
Abstract
Objectives
To estimate incidence of injury to patients attributed to misadventures during surgical and medical care by age group and to examine recent trends.
Design
Analysis of routine morbidity and mortality data categorized by the 9th and 10th revisions of the International Classification of Diseases.
Participants
Children 0–14 years and adults ≥15 years.
Setting
England and Wales during 1999 to 2008 (hospital episodes) and 1979 to 2009 (deaths).
Main outcome measures
We calculated deaths per million person-years and per 1000 hospital episodes; hospital episodes per 100,000 person-years and per 100,000 procedures performed.
Results
The rate of death attributed to misadventures during surgical and medical care in patients aged 75 years and older was over 50 times (rate ratio 57.2; 95% confidence interval 38.3–85.3) higher than in children aged 1–14 years. Estimated hospital episode rates were 20 times (RR 20.0; 18.9–21.2) higher in patients aged 75 years and older. Mortality attributed to misadventures declined from 1.1 (0.9–1.4) deaths per million person-years in 1979 to 0.4 (0.2–0.6) in 2009. Hospital episodes of misadventures decreased between 1999 and 2008 from 30.8 (29.9–31.8) episodes per 100,000 procedures to 23.25 (22.5–24.1), but increased from 7.8 (7.6–8.1) per 100,000 person-years to 9.8 (9.5–10.1).
Conclusions
Misadventures during surgical and medical care are an important cause of avoidable injury. Older patients appear to be at higher risk of experiencing and dying from misadventure. Interpretation of recent trends is limited by uncertainties regarding the consistency and coverage of coding.
Introduction
Injury to patients caused by medical error and adverse events associated with healthcare is an important health concern. It is estimated that 10% of National Health Service (NHS) patients experience an adverse event while in hospital, one-third of which lead to moderate levels of disability or death. 1 The associated economic costs are substantial – compensation payments for clinical negligence cost the NHS in England over £780 million in the 2009–2010 financial year alone. 2
Since the introduction of the 9th revision of the International Classification of Diseases (ICD) in 1979, ‘Misadventures to patients during surgical and medical care’ have been distinguished as a specific external cause of mortality and morbidity. Unlike injury from other external causes such as transport accidents, assaults, falls or fires, there has been little published analysis of routine data on misadventures during surgical and medical care. Routine mortality data and hospital episode statistics have the advantage of being regularly updated and maintained as well as offering a cost-effective alternative to data from small-scale case-note surveys or from reporting systems such as the National Safety Reporting System in England and Wales. 3 Furthermore, organizations such as the Healthcare Commission and Dr Foster have used routine data to monitor clinical performance and patient safety in the UK. 4,5
Our aim was to explore the incidence of injury due to misadventures during surgical and medical care in England and Wales by age and to examine recent trends.
Methods
We obtained mortality data and population denominator data from the Office for National Statistics (ONS) 6,7 for the years 1979–2009. In addition, data on morbidity were obtained from Hospital Episodes Statistics online (HES) 8 for England and from the Patient Episode Database for Wales (PEDW) 9 for the period 1 April 1999 to 31 March 2009. These data are publicly available from the publishers as anonymized data aggregated by age group.
All data sources utilize ICD to assign external causes of mortality or morbidity. Our study period spans two revisions of the ICD (versions 9 and 10) which we judged to be sufficiently consistent in their coding of misadventures to allow data from periods covered by these versions to be combined. We extracted all deaths and hospital episodes with external causes classified to ‘Misadventures to patients during surgical and medical care’, which correspond to ICD-10 external cause codes Y60-66 and Y69, and the equivalent ICD-9 E-codes (Table 1).
Mapping of ICD-9 and ICD-10 external cause classification for ‘Misadventures to patients during surgical and medical care’
We calculated mortality rates with 95% confidence intervals (CI) per million person-years. To estimate case-fatality rates we calculated deaths per 1000 hospital episodes of misadventures.
Morbidity data from HES and PEDW were combined to allow estimation of rates for England and Wales overall. We extracted data on the number of finished consultant episodes (a period of admitted care under a consultant or allied healthcare professional within an NHS trust) and the number of procedures and interventions (jointly referred to hereafter as ‘procedures’) performed each year. Within HES and PEDW procedures are recorded according to the Office of Population, Censuses and Surveys Classification of Operations and Procedures (OPCS-4) and include all operations and interventions that patients undergo during their hospital stay.
As an individual's risk of experiencing a misadventure depends on their exposure to medical and surgical care, we also examined the number of procedures per 1000 person-years. Hospital episode rates due to misadventure were estimated with 95% CI per 100,000 person-years and per 100,000 procedures.
The direct method was used to age-standardize incidence rates, using the year 2001 population as the standard. Differences in rates due to misadventures were examined according to age by estimating rate ratios and 95% CIs, calculated using the Poisson distribution. Age was grouped according to the categories used by HES, with the exception of an additional group (<1 year) for mortality data.
Results
Between 1979 and 2009 there were 1596 registered deaths attributed to misadventures during surgical and medical care in England and Wales, representing 1.00 (95% CI 0.95 to 1.05) deaths per million person-years. Table 2 shows average annual mortality rates by age. The rate ratios indicate increased mortality in the age groups: <1 year, 60–74 years and 75+ years. Mortality was over 50 times (rate ratio 57.2; 95% CI 38.3–85.3) higher in patients aged 75+ years than in children aged 1–14 years (Figure 1).
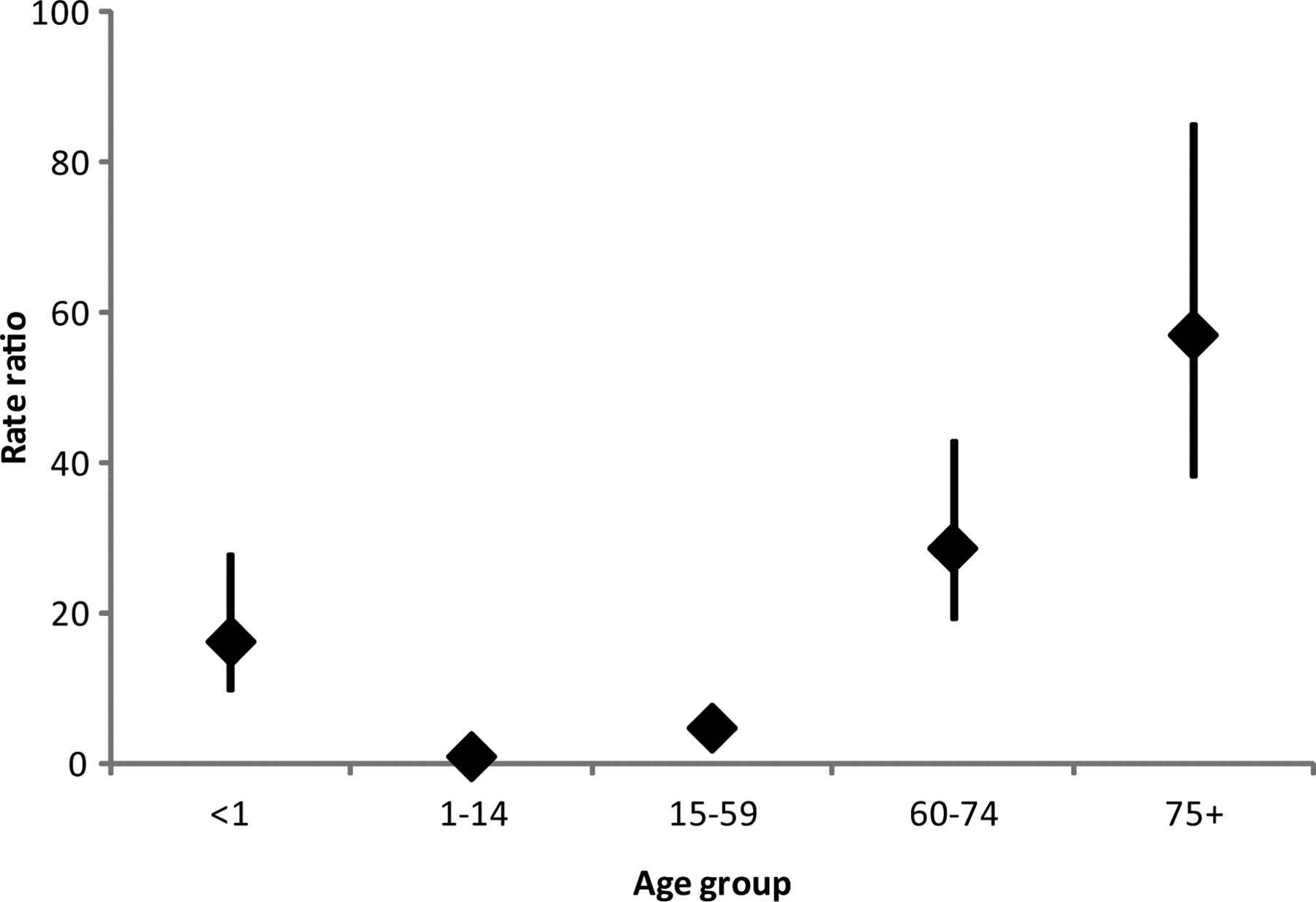
Mortality rate ratios (vertical lines show 95% CIs) by age group
Average annual rates of health events attributed to misadventures by age group
*Mortality data available separately for children aged under 1 year
†For case fatality rate deaths during 1999 to 2008 were used
During the period 1999–2008 there were 44,399 hospital episodes attributed to misadventures. Morbidity was also found to increase with age: the hospital episode rate estimated in the 75+ years age group was 20 times (RR 20.0; 18.9–21.2) higher than that in children aged 0–14 years (Table 2). The case-fatality rate (deaths per 1000 hospital episodes of misadventures) was lower in the 15–59-year age group than in the 0–14-year age group; no differences were observed for other age groups. The rates of procedures performed in hospital increased with age: among people aged 75+ years the rate was seven times higher than in children aged 0–14 years (RR 7.00; 6.99–7.01).
There was an overall decline in mortality from 1.1 (95% CI 0.9–1.4) deaths per million person-years in 1979 to 0.4 (95% CI 0.2–0.6) in 2009 (Figure 2). Between 1979 and 2000 the trend had been for an increase in deaths, but a sharp decline occurred between 2000 and 2001 and death rates continued to fall thereafter.

Age-standardized mortality per million person-years attributed to misadventures (three-year moving averages from 1979 to 2009)
Between 1999 and 2008 there was an increase in the number of procedures performed in all age groups (Figure 3). The number of procedures per 1000 person-years in the age groups 0–14 years, 15–59 years, 60–74 years and 75+ years increased by 31%, 47%, 80% and 94%, respectively. Hospital episodes per 100,000 procedures decreased by about one quarter from 30.8 (95% CI 29.9–31.8) in 1999 to 23.3 (95% CI 22.5–24.1) in 2008 (Figure 4). Conversely, the rate per 100,000 person-years increased from 7.8 (95% CI 7.6–8.1) to 9.8 (95% CI 9.5–10.1) over the same period.
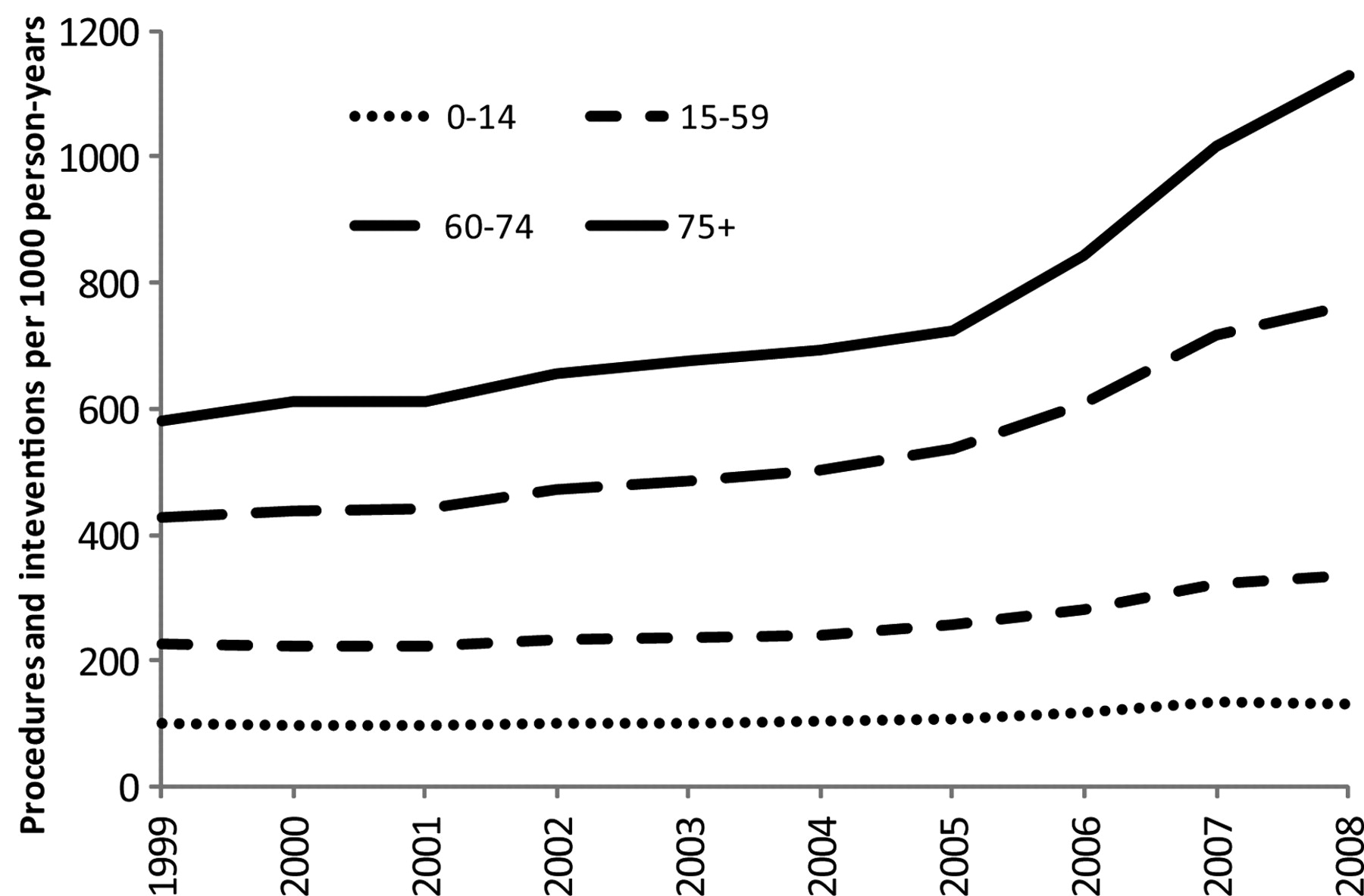
Procedures and interventions per 1000 person-years by age group (1999–2008)
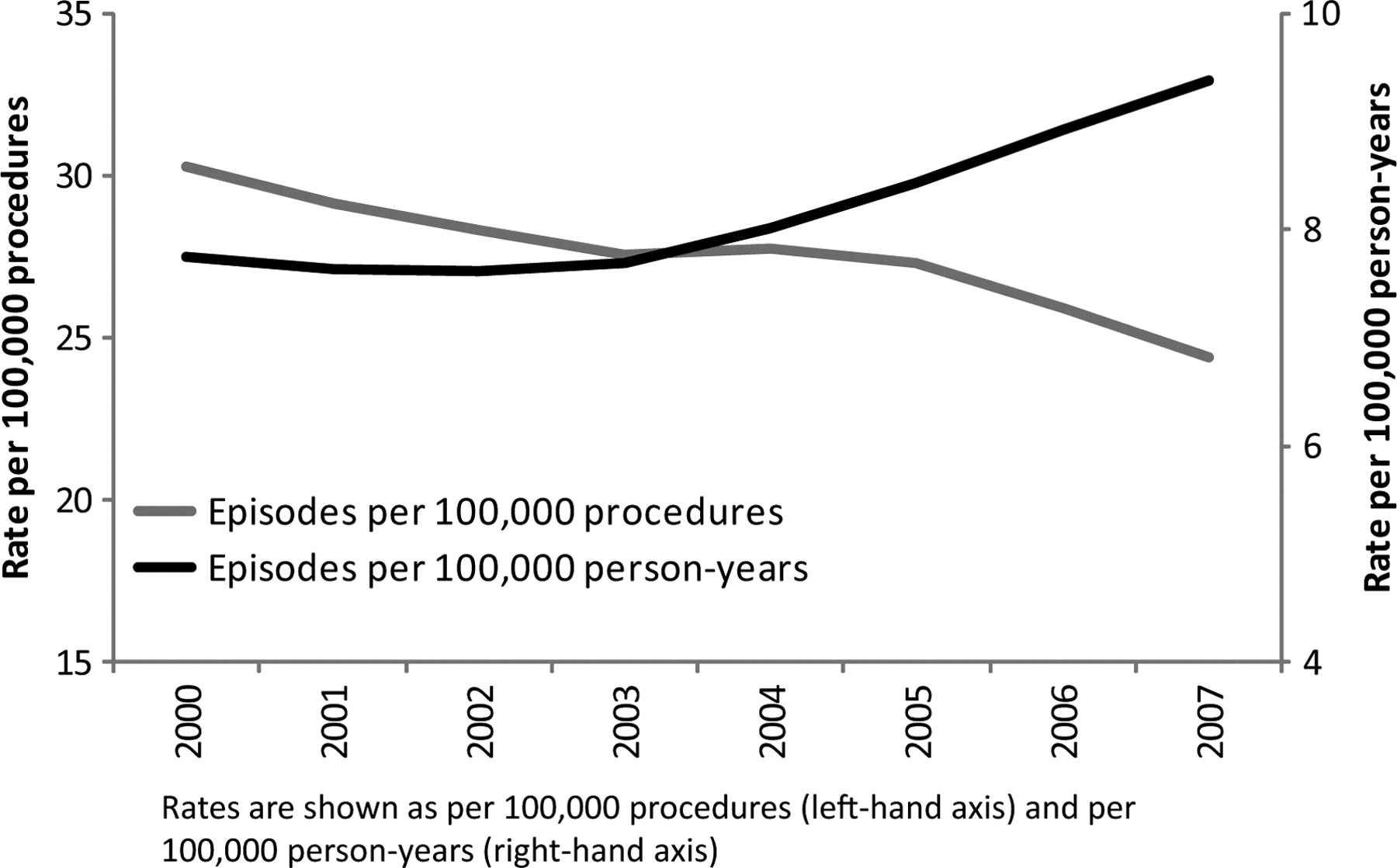
Age-standardized rate of hospital episodes attributed to misadventures (three-year moving averages from 1999 to 2008)
Discussion
Principal findings
Using 20 years of registered deaths in England and Wales we have found evidence that mortality attributed to misadventures during surgical and medical care is strongly associated with age, with higher rates in older age groups, an observed association also supported by almost 10 years of hospital episode statistics. The number of deaths attributed to misadventures has fallen over recent years, although the number of episodes attributed to misadventures has increased. Before we consider the implications for clinical practice and future research we will address the methodological limitations of this study.
Strengths and weaknesses of the study
Co-morbidities, common in older patients, can complicate the coding of health events and lead to their misclassification within routine data. This, coupled with the tendency not to code events to external causes in older persons, 10 would cause our findings to be under-estimates of the true excess rates of misadventures found in older age groups. Information bias is therefore unlikely to explain the association with age, although it may have diluted our observed effect.
Before examining recent trends, variations in the coding and reporting of misadventures must be considered. The apparent increase in episodes per population might be a result of improved reporting of events over time. In this study, the period for which morbidity data were drawn covers a time of growing awareness of patient safety issues, and includes the publication of seminal reports such as the Department of Health's An Organisation with a Memory 11 and establishment of the National Patient Safety Agency in the UK. It is therefore entirely reasonable to suspect an improvement in reporting of misadventures in routine data, which may explain the observed increase in episodes since 1999. However, the rate of deaths attributed to misadventures appeared to decline over the same period. It is not clear how an improved awareness would lead to greater coding and reporting of episodes attributed to misadventures, but not deaths.
A systematic change to data coding might also explain some of the apparent decline in deaths attributed to misadventures. Since 2001, there was a marked decrease in deaths coded as ‘Misadventures to patients during surgical and medical care’. Sudden changes in data may be explained as statistical artefact 12 and it is particularly notable that a decrease in deaths attributed to misadventures coincided with the introduction of the 10th revision of ICD. While the category ‘Misadventures to patients during surgical and medical care’ remained largely consistent between ICD-9 and ICD-10, other categories under ‘Complications during surgical and medical care’ (e.g. ‘Medical devices associated with adverse incidents in diagnostic and therapeutic use’ and ‘Drugs, medicaments and biological substances causing adverse effects in therapeutic use’) were substantially revised. Hence the observed decrease from 2001 onwards may be explained by a shift in classification of deaths from misadventures to other categories.
For these reasons it is not possible to draw confident conclusions from these data regarding the underlying trends in injury attributed to misadventures during surgical and medical care. Potential explanations for the sudden drop in deaths attributed to misadventures warrant investigation in future studies.
Comparison with other studies
This is the first study in England and Wales to examine routine mortality and morbidity data specifically on injury attributed to misadventures as classified by ICD. Our observed association with age is consistent with a previous case-note review 1 and analysis of HES data 5 which explored the wider category of adverse events in NHS healthcare, both of which observed higher rates of events among older patients.
The case-note review suggested that each year 10% of NHS patients experience an adverse event or medical error while in a NHS hospital, 1 a burden far greater than estimated by this study. As an indicator of healthcare quality, routine data offer high specificity but low sensitivity 4 and the coverage of external cause coding within HES data is known to be low. 13 Large numbers of false-negatives may therefore lead to artificially low estimated rates. For this reason the rates of misadventures presented in this study are likely to be ‘the tip of the iceberg’. However, while estimates obtained from analysis of routine data may have underestimated the true burden, our examination of the distribution of harm within these data sources by age remains valid.
Possible mechanisms and implications of study findings
Our study shows that older patients are more likely to experience a misadventure during surgical and medical care and are more likely to die as a result. One explanation for this is the frailty of older people, which alongside the presence of co-morbidities, is likely to affect their capacity to survive misadventures relative to younger patients. A fragile health status is also likely to account for much of the elevated mortality rate observed in children aged less than 1 year.
The higher rate of misadventures in older adults is likely to be a consequence of greater exposure to healthcare with advancing age. Furthermore, our study suggests that older age groups have experienced a greater increase in the number of procedures performed than the younger age groups. Despite being more vulnerable to misadventures, the data might suggest that older individuals are also being exposed to more procedures than in previous years.
It is also possible that older people undergo a greater number of complex, risky and invasive treatments which may be more prone to error. Moreover, there is concern that the potential adverse effects of treatments in older age groups may not have been fully evaluated, due in part to the common practice of excluding older patients from clinical trials. 14–16 The exclusion or under-representation of elderly patients in clinical trials forces clinicians treating these patients to make treatment decisions using evidence based on younger patients only. We have not explored the data further to assess whether these factors may explain the greater rates of misadventure in older individuals. Similarly, we cannot confirm or refute the possibility of a contributory role of poorer patient care experienced by older patients, which has been observed elsewhere. 17–19
Interpretation of the observed recent trends is constrained by uncertainty of the accuracy and consistency of coding within the routine data sources. The apparent decrease in the rate of misadventures per procedure may suggest that the safety of care has improved over recent years, although due to an increase in the number of procedures performed, the overall rate per population has actually increased. However, we cannot discount the possibility that information bias may partly explain these observed trends.
Future research
Misadventures to patients during surgical and medical care are an important cause of harm in England and Wales. The excess rate of mortality and morbidity from misadventures among older patients may suggest that this group is worthy of targeted research.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Not applicable
Guarantor
KK, PE and IR
Contributorship
KK and PE designed the study; KK obtained the data and conducted all analyses; KK and PE wrote the paper with input from IR; all authors interpreted the data and approved the final version of the paper
Acknowledgements
HES data 2009 are re-used with permission from the Health and Social Care Information Centre
Reviewer
Martin Bardlsey