators. 15,17,18
Among the available orthotopic models used for evaluating bone function, calvarial bone defects have gained a widespread reputation and use in the published literature, reporting valuable data from basic and applied research. Nonetheless, a major point of debate relies on the selection of either critical size defects (CSDs) – the ones that do not report spontaneous healing during the lifetime of the animal – or subcritical size defects – defects in which complete bone regeneration is expected, without the contribution of induced-recruited or added factors.
In this way, we aim to review the advantages and limitations of the use of rodent models in biomedical bone-related research, in particular the calvarial bone model, emphasizing the problematic issues of the use of critical size and subcritical size bone defects. Additionally, surgical protocols for the establishment of both defects in rat calvarial bone, as well as the description and exemplification of the most frequently used techniques to access the bone tissue repair, are portrayed.
Selection of animal species – the relevance of rodents
A large variety of mammalian species have been used in bone-related research. O'Loughlin et al. 19 reviewed the use of animal models in fracture repair studies published for the past 10 years in six orthopaedic journals and realized the following relative order of frequency: rat 38%, rabbit 19%, mouse 13%, sheep 11%, dog 9%, goat 4% and other 4%. This report clearly states the relevance of rodents in orthopaedic research. Fundamental research, feasibility and bioactivity testing greatly rely on the use of mice and rats due to the high definition of the models in a biological, genetic and immunological point of view, which allows the attainment of a high level of experimental reproducibility.
In fundamental research, the availability of biological tools (e.g. primers for polymerase chain reaction testing, microarrays, probes, antibodies, etc.), the fast turnover of individuals and the rapid occurrence of biological processes are of the utmost importance, allowing for a facilitated observation of the processes under study. In an additional way, the sequencing of mouse 20 and rat 21 genome smoothed the progress of transgenic and knockout models which contributed to the knowledge of the function and modulation of specific genes. 22,23
Going one step further, fundamental research, feasibility and bioactive testing direct the research process along the translational application pathway. Specific evaluation broadly includes the efficacy of materials' or agents' delivery, cytotoxicity and biocompatibility testing and screening for adverse or unwanted reactions. The same models used in feasibility studies, with relevance for both mice and rats, are also utilized for the quality control screening and bioactivity of products or implants. In addition, route of administration and assessment of the target tissues may be evaluated in compliance with the proposed clinical setting.
The assessment of clinical modelling and efficacy, also referred as preclinical testing, is broadly performed in large skeletally mature animals including dogs, goats, sheep and pigs, reporting phylogenetical resemblance. Structure and composition of these animals' bone tissue have been found to be highly similar to those of humans. 24 Point variations are generally associated with modest differences in cancellous and cortical density, response to oophorectomy and diet restriction, extent of sexual dismorphism, age of peak bone mass, and rate and extension of Haversian remodelling. 7,24,25 Despite the stated variations, there is no substantiation that one model proves to be a better match than any other to address clinical translation of assayed therapeutic approaches. As a result, individual selection should rely on economic issues, local access, housing requirements and availability, staff expertise, and considerations of the experimental protocol. Non-human primates (NHPs) have also been used in the study of bone repair, despite the established increase in the research cost and the issue of cultural and ethical questions. Arguments substantiated by the evolutionary proximity and anatomic and physiological resemblance converge to indicate NHPs as first choice models in bone-related research. Nevertheless, the diversity and variability attained in effector responses limit the efficacy of clinical translation – response variations between primate species have been shown to be greater than in quadrupeds and even humans. 26,27 In addition, biomechanical differences have been largely stated and reports concerning differential biological responses – e.g. baboons seem to be hypersensitive to the administration of bone morphogenic proteins 28 – contribute to the fact that NHPs do not attain a valid consensus as providing a first choice model, compared to other large animals. 7
As stated, a wide range of animal models is available not only for fundamental, feasibility and bioactivity bone-related biomedical research, but also for preclinical testing. Individual choice should be made according to the knowledge of established biological differences, advantages and inconveniences, but also taking into account methodological and operational features of each model. Comparing the characteristics of the bone tissue between the described animals, several differences can be outputted. For instance, rodents continue to model their skeleton throughout their life cycle – regarding growth and reshaping – and growth plates remain open throughout adulthood. Mice and rats also report limited trabecular bone content and Haversain remodelling – by tunnelling osteoclasts – does not occur, although cancellous remodelling is established. 29,30 Furthermore, rodent models are not suited to the establishment of long-term studies, in which multiple biopsies or large blood samples are required, due to biological constraints. On the other hand, compared to large animal models, rodents are inexpensive, easy to house and manipulate, and report minimal social concern. Furthermore, if data that can be validated and that are trustworthy can be acquired, animals placed at the lower end of the phylogenetic scale should be preferably used – in this case, rodents are a first choice option over large mammals. Due to their widespread utilization, much is known regarding the biological processes associated with bone turnover, diet modifications and drug administration. Furthermore, the reduced lifespan of these animals allows for the study of the influence of ageing in the bone metabolism and regeneration processes.
Overviewing the stated arguments, rodent models prove to be quite useful in bone-related research, being among first choice models for in vivo testing of regenerative and/or therapeutic approaches to the bone tissue.
In vivo models of bone regeneration – the calvarial defect model
Currently, several in vivo models are used to evaluate the bone regeneration process, the bone–biomaterial interaction and the physiological or pathological evidence of the modulation of the ossification pathway. Experimental models can be classified as heterotopic or orthotopic, based on the vicinity to the autologous bone tissue. The characterization of materials used for bone regeneration is generally assayed, on a first approach, in a heterotopic model, i.e. subcutaneous, intramuscular, intraperitoneal or mesentery location, which are generally used prior to the assessment of the materials' behaviour in direct contact with the bone tissue. Moreover, if the material reveals a paste-like consistency, it can be easily injected into the targeted site.
The surgical implantation of granular, scaffolds or bulk materials has been widely conducted in rodents. Accordingly, the rat heterotopic model has been used successfully to show the sequence of events involved in the ossification process. 31 Most common implantation sites include the subcutaneous tissue on the back or upper abdominal area. 32 Although the use of heterotopic bioassays in rodent models prevails in the biocompatibility assessment of materials, there is a scarcity of data regarding translational and clinical applications, no matter how quantitative the data from the heterotopic bioassay may be. 33
In order to solve inherited limitations from heterotopic applications, intraosseous defects have been used to test for the capacity of materials and constructs to promote the repair of discontinuous and weight-bearing lesions. The selection of orthotopic models in bone research relies broadly on one of the following options: calvarial, long bone or mandible segmental, partial cortical and cancellous bone defects. 34 The calvarial model stands out as an adequate model for evaluating complex materials and tissue engineering constructs aiming bone regeneration, especially which refers to the regeneration of craniofacial defects. This model has been established in a wide range of animal species, including mice, rats, rabbits, dogs, sheep, goats, pigs and NHPs, although rats and rabbits are the most commonly used animals.
The calvarial model is very adequate and popular among researchers, mainly due to the following reasons: the calvarial bone structure allows the establishment of a uniform, reproducible and standardized defect that is easily evaluated by radiographic and histological analysis; the anatomic location reflects an adequate size for surgical access and intraoperative handling; the dura and the overlaying skin set up an adequate support for implanted materials, without the need for internal or external fixation; and the model has been widely used and studied, allowing a precise comparison of grafted substances. 32 Nonetheless, it does not allow the assessment of the biological response of the implanted material to a physiological biomechanical loading which may be a limitation in some applications. In this case, alternative anatomical load-bearing locations, like the mandible, the femur or tibia, should be preferably selected.
Calvarial critical size and subcritical size defect models
The use of the calvarial model implies the selection of the defect size, particularly the knowledge of the critical size of the defect, which varies according to the animal species, strain, gender, age, anatomic site, shape, size and micromechanical environment. 35–37 According to Schmitz et al. the CSD can be described as the smallest wound established intraosseously in a particular bone, which does not report spontaneous healing during the lifetime of the animal. 35,36 Accordingly, the CSD can be considered the prototype of discontinuity defects, as a specific condition of failed osteogenesis for overcoming the threshold of the physiological process of tissue repair/regeneration.
Despite the stated knowledge, the processes associated with the completion of bone healing during the repair of CSD have not been fully understood. Honma et al. 38 compared the regeneration process in subcritical (3.8 mm in diameter) and critical (8.8 mm in diameter) size defects established in Wistar rats' calvaria. New bone formation was observed in both defect sizes, with small defects being almost completely filled by 24 weeks, while large defects remained unrepaired, becoming non-unions with fibrous connective tissue in the areas in which the bone formation was absent. Radiographic analysis reported that the bone formed per week was maximal at week 4, for both defect sizes, data supported by a high expression of collagen type I and osteocalcin, by osteoblasts and osteocytes, as assessed by in situ hybridization. Moreover, collagen and osteocalcin production was very low at week 24 – for both defect sizes – suggesting that bone cells may greatly reduce bone formation and the differentiation process of new osteoblasts may be severally impaired at this time point. In this way, the authors suggested that the bone formation process ceases within 24 weeks, regardless of the dimension of the defect size and completion of defect repair. 38 The influence of the postsurgical inflammatory response on the osteogenic activity may be important to substantiate the attained data, and has been reported in several in vitro and in vivo models. 39–42
All the same, the evaluation of the CSD relies not only on the assessment of the repair of the wound size but, above all, on the quality of the regenerated tissue. This evaluation should be based on the relativity of the model, i.e. according to the specificities of the experimental protocol and time points, since the best tissue quality ought to be achieved in the shortest lapse of time. Regarding tissue quality on bone regeneration, it is widely established that fibrous connective tissue regenerates faster than bone, relying on the faster migration of fibroblasts to the wound site, compared with osteoblasts. 43–46 Early works, in the 1970s, by Najjar and Kahn 47 showed that the first healing of bone wounds in animal models was set on fibrovascular connective tissue, followed by immature bone replacement, which was in turn remodelled into mature bone. Accordingly, one ought to attain a fast osseous healing which can prevent the establishment of undesirable results such as fibrous non-union or fibrous encapsulation of implanted materials. 48,49
Furthermore, apart from the size of the defect, other factors determine the quantity and quality of the new bone tissue formed. For instance, the anatomical site and its stability are relevant since the load stress and the degree of mobility can have a profound effect on the final outcome. 50,51 Other factors, proven to be relevant, include the intrinsic structure of the bone tissue, adequacy of vascular supply, involvement of the cortical bone, and presence or absence of the periosteum. 35,36,46,52 Animals' age is also an important point to consider in experimental planning since juvenile animals have been shown to report an increased healing capacity of calvarial defects, which may be related to differential transcriptional gene expression profiles. 53–56 Wu et al., in order to determine the CSD in neonatal mice, established circular defects of 0.8, 1.0 and 1.5 mm in diameter in the parietal bone. Healing assessment reported statistically significant differences in bone filling percentages: 1.5 mm defects (4.49%), 1.0 mm defects (47.65%) and 0.8 mm defects (73.45%). 57 These results show the 0.8 and 1.0 mm defects as subcritical size defects and the 1.5 mm defects as a CSD. In another experimental setting, Aalami et al. aimed to compare the bone regeneration process in juvenile and adult mice. Non-suture-associated cranial defects, with 3, 4 and 5 mm in diameter, established in the calvarial bone of juvenile (6-day-old) and adult (60-day-old) mice, were evaluated. Following eight weeks of healing, histological and radiographic evaluation concluded that all three defect sizes were found to be critical in the adult, whereas significant healing (59%, 65% and 44%, respectively, of the total defect area) was seen in juvenile mice. 53
In rats, controversial data regarding the dimensions of CSD have been reported. Turnbull et al. 58 described the surgical establishment of a 2 mm in diameter defect in Wistar rats' calvaria, and their incapacity to heal up to three months, as assessed by radiographic and histological techniques. Following, Mulliken et al. 59 reported a 4 mm CSD in Charles River rats. Takagi et al. 60 characterized the CSD as 8 mm in diameter, in 6-month-old Sprague Dawley rats, as it has been reported earlier by Ray and Holloway 61 for Long Evans rats. Later on, Hollinger et al. substantiated the 8 mm defect as the CSD for Long Evans and Walter Reed rats, reporting the inability of the defect to heal spontaneously, following 13 months, and a maximum of 10% of de novo bone formation. 35,36
Other bibliographic reports have acknowledged the 5 mm defect as a CSD for adult rats. Bosch et al. 62 reported that a 5 mm defect, apart from minor bone formation on the defects' margins, was unable to heal spontaneously up to 12 months after the surgery. The stated advantages of the use of a 5 mm CSD include the possibility to establish two defects per animal, and the avoidance of the inclusion of the sagittal suture in the defect, minimizing the risk of midsagittal sinus lesion. 62 On the other hand, laterally performed craniotomies – opposing those which include the sagittal suture, like in the 8 mm defect – may allow substance diffusion and impair local repair/regeneration due to the close vicinity of adjacent defects, which may blight the relevance of the model. 63 Accordingly, the 8 mm defect continues to be used in many reports which aim to assess different bone therapeutic strategies. This is established not only for the described limitations of the 5 mm CSD design but also due to the increased challenge associated with the higher diameter of the defect.
Apart from the need to establish a CSD, with an increased challenge for the regenerative process, subcritical size calvarial defects allow the evaluation of the impact that a wide range of conditions, biological processes or added substances have on the physiological equilibrium of the bone tissue regeneration, through an intramembranous ossification process. Specifically, subcritical size calvarial defects have been generally used to evaluate the biological response of the bone regeneration process following the establishment of pathological conditions, 64,65 within the evaluation of therapeutic options to enhance bone regeneration 66,67 and optimization of hard tissues-related surgical techniques. 68,69 In mice, 1 mm diameter defects have been routinely used as subcritical size defects due to the fast healing – normally completed around 14 days – allowing the determination of stimulatory or inhibitory effects of locally or systemically applied substances. In rats, defects created with 3 mm trephines, or less, have found generalized application as standardized subcritical size defects.
These surgical procedures, due to the technique-dependent and sensitive applied protocol, as well as the significance of the anatomical neighbouring structures, should be conducted by clinical professionals with surgical expertise, following an adequate training period. Additionally, due to the expected amount of pain induced by the orthopaedic procedure, a local anaesthetic should be used in conjunction with a general anaesthetic as well as an appropriate regimen of postoperative analgesia.
In the following, we describe a refined surgical protocol for the establishment of CSD and subcritical size defects in Wistar rats' calvarial bone, for the evaluation of the biocompatibility of a ceramic granular material.
Establishment of calvarial critical size and subcritical size defects on rodents
The animals, 3-month-old male Wistar rats, weighing between 260 and 280 g, were purchased from Charles River Laboratories. National regulations for the care and use of laboratory animals were observed at all times. All experiments were approved by the local Institutional Animal Care and Use Committee. Animals were housed in plastic cages in a monitored environment (21°C; 12 h light/dark cycle).
Anaesthesia and pain control followed recommended routines for the species. Prior to the surgical intervention, the animals were anaesthetized using sevoflurane inhalation anaesthesia (4–5% induction; 2–3% maintenance). Then, the skin that covered the skull, around the incision area, was shaved and disinfected with iodopovidone solution. An intraperitoneal injection of tramadol (10 mg/kg) for postoperative analgesia was given, and the animals were then transferred onto a heating pad, maintained at 37°C, in the operating field. A subcutaneous injection of 0.3–0.4 mL of 1% lidocaine, used as a local anaesthetic, was administered along the sagittal midline of the skull. A surgical blade was then used to perform a midline incision, from the nasofrontal area to an anterior location of the external occipital protuberance (Figure 1a). The skin was then reflected bilaterally and a new midline incision, of around 3 cm, allowed the division of the subcutaneous fascia and the bilateral reflection of the periosteal flaps following blunt dissection, to expose the calvarial bone surface (Figures 1b–d). Careful drilling with an 8 mm diameter trephine bur, mounted on a low-speed dental handpiece, was done around the sagittal suture, and a standardized, round, segmental defect was made. During drilling, the area was continuously irrigated with sterile saline solution and extreme care was taken not to damage the dura mater or the underlying blood vessels and sinus (Figures 1e and f). The obtained calvarial disk was carefully removed to avoid tearing of the subjacent cranial structures (Figure 1g). After thoroughly rinsing of the defect with physiological saline, to wash out any bone fragments, the material in the granular form – a modified hydroxyapatite – was implanted within the defect (Figures 1h and i). The periosteum and scalp were closed over in layers with interrupted 4-0 Vicryl resorbable sutures (Figures 1j and k). Following surgical intervention, the animals were given a subcutaneous injection of sterile saline (10 mL/kg/h of surgery). The rats were placed in soft-bedded plastic cages and housed individually after the procedure. Each animal received a subcutaneous injection of tramadol (10 mg/kg) at 12, 24 and 36 h after surgery for continued postoperative analgesia. Animals were given free access to food and water and were monitored daily, in the postoperative period until euthanasia, for any complications or abnormal behaviour.
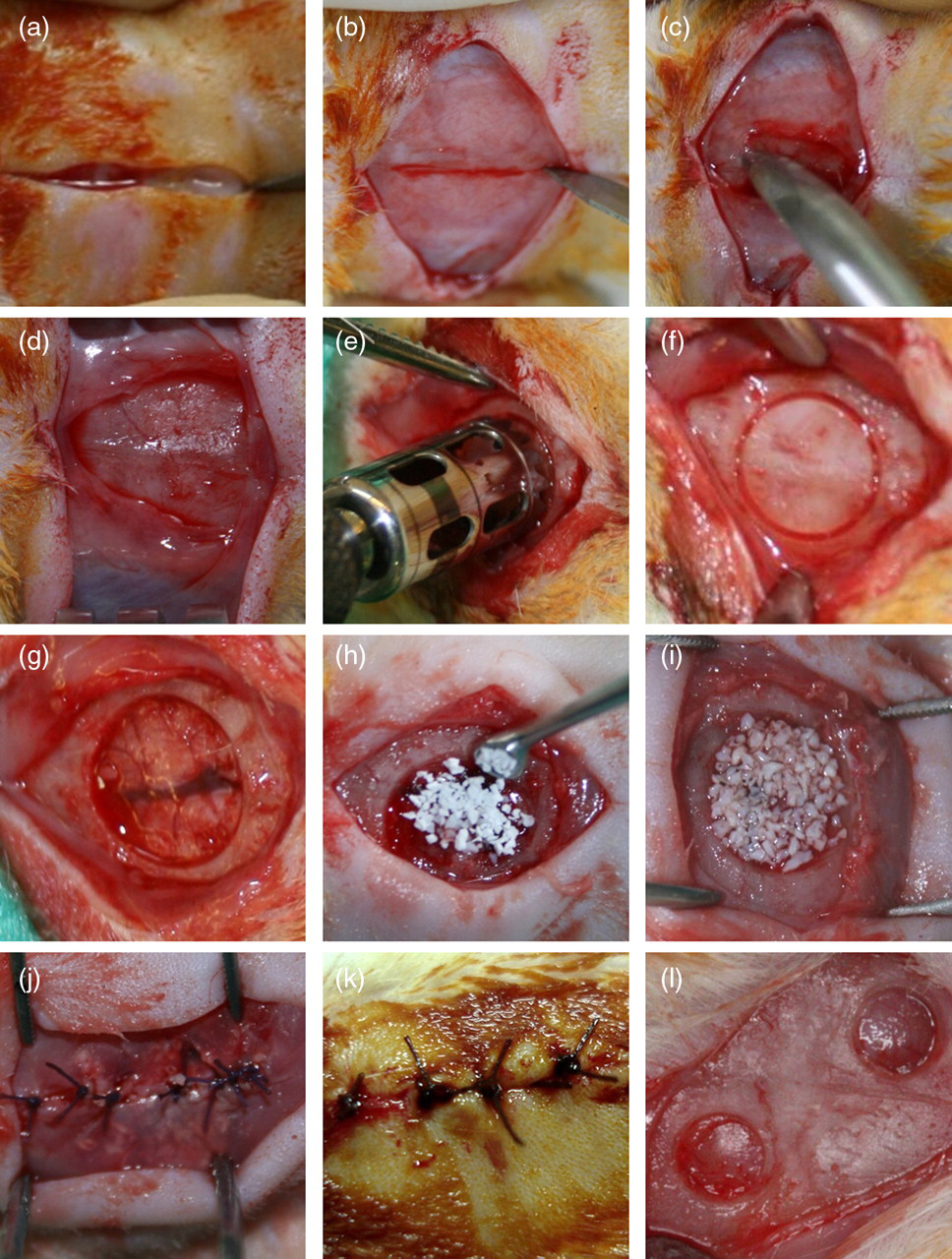
Surgical protocol for the establishment of critical size defects (a–k) and subcritical size defects (l) on rat calvarial bone
Alternatively, the establishment of subcritical calvarial defects, in rats, can be carried out with the use of 3 mm trephines or less in diameter, allowing the establishment of multiple defects in the calvarial bone (Figure 1l).
Evaluation methodologies of the bone regeneration process
The assessment of the bone regeneration process can be carried out by multiple and complementary methodologies. Histological analysis, electron microscopy and radiological techniques are among the most commonly used. Below, the authors described the most relevant techniques used with given examples from their personal experience.
Histological evaluation
Characterization of the regenerated bone tissue is commonly performed by histological evaluation with light microscopy, following standard staining of the sample. Descriptive histology and histomorphometry are the two major classes of histological evaluation. Descriptive histology is used to provide a general assessment of the tissue of interest, giving data regarding cell morphology, structure and arrangement within the interface with the extracellular matrix or with an implanted material. Semiquantitative analysis could be performed using a score system, in which the data can be evaluated using non-parametric analysis of variance. Histomorphometry allows quantitative analysis of histological data, namely regarding length and distance, area and number of the components of interest. 29,70 These are the basic parameters that can be assessed in 2D histomorphometric analysis. 3D evaluation can be conducted from 2D sampled images following specific considered assumptions. Due to the use of multiple designations and misinterpretations in histomorphometric analysis, a consensus report aimed to establish a system for standardization of nomenclature, symbols and units, has generally been adopted. 71 Despite the aim to perform a reproducible analysis in the evaluation of the attained results, histological observation is lined by significant inter-method and inter-observer variability, especially with regard to histomorphometric analysis. 72
Bone tissue can also be labelled in vivo with intravital markers, in order to assess the quantitative evaluation of bone formation and remodelling events. 73 Used fluorochromes are irreversibly deposited and rely on their calcium-binding properties to be embedded into the mineralization fronts of the remodelling bone. 73 Prepared samples can be visualized under fluorescent light. Specific binding to newly mineralizing surfaces of mineralized tissues may be due to the smaller size of the apatite crystals formed during the early stages of the mineralization process, compared with older mineralizing sites. 74,75 The most commonly used fluorochromes are tetracycline, calcein dyes, alizarins and xylenol. 76
Immunohistochemistry (IHC), by a direct or indirect technique, could also be used to identify and specifically localize peptides or proteins of interest in bone tissue section, based on the principle of the specific interaction between antibodies and antigens. 77 In order to improve reproducibility and standardization of the data attained with IHC, quantitative methodologies have been developed, relying upon pixel-counting and cumulative signal strength algorithms. 78,79
As an example, in Figure 2, representative images of some of the depicted techniques are shown.
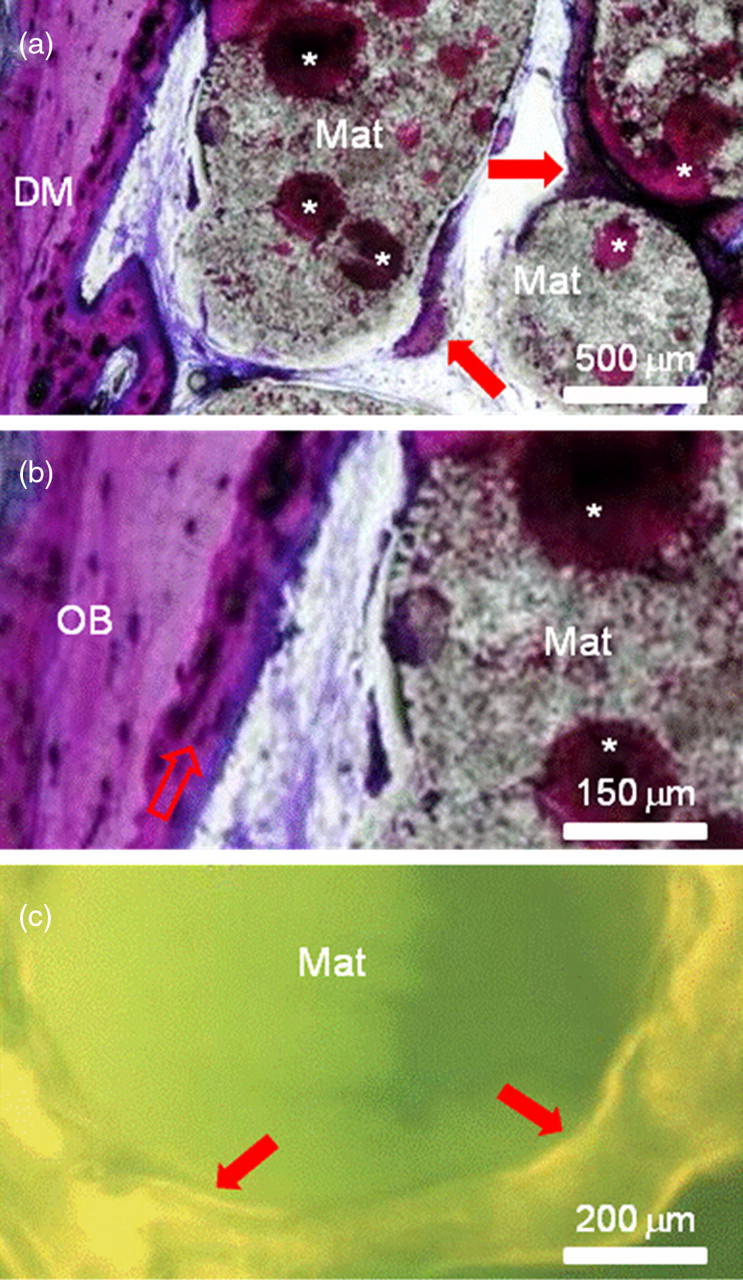
Images of non-decalcified resin-embedded calvarial samples, following the surgical establishment of an 8 mm critical size defect on rat calvarial bone and the implantation of a ceramic material. (a, b) Figures are stained with toluidine blue, 15 days following implantation. (c) A tetracycline-stained sample is shown, three months following material implantation. Mat: pellets of the implanted material; DM: defect margin; arrows: areas of new bone formation; OB: old bone; *areas of primary ossification
Electron microscopy
Scanning electron microscopy (SEM) is also an important tool used in the evaluation of the structure and morphology of the bone tissue. In biomedical bone-related research, it has been used to characterize trabecular and cortical bone surfaces, implant surfaces, wear debris, implant beds and implant–tissue interfaces. 80–82 With the use of corrosion-cast tissues, SEM has been able to assess the vascular structure in the evaluated tissues – which is of the utmost importance for the development and maintenance of an adequate bone tissue quality. 83,84 Major limitations associated with SEM application are related to the relative small size of the evaluated samples and the need for drying the specimen for observation, which has been shown to induce modifications in morphology and spatial structure of the tissues. 85 New technologies have allowed the development of low-temperature or cryo-SEM, and environmental SEM systems, which aim to solve the dehydration-related problems. 80
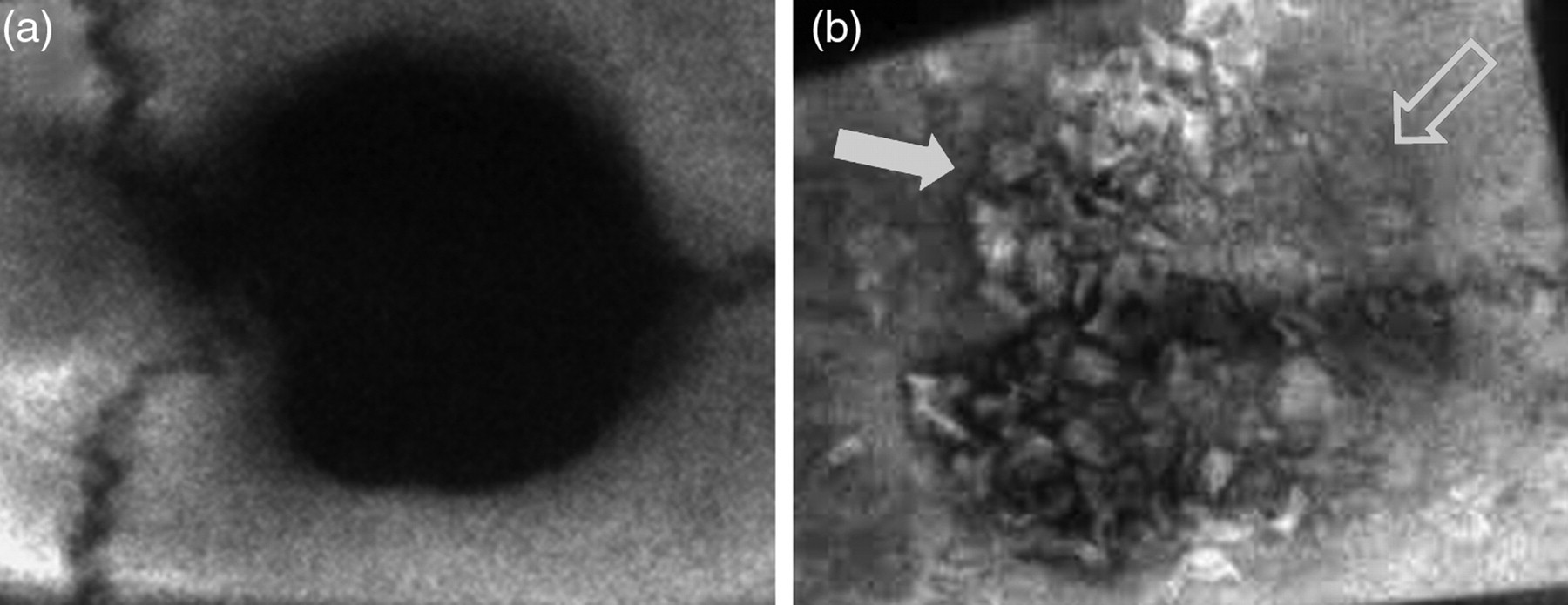
As an example images of rat calvaria specimens assessed by environmental SEM are portrayed in Figure 3.
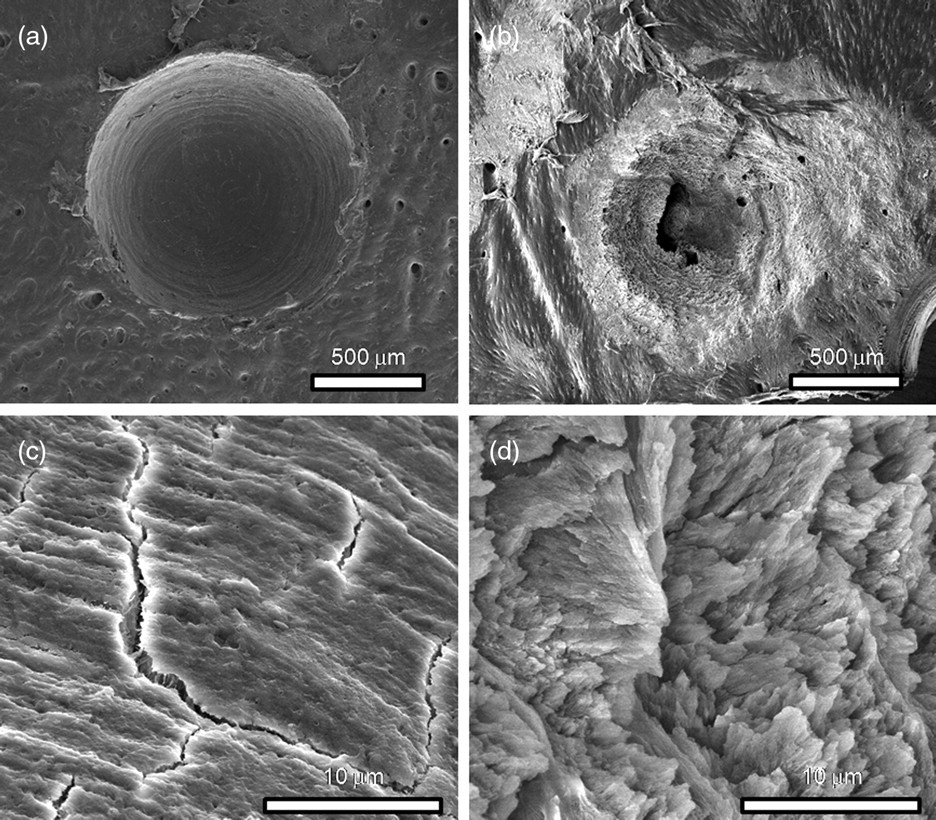
Micrographs of rat calvaria assessed by environmental scanning electron microscopy, three days following the establishment of subcritical monocortical defects, are presented. The defects were established with a 1 mm diameter burr (a and c) and with a high-intensity Erb:YAG laser (b and d). (c, d) Detailed high magnification images of (a, b), respectively
Electron microscopy techniques also make use of transmission methodologies – transmission electron microscopy (TEM) – in which a beam of electrons is transmitted through an ultrathin specimen, interacting with the specimen as it passes through. This is a very powerful methodology to evaluate the ultrastructure and morphology of subcellular components, cells and tissue–biomaterial interaction. 86–88 Despite the very high resolution, samples require extensive sample preparation and the field of view is relatively small, raising the possibility that the analysed region may not be characteristic of the whole sample. Additionally, samples may suffer modifications from the preparation process or directly damaged by the electron beam. 87,88
Illustrating this application, two images of ceramic-based materials' debris interacting with rat calvarial osteoblastic cells are shown in Figure 4.
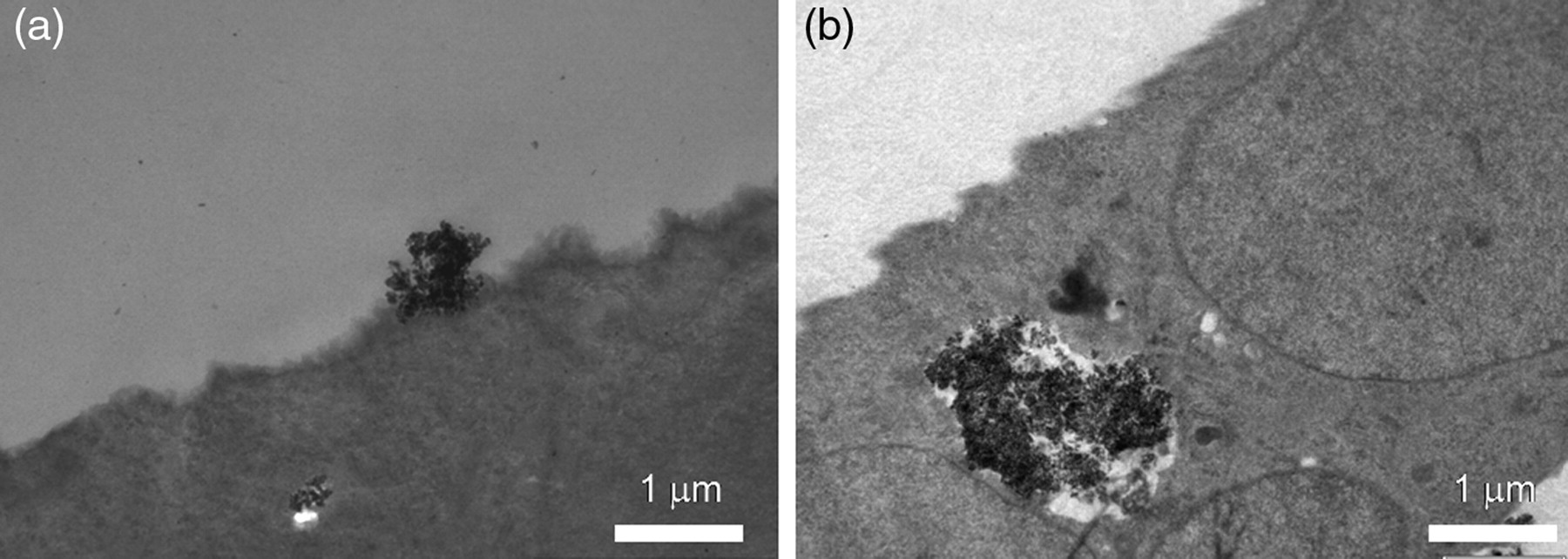
Transmission electron micrographs of ceramic-derived material debris interacting with osteoblastic cells from rat calvarial bone
Radiological techniques
Radiological techniques have also been employed with success in the evaluation of the bone repair and regeneration processes. Radiography is the basic method for the evaluation of fracture healing and bone-defect repair. In clinical or experimental settings, presurgical evaluation allows the assessment of the specific anatomy and bone dimensions, facilitating the selection of fixation devices and implants. Postoperative evaluation also benefits from the radiographic assessment, allowing the determination of the fracture placement or the quality of the defect fill. Periodic evaluation permits the monitoring of the repair process. High-resolution radiography and microradiography are complementary techniques that allow the evaluation of the detailed structure of the bone tissue. Quantification of bone aposition and densitometric analysis can be conducted, even near an implant. 89
Sample radiographic images of the rat calvarial bone, with or without a grafted material, are shown in Figure 5.
Radiographic images of the rat calvarial bone without (a) or with (b) a grafted ceramic material, six months following the surgical establishment of an 8 mm critical size defect. Areas of newly formed bone following material resorption (open arrow) can be identified, simultaneously with areas of implanted biomaterial content, interspersed with the newly formed bone tissue (full arrow)
X-ray computed microtomography (μCT) is a miniaturized form of conventional computerized axial tomography that has been found to be a valuable application in bone-related research. This technology enables 3D reconstruction of the internal structure of small X-ray opaque objects in a non-invasive and non-destructive way. μCT allows the qualitative and quantitative assessment of the spatial and temporal mineralization of bone formation. The availability of 3D analysis techniques, coupled to specific image processing methods, opens up new possibilities for the analysis of bone structures 90,91 Recent reports outline the use of μCT for the monitorization of the in vivo bone remodelling process. 92
In Figure 6, μCT-reconstructed 3D images of rat calvarial bone are shown.
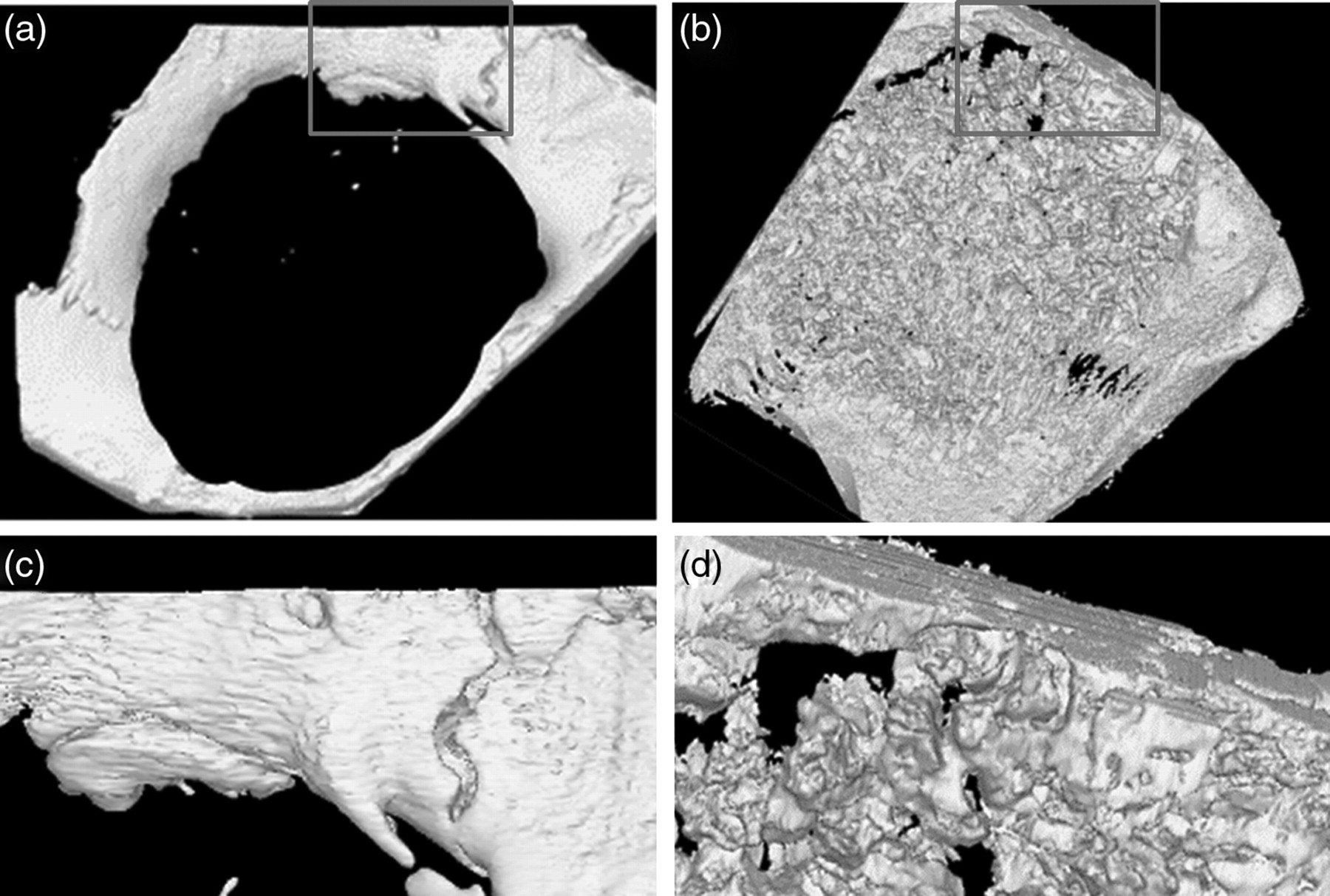
X-ray computed microtomography reconstructed three-dimensional images of rat calvarial bone, three months following the establishment of an 8 mm critical size defect, without (a, c) and with the implantation of a ceramic material (b, d). (c, d) Detailed high magnification images of (a, b), respectively
Conclusion
Animal models play an important role in bone tissue-related research by providing methodological approaches to study detailed events and regenerative advances, which aim to establish adequate translational applications with clinical relevance. While no species fulfils the requirements of an ideal animal model, rodents are by far the best choice because they are easily available, easy to house and handle, and account for a huge amount of background data due to their widespread use in the reported literature. Furthermore, the described models established on rodents calvarial bone allow the establishment of a standardized, reproducible orthotopic defect, which permits not only the evaluation of the biocompatibility of implanted biomaterials or tissue engineering constructs but also the assessment of the intramembranous ossification process in physiological and pathological conditions. Multiple methodologies, including histological analysis, electron microscopy and radiological techniques, have reported relevant and complementary data, with proven adequacy, in the assessment of bone repair/regeneration process.
Footnotes
Acknowledgements
Financial support received from Project ‘ERA-MNT/0002/2009’ (‘A new generation of biodegradable implants obtained from magnesium alloys functionalized by means of advanced surface treatments’) and Faculty of Dental Medicine, University of Porto.