
Abstract
Summary
Objective
To examine the impact of the Quality and Outcomes Framework, a major pay-for-performance incentive introduced in the UK during 2004, on diabetes management in patients with and without co-morbidity.
Design
Cohort study comparing actual achievement of treatment targets in 2004 and 2005 with that predicted by the underlying (pre-intervention) trend in diabetes patients with and without co-morbid conditions.
Setting
A total of 422 general practices participating in the General Practice Research Database.
Main outcomes measures
Achievement of diabetes treatment targets for blood pressure (< 140/80 mm Hg), HbA1c (≤ 7.0%) and cholesterol (≤ 5 mmol/L).
Results
The percentage of diabetes patients with co-morbidity reaching blood pressure and cholesterol targets exceeded that predicted by the underlying trend during the first two years of pay for perfomance (by 3.1% [95% CI 1.1–5.1] for BP and 4.1% [95% CI 2.2–6.0] for cholesterol among patients with ≥ 5 co-morbidities in 2005). Similar improvements were evident in patients without co-morbidity, except for cholesterol control in 2004 (−0.2% [95% CI −1.7–1.4]). The percentage of patients meeting the HbA1c target in the first two years of this program was significantly lower than predicted by the underlying trend in all patients, with the greatest shortfall in patients without co-morbidity (3.8% [95% CI 2.6–5.0] lower in 2005). Patients with co-morbidity remained significantly more likely to meet treatment targets for cholesterol and HbA1c than those without after the introduction of pay for perfomance.
Conclusions
Diabetes patients with co-morbid conditions appear to have benefited more from this pay-for-performance program than those without co-morbidity.
Introduction
Improving the quality of care delivered to individuals with multiple medical conditions is an important priority for healthcare systems. 1 The prevalence of co-morbidity is high and set to increase, particularly in countries with ageing populations. 2, 3 A study conducted in general practices in Quebec, Canada found that the percentage of attending patients with more than one medical condition was 68%, 95%, and 99% among women and 72%, 89%, and 97% among men aged 18–44 years, 45–64 years and 65 years and older, respectively. 2 Patients with multiple conditions have lower health-related quality of life, are more likely to be admitted to hospital and account for a disproportionate share of healthcare expenditure. 4, 5, 6 For example, Wolff et al. found that annual Medicare expenditures increased from $211 among beneficiaries without a chronic condition to $13,973 among beneficiaries with four or more chronic conditions. 6
While the use of pay for perfomance as a quality improvement tool in healthcare is increasing, little is known about the impact of these programs on the quality of care delivered to patients with multiple conditions. Pay for perfomance could impact the quality of care delivered to this group of patients in several ways. First, the single disease focus of some programs may result in more fragmented care for individuals with multiple conditions, by undermining continuity of care and the ‘generalist’ model in primary care. 7 Conversely, patients with multiple conditions may benefit from pay-for-performance programs that incentivize improvements in quality across a number of conditions. Second, the quality standards in pay-for-performance programs, which are derived from clinical trials that often exclude patients with co-morbidities, may be too ambitious and encourage inappropriate care in patients with multiple conditions. 8 Finally, pay-for-performance programs may disadvantage patients with multiple conditions and complex healthcare needs if they encourage ‘cream-skimming’ by providers or result in a higher rate of exclusion from associated public reporting mechanisms. 9 For example, early evidence from a major pay-for-performance program in the UK suggests that exclusion rates from performance reporting are higher in stroke patients with co-morbid conditions than in those without. 10
We undertook a cohort study using the General Practice Research Database (GPRD) to examine the impact of a major pay-for-performance program introduced in the UK in 2004 on the quality of diabetes management in patients with and without co-morbid medical conditions. Diabetes was selected as our index condition because of its rapidly increasing prevalence, high levels of associated morbidity and well-established evidence base for preventative care. 11, 12
Methods
Pay for perfomance in UK primary care
The Quality and Outcomes Framework, a major pay-for-performance program, was introduced into UK primary care as part of a new General Practitioner contract in 2004. The Framework accounts for approximately one-quarter of general practice income. Between 2004 and 2006, the Framework consisted of 1050 points, 550 of which covered clinical care. Each point translated into £75 ($110) of income for the average general practice during the first year of the Framework but this increased to £120 ($170) in the second year. The 10 disease areas within the clinical care domain of the Framework during this period were diabetes (99 points), coronary heart disease (CHD) (121 points), hypertension (105 points), stroke (31 points), epilepsy (16 points), hypothyroidism (8 points), mental health (41 points), chronic obstructive pulmonary disease (COPD) (45 points), asthma (72 points) and cancer (12 points). Of the 99 points available for diabetes care during 2004–2006, 50 were allocated for the achievement of treatment targets (blood pressure [BP] ≤ 145/85 mm Hg, 17 points; HbA1c ≤ 7.4%, 16 points; HbA1c ≤ 10%, 11 points; cholesterol ≤ 5 mmol/l 6 points) and the remainder to the recording of process measures, including annual measurement of body mass index (3 points) and retinopathy screening (5 points).
We undertook a cohort study examining trends in achievement of treatment targets for diabetes between 1997 and 2005. To determine the impact of the pay-for-performance incentive on patients with and without co-morbidities we compared actual achievement of targets in 2004 and 2005 with that predicted by the underlying (pre-intervention) trend.
Setting and patients
The GPRD holds anonymized, longitudinal primary care records on approximately 5% of the population registered with a general practice in the UK. The accuracy and completeness of the data recorded in the GPRD have been documented previously and the database is used extensively for health service and epidemiological research. 13, 14 General practices participating in the GPRD serve a population that is representative of the UK. 14
We obtained an extract from the GPRD containing the medical records of all adult patients (≥ 18 years) with Type 1 or Type 2 diabetes with an episode of care between January 1990 and December 2005 in participating practices. Patients were identified using both diagnostic (C10) and management (66A) Read and OXMIS codes for diabetes mellitus. Read codes are the clinical classification system used in primary care in the UK; OXMIS codes were used in the past by some general practices but have now been replaced by Read codes. The analysis conducted for the present study is limited to those patients who were registered with participating practices between 1997 and 2005.
Study variables
Our main outcome measures were achievement of national targets for HbA1c (≤ 7.0%), blood pressure (<140/80 mm Hg) and total cholesterol (≤5 mmol/L or 193mg/dl). We employed more stringent targets for blood pressure and blood glucose than those used in the Framework in line with national guidelines in the UK and USA. 15, 16 We assessed achievement of the three targets using mean annual values where patients had more than one measurement in a year. We identified the following co-morbid conditions in patients in each year using Read and OXMIS codes: hypertension, atrial fibrillation, stroke, heart failure, CHD, asthma, depression, osteoporosis and COPD (six of these nine conditions were included in the Framework). We selected these conditions because they are common and usually managed in primary care. Some of these conditions are major causes of mortality and morbidity in people with diabetes (e.g. CHD), or may influence diabetes management and outcomes (e.g. depression).
We then grouped patients by the number of co-morbid conditions from 0 to 5 or greater. Covariates in our analysis were age, gender, socioeconomic status, duration of diabetes, body mass index (BMI), number of medications prescribed (0–3 or more antihypertensives for BP target; no diabetes medications, oral hypoglycaemic agent(s), insulin, oral hypoglycaemic agent(s) plus insulin for HbA1c target; any lipid lowering medication for cholesterol target), practice size and practice diabetes caseload. Socioeconomic status was assigned to each patient using the Index of Multiple Deprivation 2004 based on their general practice postcode. 17
Statistical analysis
The data have a three-level structure, with multiple measures per patient and patients ‘clustered’ within practices; patients treated by the same general practice are expected to be more similar in their outcomes than patients treated by different general practices. This was handled by constructing marginal models using Generalized Estimating Equations (GEEs) in SAS version 9.1. The first set of models used records for 1997–2003 (pre-QOF) to estimate the underlying time trends and thereby predict the achievement rates for the post-QOF years. Year was fitted as a linear term; for HbA1c, only the pre-QOF years 2000–2003 were used for extrapolation as it was only during this period that the linear trend was valid. Actual mean post-QOF (2004 and 2005) target achievement was then compared with these mean predicted rates using t tests.
The second set of models was developed to examine whether QOF attenuated or widened differences in achievement of targets in patients with and without co-morbidities. Records for 2003–2005 were used for these models, with 2003 taken as the baseline and year this time fitted as a categorical variable to allow for non-linear post-QOF trends. All covariates were entered at once (i.e. with no stepwise selection) in both sets of models with none removed, even though BMI was not significantly associated with any of the outcomes (P>0.1). Interactions between year and co-morbidity were included where P<0.05.
Results
We identified 154,945 adult patients with diabetes registered with 422 participating practices during the study period. The number of people with diabetes registered with participating practices increased from 49,970 in 1997 to 105,065 in 2005. In 2005, 17.3% of patients had no co-morbidities with 32.4%, 21.9%, 14.8%, 8.4% and 5.2% having one, two, three, four and five or more co-morbidities, respectively. Patients with co-morbid conditions were older than those without any co-morbid conditions, and women were more likely to have three or more co-morbid conditions than men (Table 1).
Process of care and prescribing
Measurement of blood pressure, blood glucose and cholesterol increased during the study period but varied significantly (p < 0.001) with number of co-morbidities present in 1997 and 2005 (Table 1). Patients with one co-morbidity were most likely to have all three risk factors measured in both years. Prescribing of medications for secondary prevention increased during the study period. Antihypertensive and lipid lowering medications were significantly (p < 0.001) more likely to be prescribed in patients with one or more co-morbidities than in those without any co-morbidities in both 1997 and 2005.
Achievement of treatment targets
Blood pressure
The introduction of pay for perfomance was associated with improved achievement of an established treatment target for blood pressure in 2004 and 2005 which was significantly greater (p < 0.001) than that predicted by the underlying trend based on 1997 to 2003 data (Table 2, Figure 1). The magnitude of improvement was similar in patients with and without co-morbidities in both years.
For the analysis using the 2003–2005 data, blood pressure target attainment and co-morbidity showed a J-shaped relation, with patients with 1–3 comorbidities having significantly lower attainment (OR compared with no co-morbidity = 0.72, CI 0.69–0.74 for one, 0.87, CI 0.84–0.91 for two, 0.92, CI 0.89–0.96 for three co-morbidities) and five or more co-morbidities having the highest attainment (OR compared with no co-morbidity = 1.36, CI 1.28–1.44). There was no significant change in these relations over the three years (p value for interaction with year = 0.126).
HbA1c
Characteristics of the sample by number of co-morbidities
Neighbourhood socioeconomic status (SES) based on the Index of Multiple Deprivation 2004; the higher the score the greater the level of deprivation
OHAs = oral hypoglycemic agents; AHT = antihypertensive medication; BMI = body mass index
P values were derived using the Chi-squared test
Performance (as % achieving the target) for 2004 and 2005 compared with predicted by number of co-morbidities
5 mmol/L=193 mg/dL
HbA1c predicted figures were based on extrapolations from the period 2000–2003 only
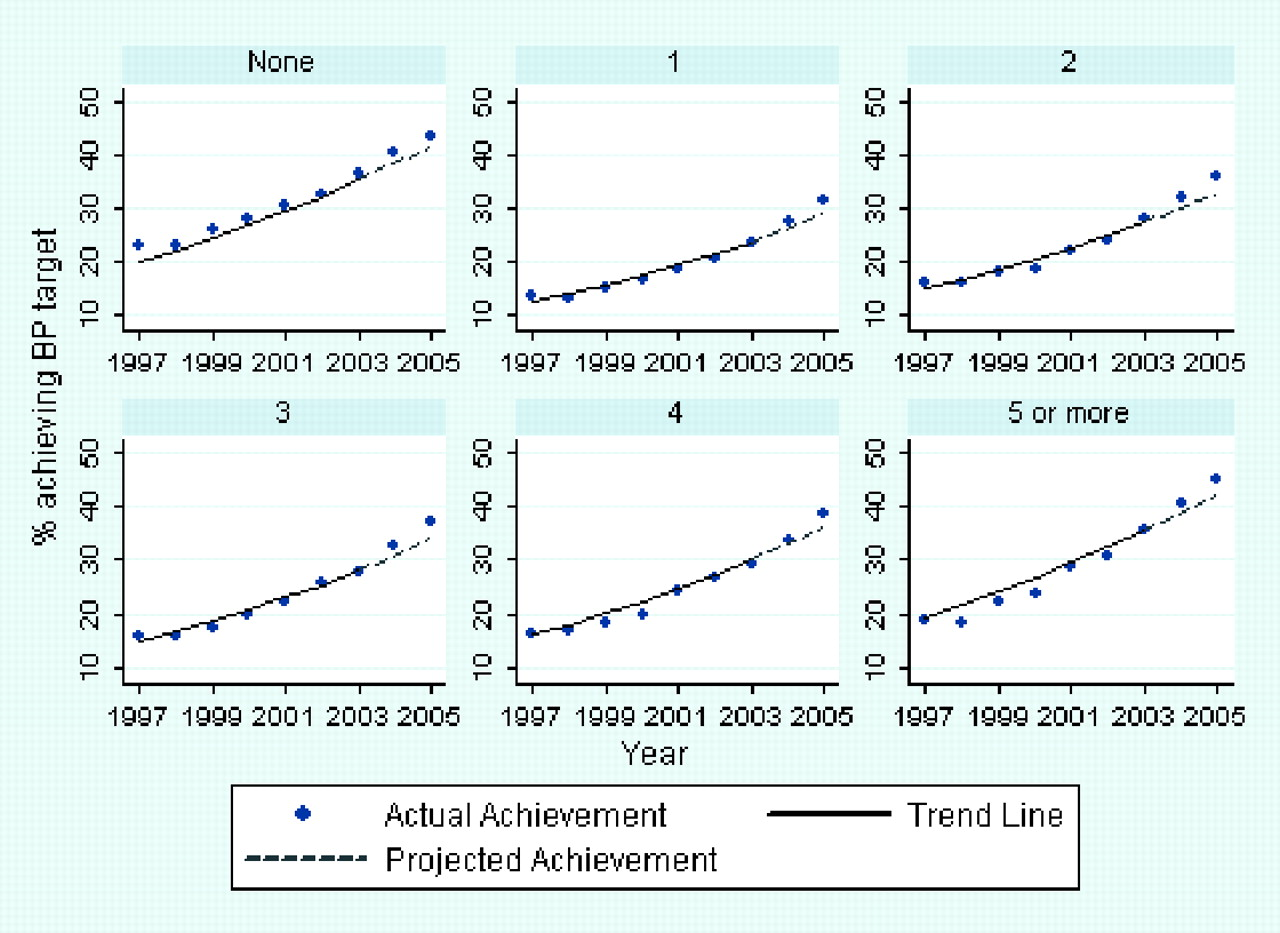
Projected and actual achievement of blood pressure target (<140/80 mmHg) by number of co-morbid conditions
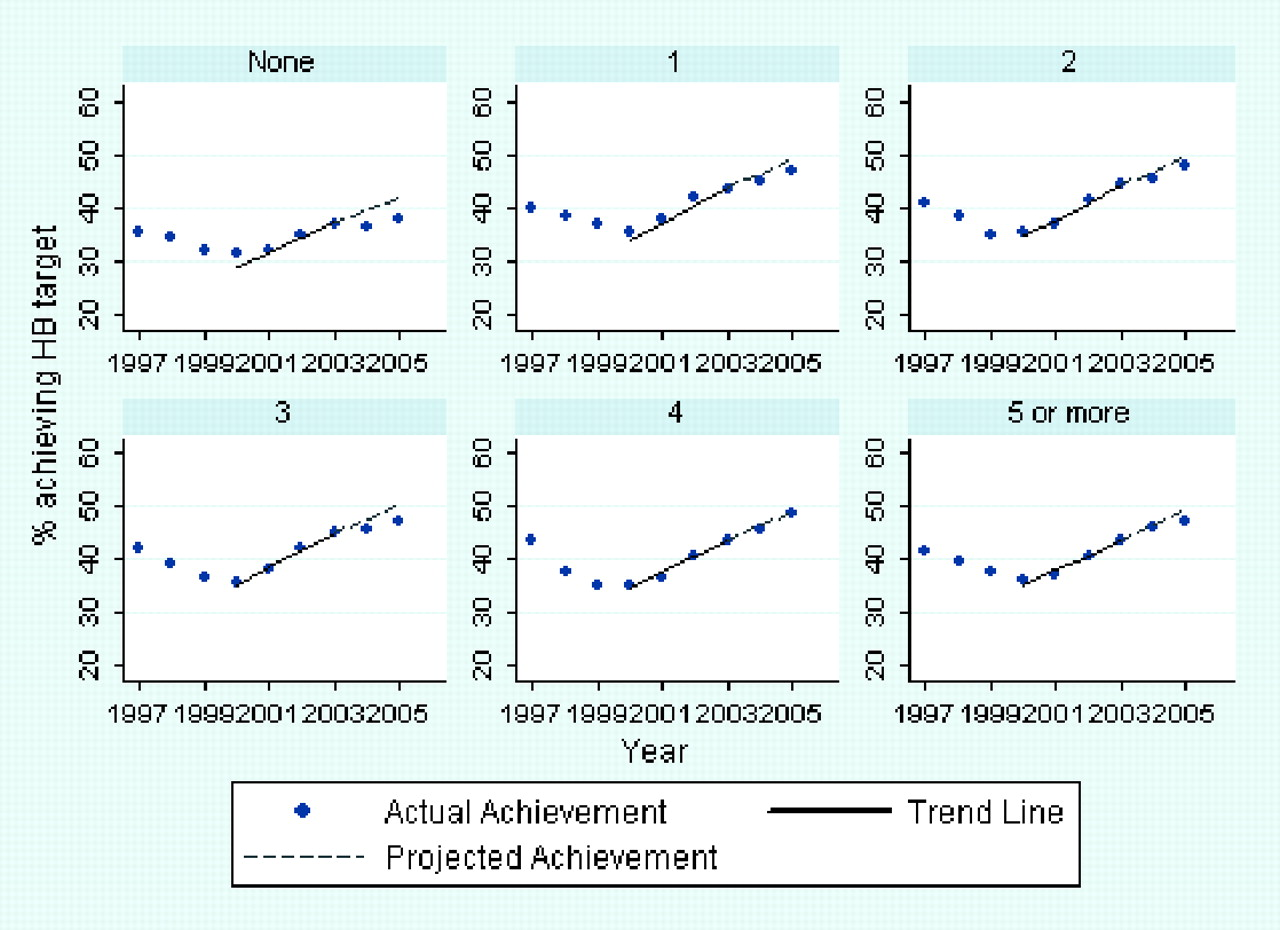
Projected and actual achievement of HbA1c target (≤7.0%) by number of co-morbid conditions
Total cholesterol
The introduction of pay for perfomance was associated with improved achievement of an established treatment target for total cholesterol in 2004 and 2005 (Table 2, Figure 3). These improvements were significantly greater than that predicted by the underlying trend based on 1997 to 2003 data in patients with co-morbidities. The improvement in cholesterol control did not exceed achievement predicted by the underlying trend in patients without any co-morbidity in 2004 (p=0.42) but did so by 1.4% in 2005 (p=0.029). For the analysis using the 2003–2005 data, in each year, cholesterol target attainment increased steadily with increasing co-morbidity. There was a significant interaction between year and co-morbidity (P = 0.0001), although the gap between 0 and 5 or more co-morbidities did not change across the three years: in 2003, the odds ratio for 5 or more co-morbidities compared with none was 1.87 (95% CI 1.69–2.08); in 2004, this was 1.96 (CI 1.78–2.16) and in 2005 it was 1.84 (CI 1.66–2.03).
Discussion
Principal findings
Diabetes patients with co-morbid conditions appear to have benefited more from the introduction of a major pay-for-performance program in the UK than those without co-morbidity. This meant that the superior cholesterol and HbA1c control evident in this group of patients before the introduction of the Quality and Outcomes Framework was maintained after its introduction.
Previous research
Our findings confirm those of a previous study which suggest that the introduction of the Quality and Outcomes Framework was associated with a step change improvement in diabetes management in the UK. 18 However, few studies have evaluated the impact of pay for perfomance on the quality of care provided to patients with co-morbidity. Whyte et al. found that the quality of diabetes care was similar in patients with and without a severe mental illness in the first year of the Quality and Outcomes Framework. 19 We have previously shown that hypertensive patients with co-morbidities had significantly better blood pressure control than those without co-morbidity after the introduction of this pay-for-perfomance program, although this benefit did not extend to black and south Asian groups. 20
Improvements seen in diabetes control in patients with co-morbid conditions after the
introduction of pay for perfomance may be due to several factors. First, the
programme incentivizes the maintenance of chronic disease registers and a systematic
approach to the management of risk factors. Patients with multiple conditions may
receive a greater number of clinic invitations, have more frequent attendance and
enhanced management as they will be on multiple disease registers. Six of the nine
co-morbid conditions examined in this study (stroke, CHD, hypertension, asthma,
depression and COPD) were included in QOF during 2004–2006. Second, the reward
structure of the programme means that it is highly beneficial for practitioners to
improve care and control risk factors in patients with several incentivized
conditions. For example, achieving good blood pressure control in one patient may
contribute to the achievement of treatment targets for hypertension, diabetes and
CHD. Finally, patients with multiple conditions may be more receptive to the
intensification of disease management incentivized by this pay-for-perfomance program
and may be more compliant with associated changes in drug regimens. While we
identified a step change improvement in blood pressure and cholesterol control
associated with pay for perfomance this was not the case for HbA1c in both patients
with and without co-morbidity. Projected and actual achievement of cholesterol target (≤5 mmol/L) by number
of co-morbid conditions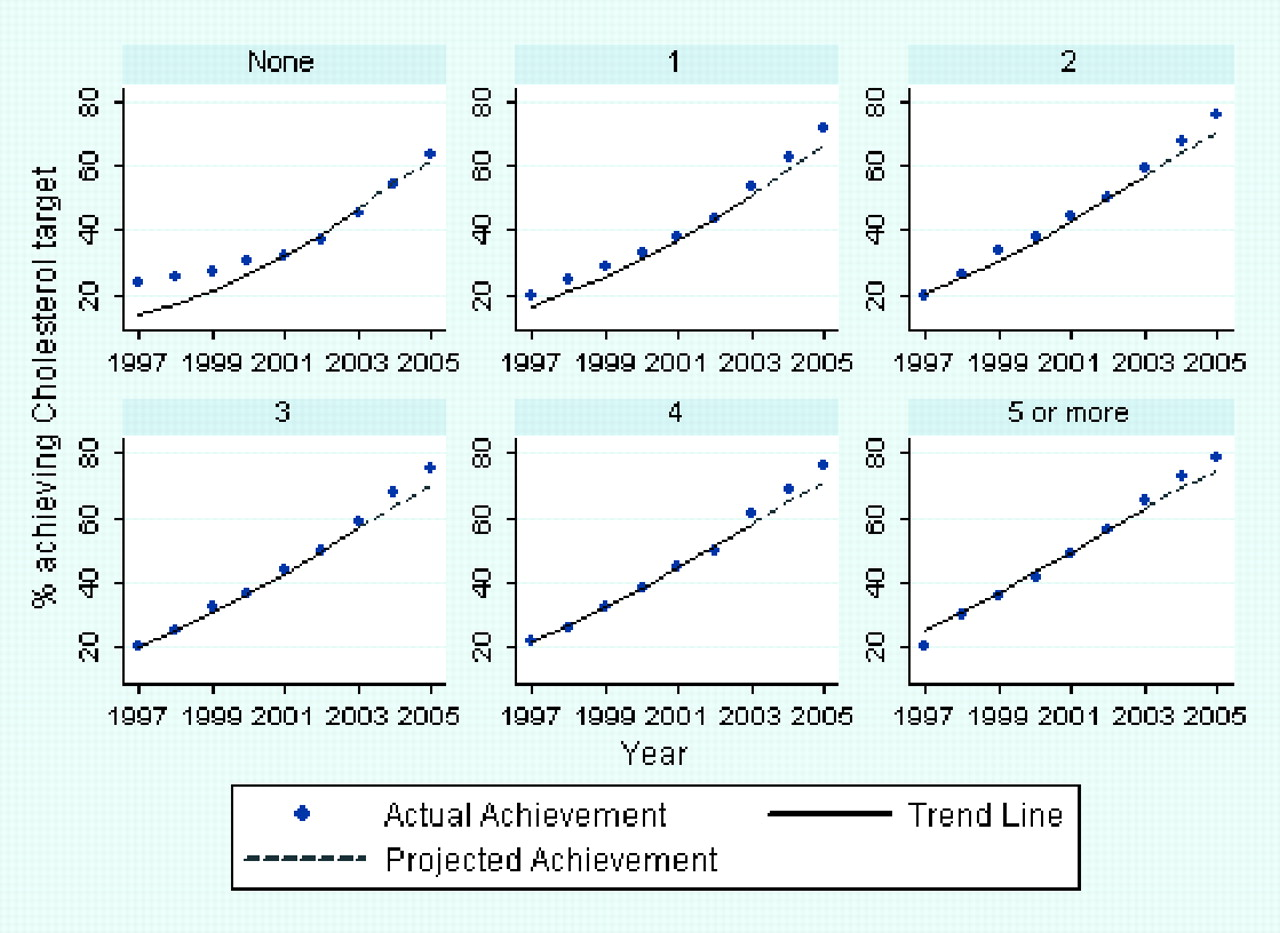
Strengths and weaknesses of the study
Our study has a number of strengths and limitations. Our findings are based on a large and representative sample of people with diabetes in the UK. Patients were identified from electronic records using diagnostic and diabetes care codes. The increase in the number of diabetes cases between 1997 and 2005 reflects an increased prevalence of this condition over this period and is consistent with findings from national survey data. 25 Further, achievements of national treatment targets seen after the introduction of this pay-for-performance incentive are broadly consistent with previous studies. 26 Data held in the GPRD are subject to rigorous quality checks. However, there may still have been some variability in the completeness and accuracy of the information used in our study. Our findings may have been influenced by any systematic differences in patients registered with practices in the different years of the study. However, we adjusted for several characteristics which may have varied over the study period, including age, BMI, duration of diabetes and socioeconomic status. There is lack of data on ethnicity in GPRD; although recording rates are now improving due to recently introduced pay incentives. There remains a lack of consensus around how to best define and assess co-morbid disease burden. 27 We opted to use a straightforward count of the number of conditions in each patient. The list of conditions used was not exhaustive but covered those which are commonly managed in primary care settings in the UK, including CHD, hypertension, depression and osteoporosis. We accept that this approach does not take into account disease severity or distinguish between concordant or discordant co-morbid conditions, i.e. those whose management and treatment goals may be consistent or inconsistent with those for diabetes. 28
Implications for policy
Our findings suggest that introduction of this major pay-for-performance program has not had a negative impact on the quality of care delivered to patients with multiple medical conditions. Rather, patients with co-morbid medical conditions seem to have benefited more than those without co-morbidity. This is reassuring given that previous studies have found that patients with multiple medical conditions are more likely to be excluded from performance reporting for this program. 10 Our findings provide no support for setting lower treatment targets for patients with multiple conditions within quality improvement programs and pay-for-performance schemes. 1 This is important given that the longer-term benefits of good diabetes control are now firmly established. 11, 12 and that associated health gain may be greatest in high-risk groups with existing co-morbid conditions such as CHD and hypertension.
Given that the Quality and Outcomes Framework incentivizes improvement across a number of the conditions examined in our study, the positive impacts on patients with co-morbidities seen here may not apply to programs which focus on a single or a small number of conditions. The study took place within the UK National Health Service, which provides universal access, free at the point of care, including free prescription medications for people with diabetes. This lack of any financial barriers to healthcare may have contributed towards the positive association between presence of co-morbidity in people with diabetes and quality of care. This may not be true in the US and in other countries with more market-based systems of healthcare. Hence, while previous US studies have found that individuals with multiple conditions receive similar standards of care to those with a single condition 29, 30 the impact of pay-for-performance programs on the care provided to these patients within market-based health settings merits careful evaluation.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
This study is based in part on data from the Full Feature General Practice Research Database (GPRD) obtained under license from the UK Medicines and Healthcare Products Regulatory Agency (MHRA). Access to the GPRD database was funded through the UK Medical Research Council'slicense agreement with MHRA. The Department of Primary Care & Social Medicine at Imperial College is grateful for the support from the National Institute for Health Research Biomedical Research Centre Scheme and the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care Scheme