
Abstract
Summary
Following the recent white paper – Equity and Excellence: Liberating the NHS – we need a 21st-century model of leadership in the NHS that re-focuses on the centrality of the relationship between clinicians and patients. This paper argues the case for co-productive ‘Health Leadership’ that can meet the challenges set by the current Big Society agenda, Darzi and Wanless, so that we achieve a sustainable, high quality NHS, fit for the 21st century.
Introduction: establishing common ground
The recent white paper 1 outlines the requirement for a patient-focused NHS; one that reflects individual's health and care needs; that is delivered mutually, and leads to better staff engagement and patient care.
This paper outlines a health leadership model that encompasses both a clinical and citizen/user perspective: one that sees health leadership as a co-production between health workers and patients working within and beyond traditional NHS boundaries.
We believe that real health improvement in the population as a whole will naturally arise from this way of working together. By linking sustainability (Wanless), quality (Darzi) and co-creativity we envisage a leadership model that embodies holistic health improvement, and is a new alternative to current public service models. 2
Wanless' fully engaged scenario, 3 now a necessity, requires the wider patient community to be enabled to play its part in achieving a safe and sustainable NHS for all citizens.
Healthcare needs to embrace a co-created model, with clinicians and patients working and learning together. ‘Engagement’, and its corollary ‘Empowerment’, can no longer remain as easily misunderstood rhetoric, or marginalized as a Patient and Public Involvement function: they are core to leadership success throughout health and social care.
Defining true engagement
Achieving a ‘portfolio’ of local services that provide safe, high quality support and care, while also reducing inequalities and improving health and quality of life outcomes, is a highly sophisticated task. This task requires health leaders to meaningfully and productively engage throughout the whole commissioning–delivery cycle.
HealthCare Commission, Review of NHS Performance on Patient and Public Engagement, March 2009
There is a fundamental requirement for a change in the relationship between clinicians and patients; they must both learn that effective healthcare is a joint endeavour: from diagnosis and clinical intervention, to supporting successful recovery and most importantly, sustainable, independent living. For too long this holistic approach has been given lip service by a profession that is still far too paternalistic and remains unchallenged by the majority of patients.
The Darzi Review demands a ‘clinically driven, patient-centred, and locally led’ approach to both commissioning and delivery. 5 Safety, quality and equity are the shared goals on all sides of a highly complex, dynamic system. Health leaders' decisions can make or break ‘quality’ and its contingent values, namely safety, equity and productivity.
Clarity about what is meant by ‘quality’ is lacking and interpreted differently by users, clinicians and managers. We believe ‘quality’ is an expression of public value that enriches people's lives and that, crucially, enhances where and how they live and work. In this sense it is the users of the service who should decide on what quality is and it is for this reason that user leadership is essential in this co-productive ‘Health Leadership’ model.
Wanless emphasized the sustainability of the NHS is dependent on improving health outcomes, through wider public engagement and enhanced service productivity. Leadership competencies required for this level of engagement go far beyond the silos of clinical or managerial leadership and require a far wider ‘Health Leadership’ approach.
Co-creative models have already emerged, mutually, through the development and implementation of the National Service Frameworks (NSFs) and more recently through true co-production, illustrated by project such as ‘Partners in Care’ from NHS Diabetes 6 involving clinicians and citizens as active partners. Local Health Watch groups outlined in the white paper will facilitate this approach going forward.
The clinician's challenge – from clinical leaders to health leaders
Government has acknowledged that the rising cost of healthcare is unsustainable. Wanless identified the requirement for a shift in emphasis from an illness service to a fully-engaged public health ‘wellness’ service 2 to enable an economically viable future NHS. Further underpinning this engagement agenda has been the recent drive to enable greater clinical leadership, enshrined in Lord Darzi's Next Stage Review. 7
So what are the issues clinicians must address in order to contribute to engaged leadership for a sustainable NHS and thus become true health leaders?
Clinicians need to embrace the change in patients' attitudes towards their healthcare delivery needs; from deference to the profession and gratitude towards the State to being less deferential, better informed (due to the information technology age), and rightly more demanding but no less trusting of the medical profession. 8
Many regular users feel the term ‘patient’ no longer feels appropriate and the profession's paternalistic approach of old is rightly being challenged. Fundamentally there is supporting evidence that demonstrates outcomes and compliance can be improved with patients taking control of their own healthcare needs. 9
‘Clinical leadership’ is the current mantra being championed with clinicians increasingly entrusted with crossing professional boundaries and delivering cost-effective personalized healthcare. However, clinicians are trained to be autonomous and, as a result of their own dedicated training, there is a danger that contributions from other health professionals, managers and users are at risk of being overlooked at best and discarded at worst. Clinicians must, therefore, learn and develop a more collaborative and sometimes less directive approach to leadership. Health leadership often requires a different approach to leading a clinical team.
Health leaders must address the issue of management speak in healthcare. When management
goals are expressly communicated appropriately as improvement to clinical services
(rather than in raw metrics) there is an improvement in clinical outcome and quality of
services ( Key characteristics of high performing teams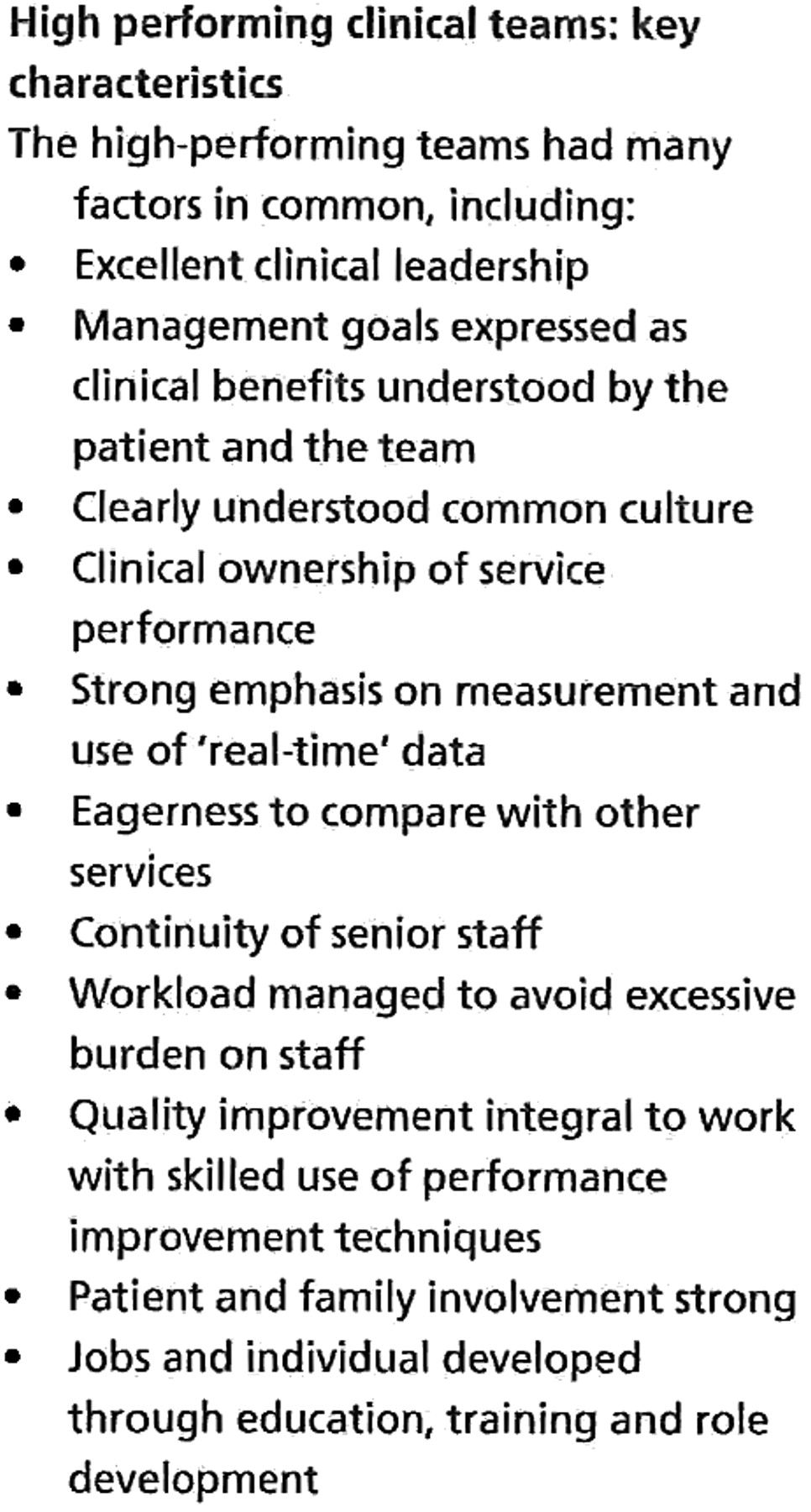
Clinicians, particularly those in specialist care, must take a more holistic approach to health, placing equal emphasis on wellbeing and public health as to curing and managing illness. Wanless' ‘fully engaged’ scenario should, therefore, apply to clinicians also. Without an appreciation of the broadest definition of health no clinician can be truly a healthcare leader.
The health leadership model
Within the current system we argue health delivery encompasses four domains: Clinical,
Managerial, User and Governmental ( The domains of health leadership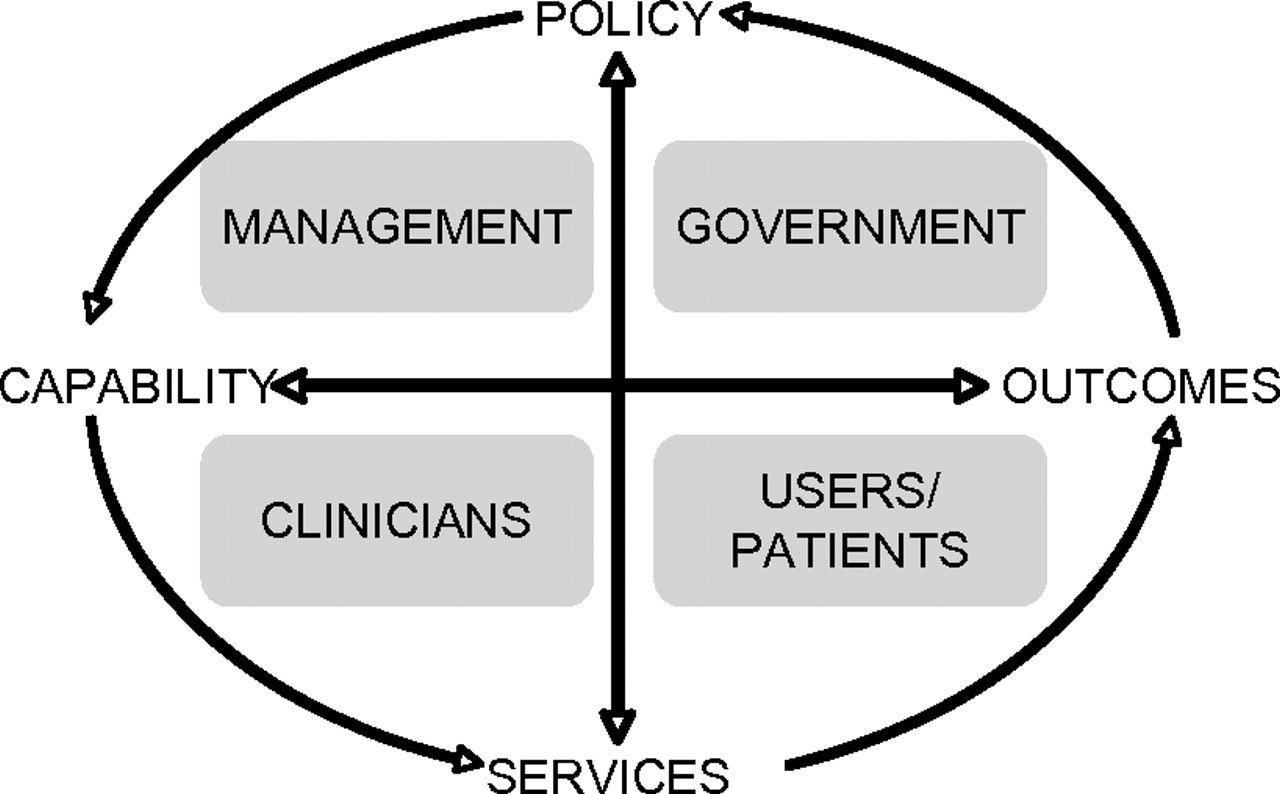
We believe that improvement should no longer be about doing better to and for others, it
should be a matter of co-production and mutual learning
10
– ‘nodecision about me, without me’.
1
Co-productive health leadership ( Health leadership: towards co-production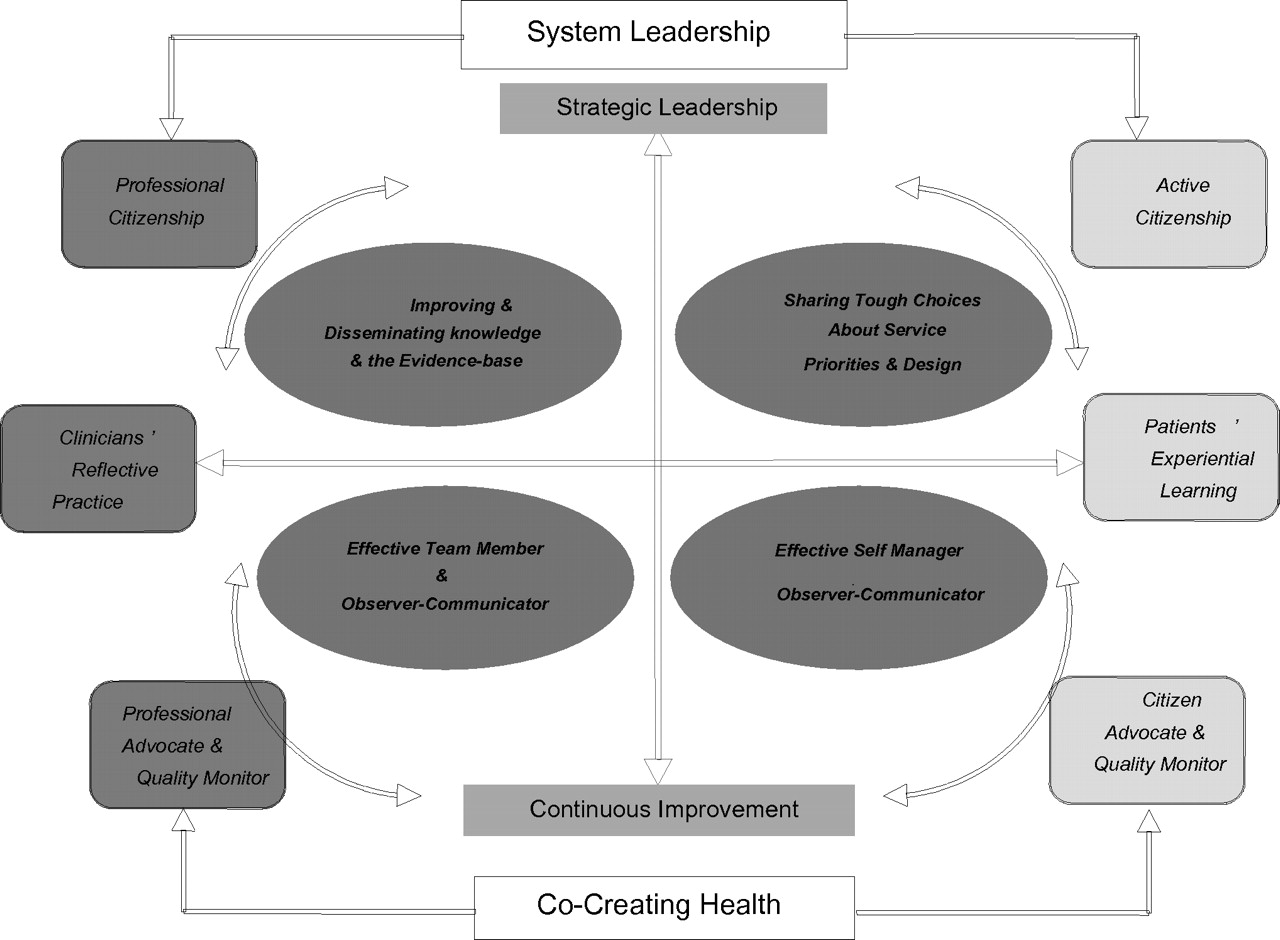
Conventional service development has been based on the integrated care pathway – a systematic and evidence-based design principle that ensures the highest possible standard of clinical outcome for people with specific medical conditions. However, the emphasis for people with longer-term conditions has moved towards more individualized ‘care planning’ model, whereby people with more complex needs have ownership of their individualized care plans and are able to choose support or treatment services, and fund them, according to their own preferences. As such leadership is required from the personal level to the ‘complex systems’ level.
Increasingly, leaders will be required to transcend traditional structures and processes. Health leaders – clinicians and citizens, commissioners and providers, will need to work much more closely together in flexible productive partnerships, sharing knowledge and experience, energy and enthusiasm, doubt and uncertainty.
This Health Leadership framework allows the NHS to become a system designed to promote health and wellbeing, supporting citizens, newly formed GP consortia commissioning services and providers, who are fully engaged. Co-designed services facilitate individual care planning, informed by the traditional medical model, accommodating individual needs, preferences and circumstances and enabling the NHS to improve: personally, locally and systemically.
While developing complementary advocacy and citizenship roles, we also create the potential for shared learning and mutual endeavour: both with regard to the strategic leadership now called for in service planning, design and commissioning, and in respect of catalysing continuous service improvement at the frontline. This model incorporates a grounded, iterative process of mutual engagement: professional experts and experts by experience.
Conclusion: from perspectives towards co-production
From a patient's perspective, the recent drive towards consumerism has profoundly unbalanced the system, especially at a day-to-day operational level. Patients have multiple roles and responsibilities, including self-management, active citizenship and community building. Most that use NHS services regularly live with long-term conditions and disabilities, and those who do not rely on the ever-present primary care and urgent response services. Individually and collectively we are learning to enter into constructive dialogues with clinicians: both about our own health, as well as the wider, long-term interests of the communities where we live. For us, ‘Health Leadership’ is about taking this dialogue forward on the basis of mature, informed and shared decision-making – an approach that goes well beyond ‘Choose and Book’, surveys and league tables. The government white paper goes a long way in setting this vision, it is now imperative for us to be invited to take, and subsequently rise to, this challenge.
Clinicians must acknowledge and embrace wider health leadership responsibility. They must be robust and collectively challenge when proposals do not enhance the central clinician–patient relationship, fighting for their patient's rights, with them, not acquiesce and blame the system. Clinicians must work collaboratively to develop a more co-productive, rewarding and cost-effective system.
Dr Colin-Thome's Mid-Staffordshire report recognized this and states ‘Patient empowerment is a theme throughout my review, and I hope my recommendations in relation to patient empowerment are taken to heart by the NHS … Patients must be involved in the design, delivery, and quality assurance of their services and … All clinicians must speak up for patients when they witness poor quality care. It is our overarching duty.’ 11
While no-one can guarantee protection against systemic failure, we believe that the longer-term solutions lie in changing the basis of the relationship between patients, clinicians and managers; by moving toward a system based on openness, informed dialogue and critical friendship. An NHS based on adult-to-adult relationships. These are the real choices that will determine the success and sustainability of the NHS. These are the key elements of co-productive ‘health leadership’ and these are the fundamental pillars that will determine the success of the ‘newly liberated’ NHS.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
The authors would like to acknowledge Simon Eaton, also a Health Foundation Leadership Fellow, for his help and advice on this manuscript. Professor Bob Sang sadly died prior to the publication of this article. He was a leading authority on patient advocacy and a ‘critical’ friend of those who worked in the National Health Service. As aservice user he constantly challenged the status quo and argued for a more equal relationship between patient and clinicians. This article is dedicated to him and the profound influence he had on making the voice of the user heard in the NHS