Articular cartilage repair is still a challenge in orthopaedic surgery. Although many treatment options have been developed in the last decade, true regeneration of hyaline articular cartilage is yet to be accomplished. In vitro experiments are useful for evaluating cell–matrix interactions under controlled parameters. When introducing new treatment options into clinical routine, adequate animal models are capable of closing the gap between in vitro experiments and the clinical use in human beings. We developed an animal model in the Göttingen minipig (GMP) to evaluate the healing of osteochondral or full-thickness cartilage defects. The defects were located in the middle third of the medial portion of the patellofemoral joint at both distal femurs. Chondral defects were 6.3 mm, osteochondral defects either 5.4 or 6.3 mm in diameter and 8 or 10 mm deep. In both defects the endogenous repair response showed incomplete repair tissue formation up to 12 months postoperatively. Based on its limited capability for endogenous repair of chondral and osteochondral defects, the GMP is a useful model for critical assessment of new treatment strategies in articular cartilage tissue engineering.
Hyaline articular cartilage plays a crucial role in mammalian joint function. Based on its distinct histoanatomical structure it allows nearly frictionless movement between articulating bones while reducing peak stress forces during joint load at the same time. Hyaline articular cartilage is avascular and has no neuronal or lymphatic supply. As a result, its endogenous healing potential is limited and any structural damage, even if penetration of the subchondral bone plate occurs, at best is repaired with fibrous or fibrocartilaginous repair tissue (Mankin 1982). True restoration with repair tissue mimicking hyaline cartilage was never observed in humans or in other mammalian species.
Although new cell-based therapy strategies are established in clinical routine, e.g. autologous chondrocyte transplantation (ACT) (Brittberg et al. 1994), autologous osteochondral transplantation (Bobic 1999, Hangody & Fules 2003) and microfracturing (Steadman et al. 2001), each of these techniques still has its own limitations and prospective randomized clinical trials did not show a significant difference in the clinical outcome when compared with each other (Knutsen et al. 2004). As a result, there is a strong interest in new treatment options. Lately, cell-based technologies and methods from tissue engineering have become more and more popular and some investigators have already shown a beneficial potential to overcome the endogenous limitations of articular cartilage defect repair (Solchaga et al. 2001, Hunziker 2002). In vitro experiments allow evaluating the interaction and effect of various cell culture conditions while developing a new implant under controlled parameters. However, mimicking the biophysiological events which occur during articular cartilage and bone healing in vivo is practically impossible. Therefore, adequate animal models are needed in order to perform a critical evaluation and assessment of the expected clinical impact of any new treatment protocol.
In experimental joint surgery, an idealized animal model would duplicate the endogenous repair process found in humans. In addition, a well standardized and reproducible defect model would facilitate a robust comparison of different treatment modalities. However, there is no species available which allows a direct translation into the biological system of humans. Therefore, the choice of the species and the defect model, the age of the animals used, individual joint dimensions, joint load and mechanics as well as the thickness of the articular cartilage are considered to be critical key factors when interpreting experimental data (Hunziker 1999).
During the past years, we have established the Göttingen minipig (GMP) in our institution as a larger animal model for experimental joint surgery. Earlier work by Hunziker and co-workers (Hunziker & Rosenberg 1996) on partial thickness articular cartilage repair in the minipig prompted the author (S Breusch) to investigate experimental osteochondral and full-thickness articular cartilage repair procedures within a similar animal model. In the course of our experimental work, we assessed the effect of novel tissue engineering-based protocols for the treatment of chondral (Gotterbarm 2003, Schneider et al. 2006) as well as osteochondral defects (Gotterbarm et al. 2003, 2006, Jung et al. 2005). This article summarizes our experience focusing on the technical feasibility and the endogenous repair response of chondral and osteochondral defect repair in the GMP. We also discuss advantages and disadvantages compared with other animal models within this context.
Materials and Methods
We retrospectively analysed a total of 46 chondral and 134 osteochondral defects which were created in the knees of 90 GMPs during various experiments (Gotterbarm 2003, Gotterbarm et al. 2003, 2006, Jung et al. 2005, Schneider et al. 2006). Sixty-two animals were male and 28 female, with a mean age of 24 months (range: 11–55) and mean weight of 38 kg (range: 20–55). All procedures were performed according to the German Animal Welfare Act dated 25 May 1998 and the experimental designs were approved by the local animal rights protection authorities (AZ 37/9185.81/48/97; AZ 35-9185.81/148/00; AZ 35-9185.81/151/00). To allow an intra-individual comparison of different treatment modalities, a bilateral setting was used with one defect per knee joint. All defects were located in the medial facet of the trochlear groove. The animals were acquired from Ellegaard Minipig, Dalmose, Denmark. The GMP originated from a crossing between the Minnesota minipig (33%), the Vietnamese potbelly swine (59%) and backcrossed with the German Landrace (8%). Skeletal maturity with closure of the growth plates occurred between 18 and 22 months. For further details, the reader is referred to the vendor's homepage (http://www.minipigs.dk).
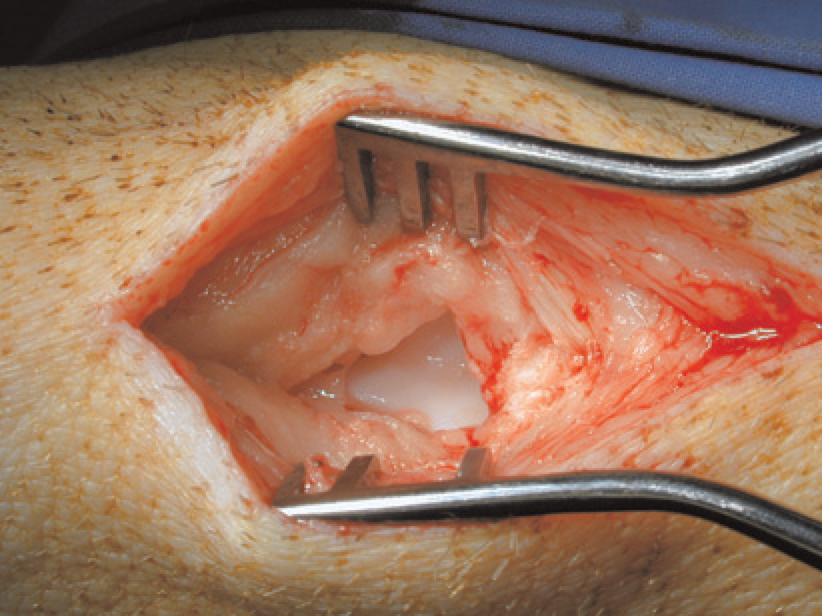
Approach Skin incision was made midline ranging from the distal patellar pole to the tibial tubercle. Splitting of the patellar tendon and inferior patellar fat pad allowed access to the patellofemoral joint (Figure 1). By flexion and extension of the knee, the whole compartment of the trochlear groove was exposed. All defects were created in the middle third of the medial portion of the patellofemoral joint. After creating the defects and treatment, all wounds were closed in layers with resorbable sutures and sealed with occlusive wound spray. Postoperatively, animals were returned to the cages and allowed immediate full weight bearing.
Transpatellar approach to the trochlear groove of the minipig stifle joint. With a midline incision and by splitting the patellar tendon and inferior patellar fat pad, the patellofermoral joint was exposed. Defects were created in the medial facet of the trochlear groove
Chondral defect
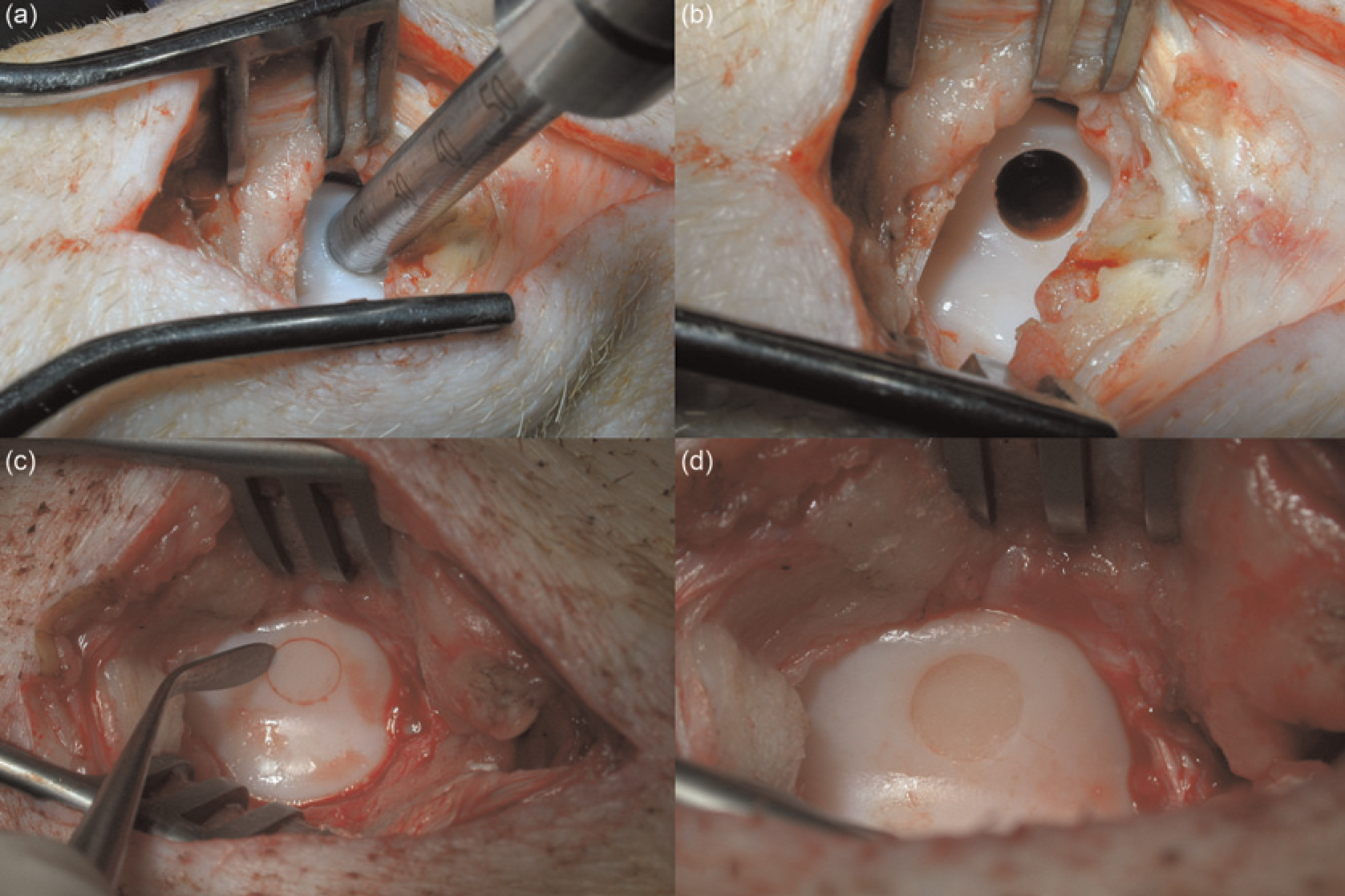
A circular full-thickness chondral defect with a diameter of 6.3 mm was created with a custom-made circular hollow cutter and a sharp, angulated raspatorium (Figure 2c). The articular cartilage was debrided meticulously down to the subchondral bone avoiding bleeding (Figure 2d). Chondral defects were either left empty or experimentally treated with autologous chondrocytes seeded into a novel collagen type I gel (Gotterbarm 2003, Schneider et al. 2006) and compared with ACT established in clinical routine (Brittberg et al. 1994).
Intraoperative pictures of defect preparation. Both defects were created in the central area of the medial facet of the trochlear groove. The osteochondral defect was prepared with a hollow diamond-coated trephine (a). This allowed highly exact defect preparation with sharp defect borders omitting any destruction of the microarchitecture of the cancellous bone (b). The chondral defect was prepared with a custom-made angulated sharp raspatorium (c). After cutting a circular defect, articular cartilage was removed by taking care not to disrupt the subchondral bone plate, i.e. avoiding bleeding (d)
Osteochondral defect
In three experiments, osteochondral defects (Figure 2b) of two different defect dimensions were created in the medial facet of the trochlear groove. A 5.4 mm in diameter and 8 mm deep defect was used to evaluate spontaneous healing compared with a cell-free biphasic collagen-TCP implant (Gotterbarm et al. 2006), whereas a larger one with 6.3 mm in diameter and 10 mm in depth was used to determine the effect of osteoperiosteal autografting with additional cell (Gotterbarm et al. 2003) or growth factor treatment (Jung et al. 2005) and compared with spontaneous healing. In both settings, the articular cartilage was at first cut perpendicular to the joint surface with a custom-made circular hollow cutter and the osteochondral defect was drilled (Figure 2a) with a diamond-coated hollow trephine (TL04 ø 6.3 mm or TL03 ø 5.4 mm, Surgical Diamond Instruments [SDI]; MedArtis AG, Deisenhofen, Germany) developed by Draenert and Draenert (1988). To prevent heat damage, the bone cutter was rinsed with sterile saline solution (NaCl 0.9%, Braun, Melsungen, Germany).
In 90 specimens, the cartilage thickness of the lateral facet of the trochlear groove was assessed prior to stress relaxation testing. The prepared distal femoral bone was therefore mounted in a custom-designed mechanical testing device (Z005/TN2S, Zwick GmbH, Ulm, Germany), and the cartilage thickness was measured according to the needle-penetration technique previously described by Hoch et al. (1983).
Histology
All specimens were cut into a 2 × 3 × 3 cm block, including the defect. The defect area was sawed into two pieces; one piece containing ~60% of the total defect area was fixed in 4% buffered formalin (pH = 7.4) for 48 h. After decalcification with 0.5 mmol/L ethylenediaminetetraacetic acid (pH = 7.4), the specimens were embedded in paraffin and serially sectioned (5 μm) in the sagittal plane including the centre of the defect and the adjacent cartilage. Alternate sections were stained with Toluidine-blue, Safranin O/fast green and immunohistochemical staining against collagen type II was performed according to routine protocols. Qualitative histomorpholgical evaluation was carried out by a blinded observer according to two different semi-quantitative scoring systems (Wakitani et al. 1989, Mainil-Varlet et al. 2001).
Statistical analysis
Simple regression analysis, one factor analysis of variance (ANOVA) and the Fisher's protected least-square difference post hoc test was performed with StatView (version 5.0.1, SAS Institute Inc, Cary, NC, USA). The level of significance was set to P < 0.05. Data are given in the text as mean values with standard deviation.
Results
All presented data were derived from earlier performed experiments (Gotterbarm 2003, Gotterbarm et al. 2003, 2006, Jung et al. 2005, Schneider et al. 2006), and retrospective data analysis was used to summarize findings and observations.
The mean thickness of healthy articular cartilage at the lateral facet of the trochlear groove in 90 knees was 518 ± 119 μm (range: 300–863 μm). One factor ANOVA testing revealed a significant difference (P = 0.004, power = 0.97) between male (563 μm) and female (475 μm) animals. Regression analysis showed a medium and small negative correlation between cartilage thickness and age (R2 = 0.318) or weight (R2 = 0.133) within all animals.
Endogenous repair response of chondral defects
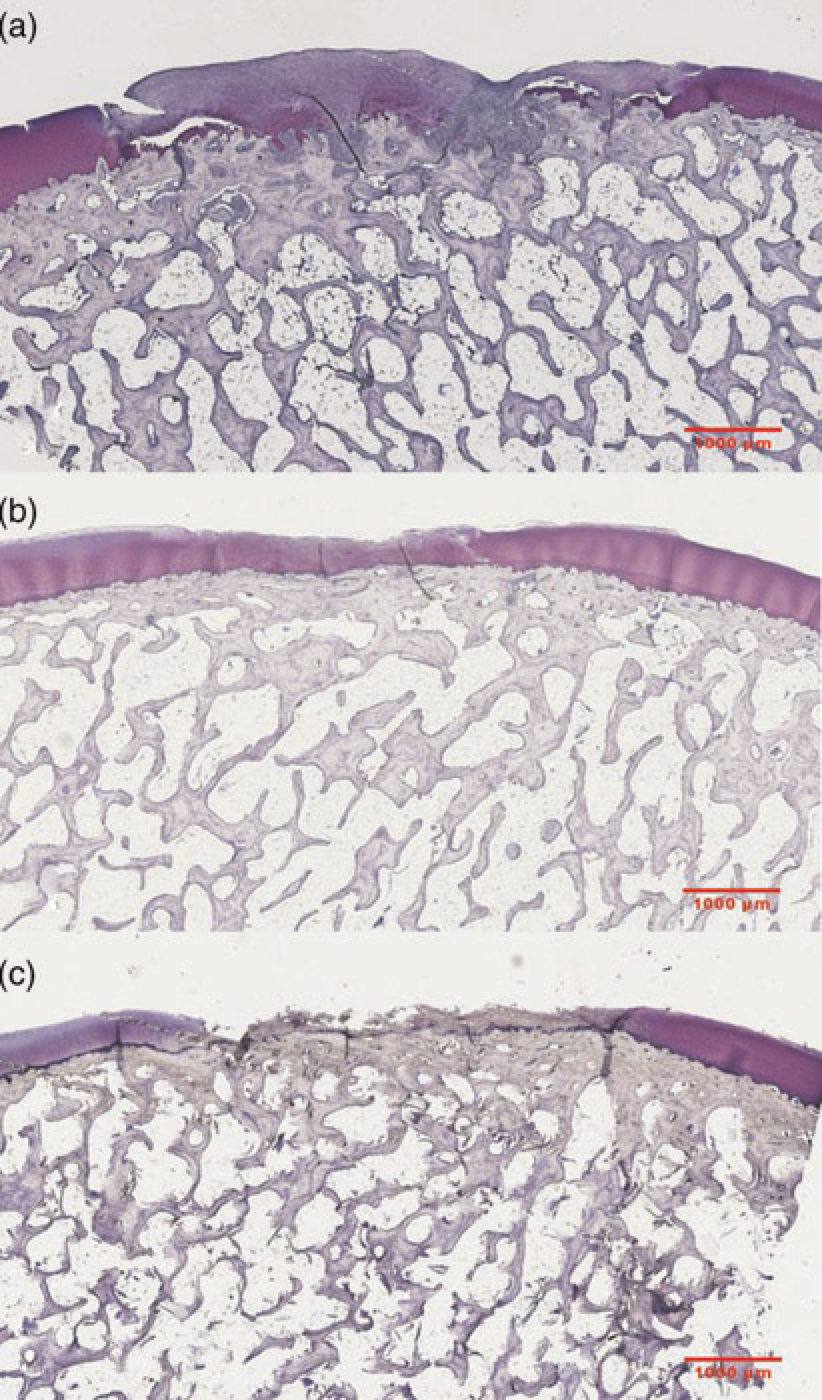
Chondral defects were followed up for 6 (n = 5), 12 (n = 3) and 52 (n = 6) weeks. Six weeks after surgery the endogenous repair response has yielded a complete filling of the defect void with mainly fibrous and partially fibrocartilaginous repair tissue (Figure 3a). The repair tissue surface was smooth and integration to the adjacent cartilage was incomplete. At 12-week follow-up, the predominant repair tissue quality was fibrocartilaginous with round, chondrocyte-like cells in lacuna embedded in a glycosaminoglycan (GAG)-rich extracellular matrix (ECM) with large disorganized collagen bundles (Figure 3b). Integration with the surrounding tissue was without cleft formation. After one year, signs of degeneration were present: defects showed a decreasing amount of filling mainly with fibrous tissue. Fibrillation of the surface and a lack of GAG-positive ECM staining became apparent (Figure 3c). According to Wakitani et al. (1989), the inversed histomorphological scoring system showed no relationship between animal age and total score values of all created defects as well as untreated chondral defects alone.
Representative photomicrographs of untreated full-thickness chondral defects in the Göttingen minipig at 6 (a), 12 (b) and 52 (c) weeks after defect creation. Of note is that good defect filling, with mainly fibrocartilage-like repair tissue occurred at 6 and 12 weeks. The intense purple metachromatic stain at 12 weeks indicates a high content of glycosaminoglycans (GAG). At 52 weeks, the repair tissue showed severe signs of degradation with a reduction of GAG-positive staining and surface disruption. (Toluidine-blue 5 μm centre-cut paraffin sections; original magnification ×10)
Endogenous repair response of osteochondral defects
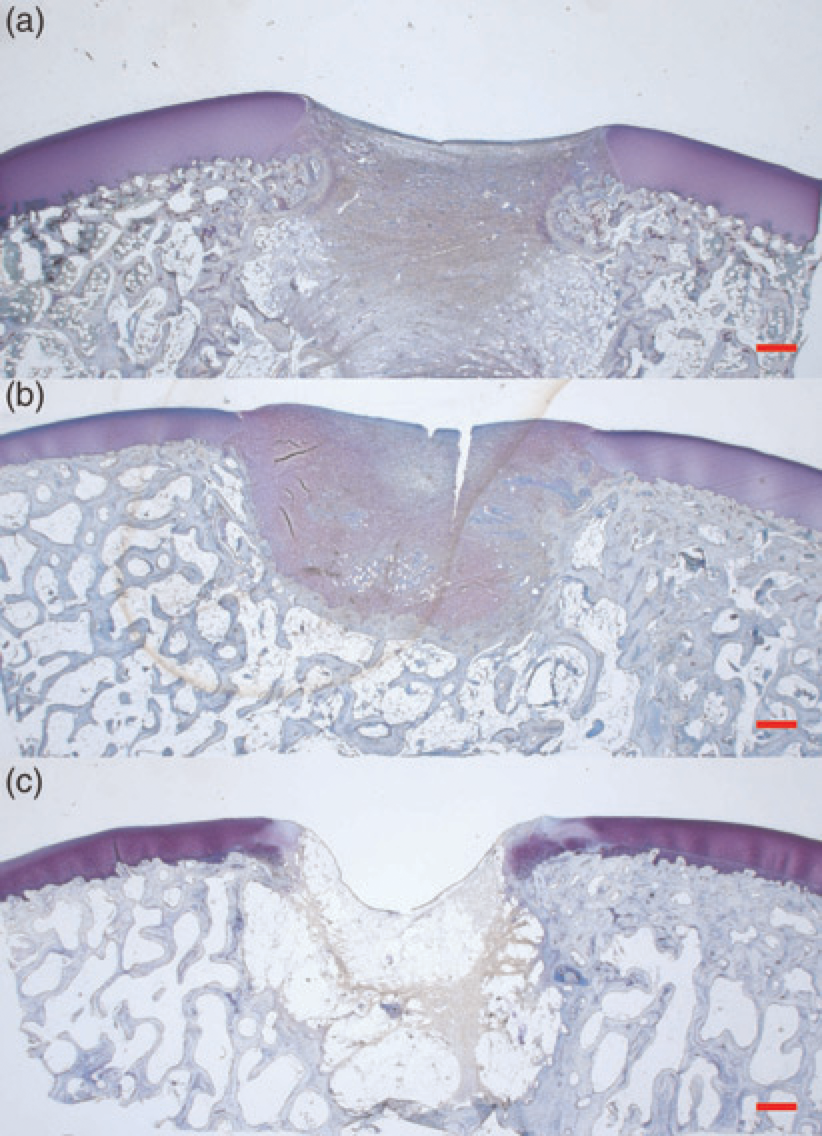
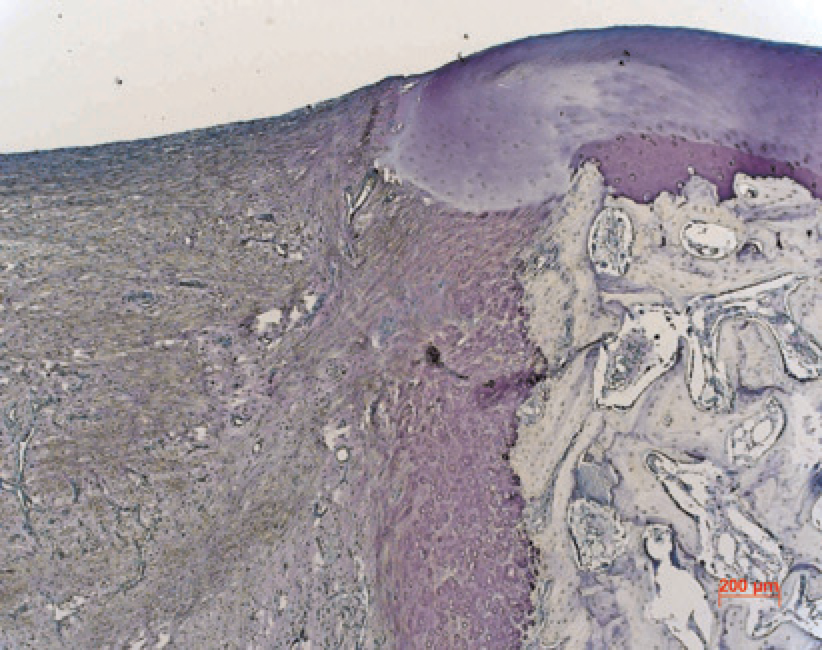
Untreated osteochondral defects of either 5.4 × 8 mm or 6.4 × 10 mm showed a similar healing pattern over time. Therefore, the following summarizes the observations made in osteochondral defects of either dimension. Defects were followed up for 6 (n = 9), 12 (n = 12) and 52 (n = 8) weeks, respectively. Throughout the evaluation they showed incomplete filling with a concavely depressed repair tissue below the level of the surrounding cartilage. From 6 to 12 weeks postoperatively (Figures 4a and b), mainly fibrous tissue with small capillary vessels and an increasing amount of fibrocartilage was present at the defect site. The repair tissue surface was smooth and integration to the adjacent bone and cartilage defect edges was complete. In some specimens, the adjacent cartilage protruded into the defect cavity (cartilage flow phenomenon) and showed signs of degradation with chondrocyte clustering and a significant loss of GAG-positive stain of the ECM (Figure 5). New trabecular bone formation was conducted by enchondral ossification at the defect edges (Figure 5) and restored the subchondral trabecular bone integrity partially, reaching a maximum of 40–50% at 12 and 70–80% at 52 weeks. After one year, ulceration with erosive degradation of the defect side was present macroscopically. The repair tissue was mainly fibrous, with capillary vessels and fat vacuoles and the surface showed severe fibrillation with strong disruption and cyst formation in the subchondral bone (Figure 4c). Only two untreated defects (5.4 × 10 mm) showed nearly complete subchondral bone repair up to the original level, covered with GAG-rich fibrocartilaginous repair tissue. In 90 osteochondral defects with or without treatment, there was no correlation between the age of the animal and the amount of Safranin-O or collagen type II positive repair tissue formation. There was also no correlation between age and the total histomorphological score values (Mainil-Varlet et al. 2001).
Representative photomicrographs of osteochondral articular cartilage defects (5.4 × 8 mm) in the trochlear groove, showing repair at 6 (a), 12 (b) and 52 (c) weeks postoperatively (Gotterbarm et al. 2006). After 6 and 12 weeks, mainly fibrous tissue with some fibrocartilage was filling the defect void. At one year, repair tissue quality was mainly fibrous along with strong disruption and cyst formation in the subchondral bone. (Toluidine-blue, 5 μm centre-cut paraffin sections, original magnification 12.5-fold)
Photomicrograph of the upper defect edge of an osteochondral defect six weeks postoperatively. New trabecular bone formation was conducted by enchondral ossification at the defect edge. The adjacent cartilage showed a cartilage flow phenomenon and showed chondrocyte clustering with loss of GAG-positive staining. (Toluidine-blue, 5 μm centre-cut paraffin sections, original magnification 50-fold)
Discussion
Endogenous articular cartilage repair is limited due to its distinct histoanatomical structure (Mankin 1982). Therefore, cell-based strategies and principles from tissue-engineering evolved in order to overcome these limitations with the final goal to regenerate destroyed articular cartilage and restore joint function (Hunziker 2002). The process of the embryonic development of articular cartilage, with its distinct mechanical and biophysiological environment is not fully understood. In vitro research is an important tool for gaining knowledge of the interaction of cells, scaffolds, cytokines and mechanical stimuli, but mimicking and duplicating the processes which take place during articular cartilage development and repair are virtually impossible. Hence, there is still a strong need for animal models in tissue engineering and experimental joint surgery to evaluate the expected impact of new cell-based strategies on articular cartilage repair.
Various animal models have been established for experimental research on cartilage repair. Among the most common are rabbit (O'Driscoll et al. 1988, Grande et al. 1989, Wakitani et al. 1998), dog (Breinan et al. 1997, Nehrer et al. 1998, Cook et al. 2003), sheep (Homminga et al. 1991, Solchaga et al. 1996, Dorotka et al. 2005, Hoemann et al. 2005), goat (Butnariu-Ephrat et al. 1996, van Susante et al. 1999, Driesang & Hunziker 2000, Jackson et al. 2001, Dell'Accio et al. 2003, Brehm et al. 2006, Lu et al. 2006) and horse (Convery et al. 1972, Vachon et al. 1991, Nixon et al. 2000, Litzke et al. 2004, Frisbie et al. 2006). Each of these species has certain advantages and disadvantages, which one has to consider in order to choose the appropriate model in experimental in vivo research. It is common sense that larger animal models may more closely imitate the human setting than smaller animals such as rabbits, rats or mice (Reinholz et al. 2004). In this regard, the horse model with large joint dimension, thick articular cartilage layer and fully extended, upright stifle joints during gait must be considered as very similar to the anatomy of a human knee joint. Monetary and practical reasons limit the use and feasibility of the horse model to institutions with the appropriate constructional requirements for animal care and OR facilities. Not surprisingly, based on the easiness of handling, the need for small cages and low cost animal purchase and care, the most popular animal model used in experimental research on cartilage repair is the rabbit model. It has already been proposed that one of the limiting factor of this model is the thickness of the articular cartilage (Hunziker 1999, Breinan et al. 2001). An elaborate analysis revealed a mean cartilage thickness at the trochlear groove of 440 ± 80 μm and 300 ± 70 μm at the anteromedial femoral condyle, respectively (Rasanen & Messner 1996). This does allow creating only very small and shallow articular cartilage defects. In addition, the articular cartilage in rabbit osteochondral defects only represents about 5% of the total defect volume (Hunziker 1999). Small femoral and tibial bones also limit the size of the knee joint cavity itself and joint mechanics have to be considered very differently in humans. The endogenous healing potential in the rabbit model might also differ from the human situation as the bone turnover in rabbits is about 60 times faster than in humans (Osborn 1985). We therefore conclude that the rabbit model might be useful to principally prove the effect of new procedures, but based on the abovementioned limitations, larger animal models are more relevant when translating new findings into the human setting for preclinical testing.
The GMP is a well-established model in dental and craniomaxillofacial surgery (Hönig & Merten 1993, Amarante et al. 1995, Herring et al. 2002). The GMP was also used for studies on bone metabolism (Borah et al. 2002, Tsutsumi et al. 2004), bone and fracture repair (Wiese & Merten 1993, Raschke et al. 1999, Merten et al. 2000, Schnettler et al. 2003), implant fixation (Buser et al. 1991, Wong et al. 1995) and total hip replacement (Thomsen et al. 1997) in orthopaedic research. Earlier studies have shown that the physiological and chemical parameters of the GMP such as blood count and blood clotting, electrolytes, and liver enzymes are, unlike in dogs or sheep, similar to the values found in humans (Marshall et al. 1972, Hönig & Merten 1993, Rispat et al. 1993). Histomorphometric analysis of peripheral bone (Hönig & Merten 1993) has shown that the bone apposition rate and trabecular thickness in the GMP resemble the human bone. Despite the lack of any detailed quantitative analysis on the structure and organization of adult minipig articular cartilage, Kaab et al. (1998) were able to show by freeze-fracture scanning electron microscopy (SEM) analysis that the collagen fibre arrangement in pig articular cartilage is very similar to the leaf-like arrangement found in humans, whereas cow, sheep, rabbit or rat present a columnar pattern. Some investigators have chosen the GMP for in vivo evaluation of experimental articular cartilage repair. Hunziker and colleagues created superficial partial thickness (Hunziker & Rosenberg 1996, Hembry et al. 2001, Hunziker 2001, Hunziker et al. 2001a, Hunziker & Quinn 2003) as well as full-thickness articular cartilage defects (Hunziker et al. 2001b, Hunziker & Driesang 2003), and subsequently treated with various tissue engineering-based strategies including different growth factors and scaffolds. The authors clearly demonstrated that partial thickness defects do not heal spontaneously in the GMP model. Mainil-Varlet et al. (2001) have created full-thickness articular cartilage defects and followed up for 24 weeks. They showed, in analogy to our findings, that such defects did only fill with a fibrous repair tissue when examined 24 weeks after surgery.
In our chosen defect model within the stifle joint of the miniature pig, we clearly distinguished between chondral and osteochondral defects (penetration of the subchondral bone plate into the marrow space). The created chondral defect was best described as a ‘full-thickness’ defect, which comprised a complete removal of the articular cartilage down to the subchondral bone, with attention paid not to penetrate. The defect size was limited by the width of the medial facet of the trochlear groove and allowed a maximal diameter of 6.3 mm in diameter. Histomorphology showed fibrous and fibrocartilage-like repair tissue formation 12 weeks after surgery. Subsequent long-term follow-up for 52 weeks revealed a breakdown with severe signs of degradation. This strongly indicates that fibrocartilage is incapable of withstanding the biomechanical environment of a loaded joint over time (Mankin 1982). Even if we did not see intraoperative bleeding, postmortal histomorpholgical analysis revealed repair tissue merging from the subchondral space, indicating a disruption of the subchondral bone plate. It was already reported by Breinan and co-workers (Breinan et al. 2001) in the dog model that there is in fact a significant correlation between the depth of a chondral defect, e.g. disruption of the calcified cartilage and the amount of repair tissue filling the defect void. As we found nearly complete filling of the defect void 12 weeks postoperatively, we must have somehow opened the marrow space during defect preparation. For scientific reasons it is of major interest to clearly distinguish between a disrupted or intact subchondral bone plate, as opening the marrow space generally induces fibrocartilage repair tissue. On the other hand, a defect setting with complete removal of the articular cartilage more closely resembles the clinical situation of an abraded and eburnized joint surface. Our findings strengthen the importance of applied surgical technique for creating chondral defects and also point out that a follow up of less than a year might be misleading as the durability of the generated repair tissue in the biomechanical environment of a functional joint is clearly time-dependent.
Osteochondral defects of either size (5.4 × 8 mm or 6.3 × 10 mm) did show incomplete filling throughout evaluation. Enchondral bone formation was found at the defect edges and bone restoration reached a maximum of 80% after one year. There was a noticeable variability in the endogenous repair response, host bone collapse and cyst formation evident in defects of either size, whereas in two defects (5.4 × 8 mm) nearly complete restoration of the subchondral bone became evident. In this context, the term ‘critical size defect’ has been used for defects of a certain size above which no healing/regeneration occurs. We consider both osteochondral defects evaluated as ‘critical size defects’ but osteochondral defects at 6.3 × 10 mm are more likely to be incapable of healing. We have also investigated the endogenous repair of osteochondral defects (6.3 × 10 mm) in the central portion of the medial femoral condyle in the minipig model (unpublished data). There was a dramatic difference in bone repair when compared with the trochlear defect location. In this case, restoration of the subchondral bone plate was completed by enchondral bone formation starting form the upper defect edges. But, a remaining subchondral cystic cavity was found in the bone stock, similar to the reports of Jackson et al. (2001) in the goat model. These findings are most likely due to an increased mechanical loading on the convex joint surface, as there is evidence of increased contact stress at the rim of osteochondral defects in the femoral condyles (Brown et al. 1991). Mean cartilage thickness of the lateral facet of the trochlear groove in the GMP was found to be 0.5 mm reaching a maximum of 0.8 mm in some individuals. Significant higher values were found in male GMP. These data indicate thicker articular cartilage in the GMP when compared with the rabbit model (~0.4 mm) (Rasanen & Messner 1996), but similar values are found in the canine model (0.5–0.8 mm) (Shortkroff et al. 1996). Cartilage thickness therefore still has to be considered as a limiting factor when translating findings into the human system (~2–3 mm) (Shortkroff et al. 1996, Hunziker et al. 2002). To gain access to the patellofemoral joint we have chosen a transligamentous approach instead of a parapatellar incision with median capsulotomy. Although splitting the patellar ligament limited the field of operation, we were still able to expose the complete trochlear groove and to perform microsurgery techniques for implant fixation. In addition, this technique has to be considered as less traumatic and preventive for patellar maltracking or dislocation. We do not have experience in the use of an external fixation device to restrict postoperative mobilization. Such means might be useful in future in order to prevent postoperative implant dislocations if delicate fixation techniques (e.g. stitching or gluing) are applied (Driesang & Hunziker 2000, Mainil-Varlet et al. 2001).
Our work demonstrates the main characteristics of the GMP as a model for evaluating tissue engineering-based chondral and osteochondral defect repair. Histomorphological analysis has clearly shown that the endogenous repair of untreated chondral and osteochondral defects within this species is limited and therefore allows a critical assessment of new treatment strategies. This model allows an intra-individual left vs. right comparison with a low complication rate of approximately 2%. The GMP therefore seems to be a useful in vivo model for investigative work on tissue engineering-based articular cartilage repair.
References
1.
AmaranteMT, ConstantinescuMA, O'ConnorD, YaremchukMJ (1995) Biomechanical evaluation of the canine and porcine models for experimental craniofacial surgery. Journal of Craniofacial Surgery6, 288–91.
2.
BobicV (1999) Autologous osteo-chondral grafts in the management of articular cartilage lesions. Orthopäde28, 19–25.
3.
BorahB, DufresneTE, ChmielewskiPA. (2002) Risedronate preserves trabecular architecture and increases bone strength in vertebra of ovariectomized minipigs as measured by three-dimensional microcomputed tomography. Journal of Bone Mineral Research17, 1139–47.
4.
BrehmW, AklinB, YamashitaT. (2006) Repair of superficial osteochondral defects with an autologous scaffold-free cartilage construct in a caprine model: implantation method and short-term results. Osteoarthritis Cartilage14, 1214–26.
5.
BreinanHA, HsuHP, SpectorM (2001) Chondral defects in animal models: effects of selected repair procedures in canines. Clinical Orthopaedics and related Research391: (suppl.), S219–30
6.
BreinanHA, MinasT, HsuHP. (1997) Effect of cultured autologous chondrocytes on repair of chondral defects in a canine model. Journal of Bone and Joint Surgery: American Volume79, 1439–51.
7.
BrittbergM, LindahlA, NilssonA. (1994) Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. New England Journal of Medicine331, 889–95.
8.
BrownTD, PopeDF, HaleJE, BuckwalterJA, BrandRA (1991) Effects of osteochondral defect size on cartilage contact stress. Journal of Orthopaedic Research9, 559–67.
9.
BuserD, SchenkRK, SteinemannS. (1991) Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. Journal of Biomedical Material Research25, 889–902.
10.
Butnariu-EphratM, RobinsonD, MendesDG, HalperinN, NevoZ (1996) Resurfacing of goat articular cartilage by chondrocytes derived from bone marrow. Clinical Orthopaedics and Related Research330, 234–43.
11.
ConveryFR, AkesonWH, KeownGH (1972) The repair of large osteochondral defects. An experimental study in horses. Clinical Orthopaedics and Related Research82, 253–62.
12.
CookSD, PatronLP, SalkeldSL, RuegerDC (2003) Repair of articular cartilage defects with osteogenic protein-1 (BMP-7) in dogs. Journal of Bone and Joint Surgery: American Volume85-A: (suppl. 3), 116–23
13.
Dell'AccioF, VanlauweJ, BellemansJ. (2003) Expanded phenotypically stable chondrocytes persist in the repair tissue and contribute to cartilage matrix formation and structural integration in a goat model of autologous chondrocyte implantation. Journal of Orthopaedic Research21, 123–31.
14.
DorotkaR, WindbergerU, MacfeldaK. (2005) Repair of articular cartilage defects treated by microfracture and a three-dimensional collagen matrix. Biomaterials26, 3617–29.
15.
DraenertK, DraenertY (1988) A new procedure for bone biopsies and cartilage and bone transplantation. SandoramaIII-IV, 33–40.
16.
DriesangIM, HunzikerEB (2000) Delamination rates of tissue flaps used in articular cartilage repair. Journal of Orthopaedic Research18, 909–11.
17.
FrisbieDD, MorissetS, HoCP. (2006) Effects of calcified cartilage on healing of chondral defects treated with microfracture in horses. American Journal of Sports Medicine34, 1824–31.
18.
GotterbarmT (2003) Thesis: Neue Konzepte zur Behandlung chondraler und osteochondraler Defekte - eine tierexperimentelle Untersuchung. Heidelberg, Medizinische Fakultät der Ruprecht-Karls Universität, 1-201
19.
GotterbarmT, ReitzelT, SchneiderU. (2003) Integration of periosteum covered autogenous bone grafts with and without autologous chondrocytes. An animal experiment using the Gottinger minipig. Orthopäde32, 65–73.
20.
GotterbarmT, RichterW, JungM. (2006) An in vivo study of a growth-factor enhanced, cell free, two-layered collagen-tricalcium phosphate in deep osteochondral defects. Biomaterials27, 3387–95.
21.
GrandeDA, PitmanMI, PetersonL, MencheD, KleinM (1989) The repair of experimentally produced defects in rabbit articular cartilage by autologous chondrocyte transplantation. Journal of Orthopaedic Research7, 208–18.
22.
HangodyL, FulesP (2003) Autologous osteochondral mosaicplasty for the treatment of full-thickness defects of weight-bearing joints: ten years of experimental and clinical experience. Journal of Bone and Joint Surgery: American Volume85-A: (suppl. 2), 25–32
23.
HembryRM, DyceJ, DriesangI. (2001) Immunolocalization of matrix metalloproteinases in partial-thickness defects in pig articular cartilage. A preliminary report. Journal of Bone and Joint Surgery: American Volume83-A, 826–38.
24.
HerringSW, DeckerJD, LiuZJ, MaT (2002) Temporomandibular joint in miniature pigs: anatomy, cell replication, and relation to loading. Anatomical Record266, 152–66.
25.
HochDH, GrodzinskyAJ, KoobTJ, AlbertML, EyreDR (1983) Early changes in material properties of rabbit articular cartilage after meniscectomy. Journal of Orthopaedic Research1, 4–12
26.
HoemannCD, HurtigM, RossomachaE. (2005) Chitosan-glycerol phosphate/blood implants improve hyaline cartilage repair in ovine microfracture defects. Journal of Bone and Joint Surgery: American Volume87, 2671–86.
27.
HommingaGN, BulstraSK, KuijerR, van der LindenAJ (1991) Repair of sheep articular cartilage defects with a rabbit costal perichondrial graft. Acta Orthopaedica Scandinavica62, 415–18.
28.
HönigJF, MertenHA (1993) Das Göttinger Miniaturschwein (GMS) als Versuchtier in der human-medizinischen osteologischen Grundlagenforschung. Z Zahnärztl ImplantolIX, 244–54.
29.
HunzikerEB (1999) Biologic repair of articular cartilage. Defect models in experimental animals and matrix requirements. Clinical Orthopaedics and Related Research367: (suppl.), S135–46
30.
HunzikerEB (2001) Growth-factor-induced healing of partial-thickness defects in adult articular cartilage. Osteoarthritis Cartilage9, 22–32.
31.
HunzikerEB (2002) Articular cartilage repair: basic science and clinical progress. A review of the current status and prospects. Osteoarthritis Cartilage10, 432–63.
HunzikerEB, DriesangIM, MorrisEA (2001a) Chondrogenesis in cartilage repair is induced by members of the transforming growth factor-beta superfamily. Clinical Orthopaedics and Related Research391: (suppl.), S171–81
34.
HunzikerEB, DriesangIM, SaagerC (2001b) Structural barrier principle for growth factor-based articular cartilage repair. Clinical Orthopaedics and Related Research391: (suppl.), S182–9
35.
HunzikerEB, QuinnTM (2003) Surgical removal of articular cartilage leads to loss of chondrocytes from cartilage bordering the wound edge. Journal of Bone and Joint Surgery: American Volume85-A: (suppl. 2), 85–92
36.
HunzikerEB, QuinnTM, HauselmannH (2002) Quantitative structural organization of normal adult human articular cartilage. Osteoarthritis Cartilage10, 564–72.
37.
HunzikerEB, RosenbergLC (1996) Repair of partial-thickness defects in articular cartilage: cell recruitment from the synovial membrane. Journal of Bone and Joint Surgery: American Volume78, 721–33.
38.
JacksonDW, LalorPA, AbermanHM, SimonTM (2001) Spontaneous repair of full-thickness defects of articular cartilage in a goat model. A preliminary study. Journal of Bone and Joint Surgery: American Volume83-A, 53–64.
39.
JungM, GotterbarmT, GruettgenA. (2005) Molecular characterization of spontaneous and growth-factor-augmented chondrogenesis in periosteum-bone tissue transferred into a joint. Histochemistry and Cell Biology123, 447–56.
40.
KaabMJ, GwynnIA, NotzliHP (1998) Collagen fibre arrangement in the tibial plateau articular cartilage of man and other mammalian species. Journal of Anatomy193, 23–34.
41.
KnutsenG, EngebretsenL, LudvigsenTC. (2004) Autologous chondrocyte implantation compared with microfracture in the knee. A randomized trial. Journal of Bone and Joint Surgery: American Volume86-A, 455–64.
42.
LitzkeLE, WagnerE, BaumgaertnerW. (2004) Repair of extensive articular cartilage defects in horses by autologous chondrocyte transplantation. Annals of Biomedical Engineering32, 57–69.
43.
LuY, DhanarajS, WangZ. (2006) Minced cartilage without cell culture serves as an effective intraoperative cell source for cartilage repair. Journal of Orthopaedic Research24, 1261–70.
44.
Mainil-VarletP, RieserF, GroganS. (2001) Articular cartilage repair using a tissue-engineered cartilage-like implant: an animal study. Osteoarthritis Cartilage9: (suppl. A), S6–15
45.
MankinHJ (1982) The response of articular cartilage to mechanical injury. Journal of Bone and Joint Surgery: American Volume64, 460–6.
46.
MarshallM, LydtinH, KrawietzW. (1972) Das Miniaturschwein als Versuchtier in der experimentellen Medizin. Research in Experimental Medicine157, 300
47.
MertenHA, WiltfangJ, HonigJF, FunkeM, LuhrHG (2000) [Intra-individual comparison of alpha- and beta-TCP ceramics in an animal experiment]. Mund Kiefer Gesichtschir4: (suppl. 2), S509–15
48.
NehrerS, BreinanHA, RamappaA. (1998) Chondrocyte-seeded collagen matrices implanted in a chondral defect in a canine model. Biomaterials19, 2313–28.
49.
NixonAJ, Brower-TolandBD, BentSJ. (2000) Insulin-like growth factor-I gene therapy applications for cartilage repair. Clinical Orthopaedics and Related Research379: (suppl.), S201–13
50.
O'DriscollSW, KeeleyFW, SalterRB (1988) Durability of regenerated articular cartilage produced by free autogenous periosteal grafts in major full-thickness defects in joint surfaces under the influence of continuous passive motion. A follow-up report at one year. Journal of Bone and Joint Surgery: American Volume70, 595–606.
RasanenT, MessnerK (1996) Regional variations of indentation stiffness and thickness of normal rabbit knee articular cartilage. Journal of Biomedical Materials Research31, 519–24.
53.
RaschkeMJ, BailH, WindhagenHJ. (1999) Recombinant growth hormone accelerates bone regenerate consolidation in distraction osteogenesis. Bone24, 81–8
RispatG, SlaouiM, WebeD. (1993) Haematological and plasma biochemical values for healthy Yucatan micropigs. Laboratory Animals27, 368–73.
56.
SchneiderU, GotterbarmT, VossHJ. (2006) Comparative study of traditional ACT and a novel collagen-gel based matrix augmented with autogenous chondrocytes in a minipig model. In: Basic Science, Clinical Repair and Reconstruction of Articular Cartilage Defects: Current Status and Prospects (ZanasiS, BrittbergM, MarcacciM, eds). Bologna: Timeo Editore, 743–53
57.
SchnettlerR, AltV, DingeldeinE. (2003) Bone ingrowth in bFGF-coated hydroxyapatite ceramic implants. Biomaterials24, 4603–8.
58.
ShortkroffS, BaroneL, HsuHP. (1996) Healing of chondral and osteochondral defects in a canine model: the role of cultured chondrocytes in regeneration of articular cartilage. Biomaterials17, 147–54.
59.
SolchagaL, ForriolF, CanadellJ (1996) Repair of articular cartilage with biological tissues. An experimental study in sheep. Revue de Chirurgie Orthopedique et Reparatrice de Appareil Moteur82, 101–7.
60.
SolchagaLA, GoldbergVM, CaplanAI (2001) Cartilage regeneration using principles of tissue engineering. Clinical Orthopaedics and Related Research391: (suppl.), S161–70
61.
SteadmanJR, RodkeyWG, RodrigoJJ (2001) Microfracture: surgical technique and rehabilitation to treat chondral defects. Clinical Orthopaedics and Related Research391: (suppl.), S362–9
62.
ThomsenM, von StrachwitzB, LoewM. (1997) [The Gottinger minipig as an animal model in hip endoprosthesis. Anatomy, anesthesia, operation results]. Zeitschrift fur Orthopadie und Ihre Grenzgebeite135, 58–62.
63.
TsutsumiH, KatagiriK, MorimotoM. (2004) Diurnal variation and age-related changes of bone turnover markers in female Gottingen minipigs. Laboratory Animals38, 439–46.
64.
VachonAM, McIlwraithCW, TrotterGW, NorrdinRW, PowersBE (1991) Morphologic study of repair of induced osteochondral defects of the distal portion of the radial carpal bone in horses by use of glued periosteal autografts. American Journal of Veterinary Research52, 317–27.
65.
van SusanteJL, BumaP, SchumanL. (1999) Resurfacing potential of heterologous chondrocytes suspended in fibrin glue in large full-thickness defects of femoral articular cartilage: an experimental study in the goat. Biomaterials20, 1167–75.
66.
WakitaniS, GotoT, YoungRG. (1998) Repair of large full-thickness articular cartilage defects with allograft articular chondrocytes embedded in a collagen gel. Tissue Engineering4, 429–44.
67.
WakitaniS, KimuraT, HirookaA. (1989) Repair of rabbit articular surfaces with allograft chondrocytes embedded in collagen gel. The Journal of Bone and Joint Surgery: British Volume71, 74–80.
68.
WieseKG, MertenHA (1993) The role of the periosteum in osteointegration of hydroxyapatite granules. International Journal of Oral and Maxillofacial Surgery22, 306–8.
69.
WongM, EulenbergerJ, SchenkR, HunzikerE (1995) Effect of surface topology on the osseointegration of implant materials in trabecular bone. Journal of Biomedical Materials Research29, 1567–75.