
Abstract
This case highlights the risks of long-term unopposed oestrogen therapy after hysterectomy in a patient with a history of severe endometriosis.
Introduction
High levels of oestrogens are a strong risk factor for endometrial adenocarcinoma. Therefore, at present, guidelines state that unopposed oestrogen hormone replacement therapy (HRT) is recommended only for patients who have had a hysterectomy. 1 However in patients with endometriosis who have had a total abdominal hysterectomy and salpingo-oophorectomy (TAHBSO), unopposed oestrogens may cause a malignant change in any remaining endometrial deposits. We describe such a case presenting with bowel obstruction. As a result, we propose regular reviews for patients with endometriosis taking HRT post-TAHBSO. This will ensure that the advantages of HRT continue to outweigh the disadvantages.
Case report
A 78-year-old woman presented to the emergency department with a two-day history of severe abdominal pain, absolute constipation and bilious vomiting. For the past year she had experienced churning lower abdominal pains and an increased frequency of defecation (5–6 times per day on average). She did not complain of weight loss, bleeding per rectum, or any genito-urinary symptoms. Her past medical history included severe endometriosis and fibroids. As a consequence, in 1976, she underwent a TAHBSO. Following surgery, she received oestradiol implants for symptom control. Postsurgery she was found to have regularly high oestradiol levels; in 1990 her oestradiol level was measured at 1102 pg/mL (normal 50–400 pg/mL). As a result, she was switched to oestrogen patches (100 mg), and remained on these until the age of 76.
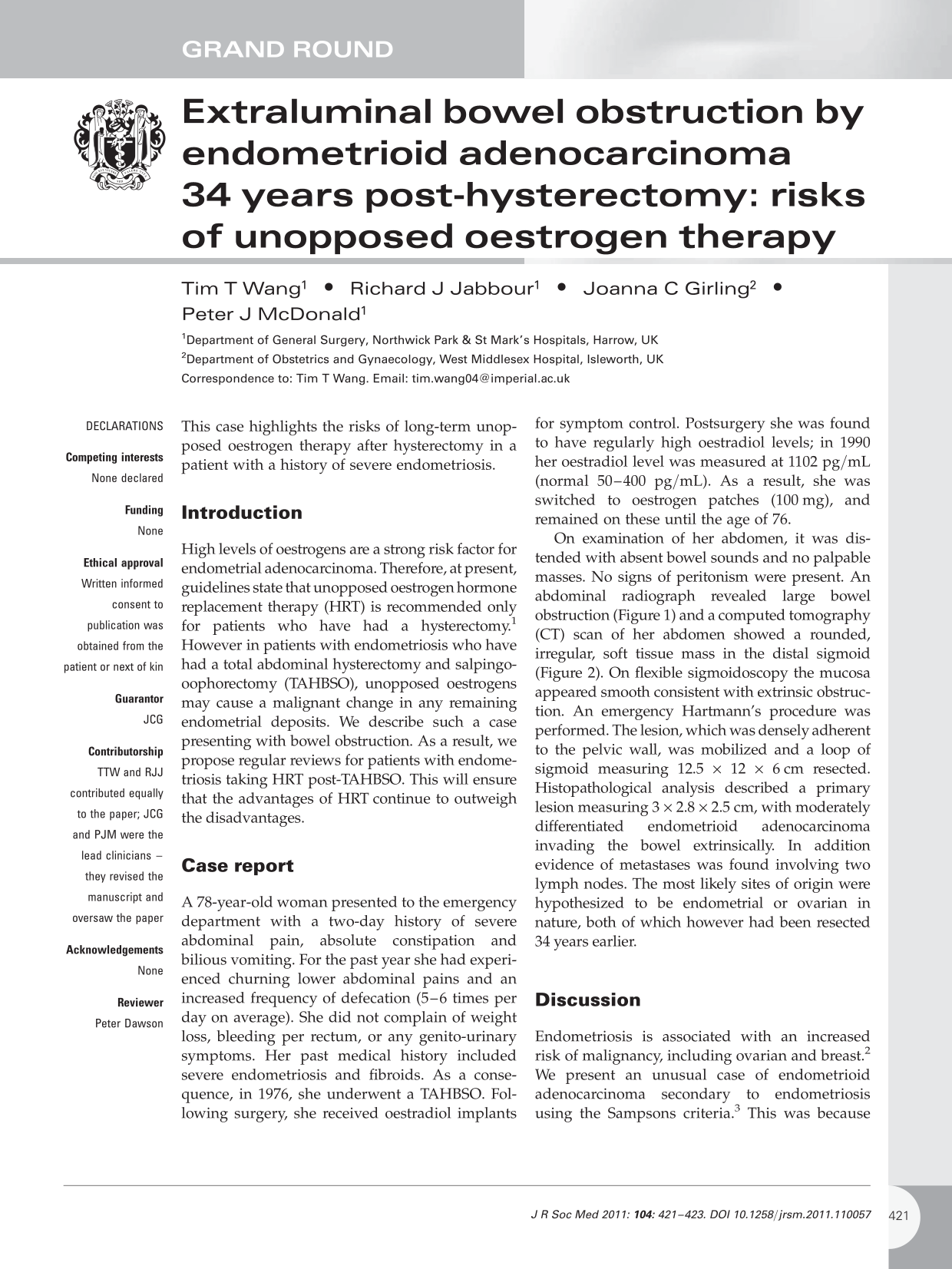
On examination of her abdomen, it was distended with absent bowel sounds and no palpable masses. No signs of peritonism were present. An abdominal radiograph revealed large bowel obstruction (Figure 1) and a computed tomography (CT) scan of her abdomen showed a rounded, irregular, soft tissue mass in the distal sigmoid (Figure 2). On flexible sigmoidoscopy the mucosa appeared smooth consistent with extrinsic obstruction. An emergency Hartmann's procedure was performed. The lesion, which was densely adherent to the pelvic wall, was mobilized and a loop of sigmoid measuring 12.5 × 12 × 6 cm resected. Histopathological analysis described a primary lesion measuring 3 × 2.8 × 2.5 cm, with moderately differentiated endometrioid adenocarcinoma invading the bowel extrinsically. In addition evidence of metastases was found involving two lymph nodes. The most likely sites of origin were hypothesized to be endometrial or ovarian in nature, both of which however had been resected 34 years earlier.

Abdominal radiograph taken during admission in the emergency department showing signs of large bowel obstruction
Abdominal CT scan (axial view) identifying a mass in the pelvis causing compression of the sigmoid colon
Discussion
Endometriosis is associated with an increased risk of malignancy, including ovarian and breast. 2 We present an unusual case of endometrioid adenocarcinoma secondary to endometriosis using the Sampsons criteria. 3 This was because no additional primary tumour was found on investigation, the site of endometriosis and the malignant tissue were adjacent to each other, and the histology confirmed endometrial tissue. In the literature, 15 cases of endometrioid adenocarcinoma arising in patients post-TAHBSO have been reported to date. 4 Our case is unusual because: (a) the patient presented with bowel obstruction; (b) the patient underwent TAHBSO 34 years previously; (c) the patient had consistently high oestrodial levels for over 10 years and was managed with oestrogen implants until the age of 76.
Hormone replacement therapy in patients following hysterectomy has significant benefits for a number of reasons including symptom control, improving libido and bone protection. 5 Currently, according to the Green Top guidelines, there is no consensus as to the correct choice of HRT in patients with TAHBSO due to endometriosis. 6 As a result the correct HRT regimen is determined on an individual basis. 6 Unopposed oestrogen implants have been associated with a higher rate of malignant transformation. 7 However, delaying HRT following pelvic clearance surgery is not beneficial. 7 Therefore we recommend that clinicians re-assess on a regular basis the pros and cons of HRT in these types of patients, avoiding implants where possible and being aware of an unusual differential in patients presenting with bowel obstruction who have a background of endometriosis and TAHBSO.
Further research is needed to reveal the ideal HRT regimen in patients who have undergone TAHBSO for extensive endometriosis and should include investigations as to whether combined HRT (oestrogens and progestins) minimizes the risk of malignant transformation.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Written informed consent to publication was obtained from the patient or next of kin
Guarantor
JCG
Contributorship
TTW and RJJ contributed equally to the paper; JCG and PJM were the lead clinicians – they revised the manuscript and oversaw the paper
Acknowledgements
None
Reviewer
Peter Dawson