
Abstract
Summary
Objectives
To assess changes in senior management culture in English NHS hospitals between 2001 and 2008.
Design
Longitudinal study comprising cross-sectional surveys of board levels managers at three time-points using a validated culture measurement instrument – the Competing Values Framework.
Setting
English NHS hospital trusts.
Main outcomes
There has been a decline in ‘Clan’ and an increase in more competitive ‘Rational’ cultures among senior management teams in NHS hospital trusts during the period 2001–2008.
Conclusions
Government policy for the NHS has espoused the desirability of competition, particularly since 2002. Our data suggest that corresponding changes in the cultures of senior management teams in NHS hospital trusts is beginning to occur, with the expectation that these organizations will pursue more competitive strategies.
Introduction
The notion of ‘organizational culture’ became prominent in the management literature of the 1980s 1 and has increasingly found its way into the discourse of those who advocate organizational change in health systems, including the British National Health Service (NHS). 2 Academic analysts generally agree that culture signifies something which is shared between an organization's members, for example: the prevailing beliefs, values, assumptions and attitudes, and from these the local norms of behaviour. These shared ways of thinking and behaving help to define what is legitimate and acceptable within an organization. They are the social and normative ‘glue’ that bind people in collective enterprise; or ‘the way things are done around here’ and help guide the discretionary behaviour of professionals and underpin management strategy and practice.
A diverse range of conceptual frameworks and models for understanding organizational
culture and culture change have been developed. This diversity reflects a lack of
theoretical consensus surrounding both definitions of organizational culture and the
processes of organizational change.
3
Perhaps the most critical cleavage in contemporary The Competing Values Framework for modelling organizational culture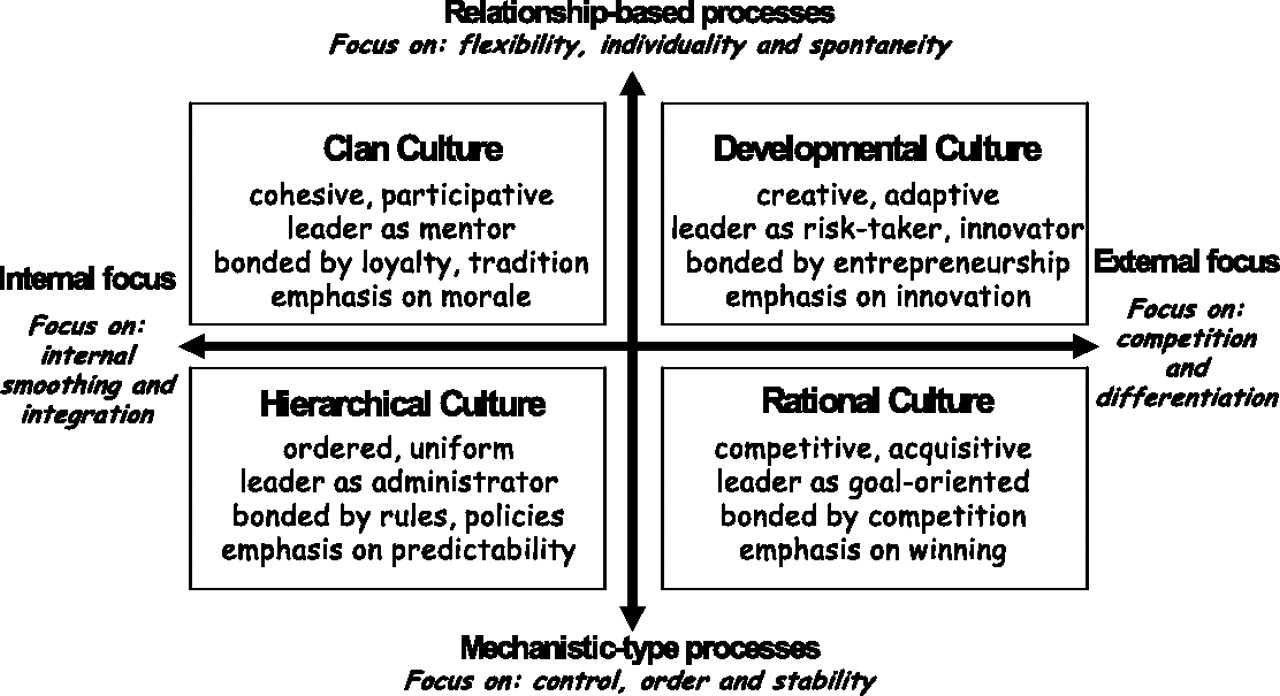
Appeals for ‘culture change’ imply that deep‐rooted changes in the kinds of characteristics listed above will lead to new patterns of behaviour and hence performance. It is unsurprising therefore that such change has been seen as a possible route to system‐wide performance improvement in healthcare. 5, 6 Over recent years NHS reforms in England have been based on the idea that major cultural change must be secured alongside structural and procedural change if the desired improvements in performance are to be achieved, with the National Patient Safety Agency the Healthcare Commission, and the Clinical Governance support team all prescribing culture change and transformation as a lever for quality and safety improvement. 7 Recent NHS system reforms have focused on the implementation of pro‐market policies, including an expanded role for patient choice, 8 competition between providers and a new prospective Payment by Results funding system for hospital Trusts. 9 In this context, a ‘market‐oriented culture’ 10 is officially seen as a prerequisite for successful healthcare providers.
In this paper, we examine how senior management culture within English NHS acute hospital Trusts has changed since 2001; that is, we explore cultural change over the period where official policy has revived ideas about hospital competition. To assess changes in senior management cultures we used a validated culture measurement tool, the Competing Values Framework (CVF), 11 which has been employed to analyse a number of health systems. 12 The CVF uses two main dimensions in order to generate a two‐by‐two matrix that articulates four basic organizational cultural ‘types’ (Figure 1). The vertical axis denotes how flexibly or mechanistically processes are carried out within the organization, while the horizontal axis denotes the orientation of the organization to the outside world. The values denoted by CVF ‘compete’ in the sense that scores in one direction on an axis are allocated at the expense of scores in the other direction. Nevertheless, organizations are not deemed simply to fall into one of the four cells in Figure 1. Rather, they are seen to exhibit competing values while nevertheless having a more‐or‐less strong tendency to one particular ‘dominant’ culture type.
Methods
We assessed senior management team cultures in NHS hospitals by means of a national
longitudinal study in the English NHS between 2001 and 2008, comprising cross-sectional
surveys of board level managers undertaken at three time-points: 2001–2002 (T1) with responses from 899 managers from 187 hospital Trusts; 2006–2007 (T2) with responses from 826 managers from 143 hospital Trusts; 2007–2008 (T3) with responses from 739 managers from 140 hospital Trusts.
(The diminution in the number of hospital organizations in the sample largely reflected merger of organizations over this period.)
For T1, out of a total of 2244 questionnaires sent out (12 per trust) a response rate of 40% was recorded. The same number of respondents (12) were targeted for both T2 and T3, corresponding to a total of 1716 and 1680 and yielding a response rate of 48% and 44%, respectively.
Frequency distribution of dominant culture by Trusts, weighted for number of
respondents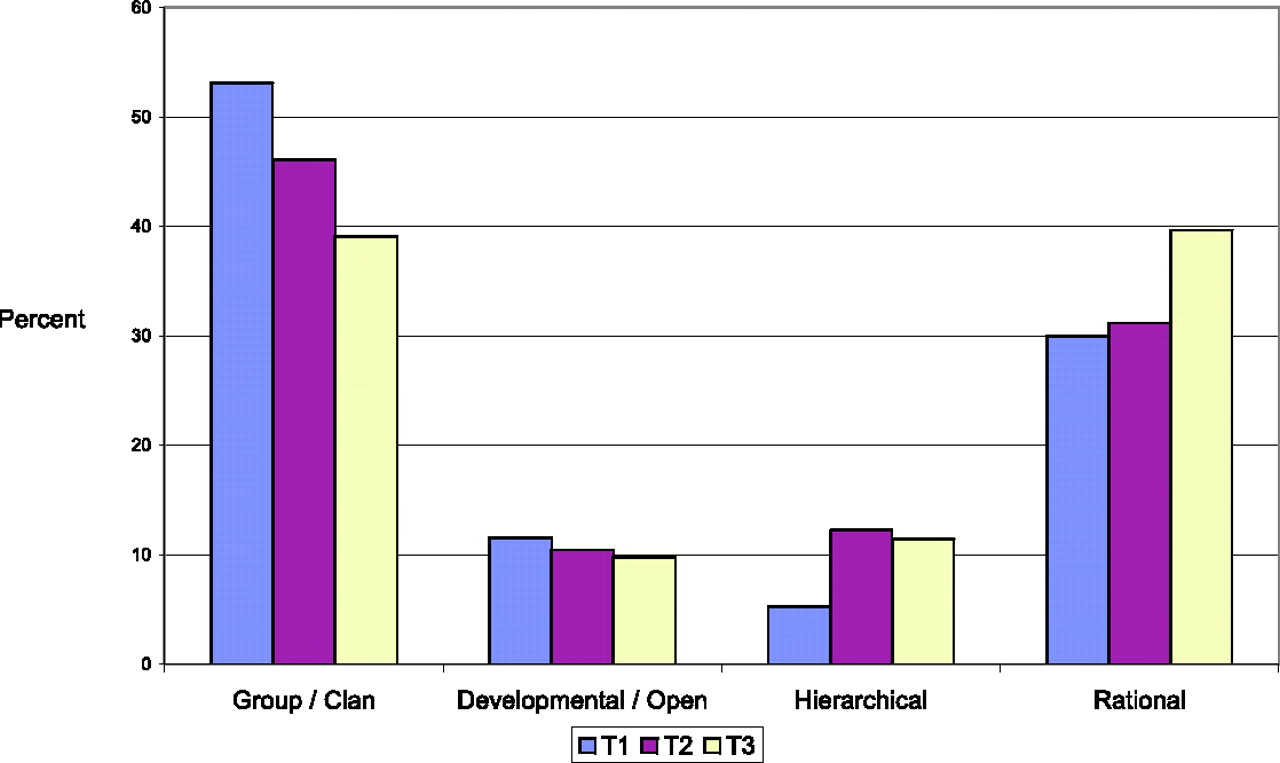
The cultural type with the largest score from a respondent defines that individual's perception of the organization's dominant culture type; the actual value represents the ‘strength’ of that dominant cultural type. Scores on each axis of the matrix, along with dominant culture type and strength were calculated by aggregating across the individual scores of the senior management team (executive board) of each organization. Both the originators of CVF and other users of the instrument have taken the view that three or four responses from senior managers in a particular organization are sufficient validly to describe its culture in these terms. 14 We tested for the appropriateness of aggregation using interclass correlations and ANOVA and found acceptable levels of agreement. Results as reported below were weighted by the number of respondents per organization, though this made little difference from unweighted scores (analyses weighted by respondents job type also gave very similar results).
Results
We attained excellent national coverage of the English acute hospital sector. At the first time‐point (T1) at least three senior managers responded from 170 organizations (86% of those surveyed), and four or more replied from 145 (74%). At the second wave data collection (T2), at least three responses were received from 95% of the organizations surveyed and 89% provided four or more respondents. The corresponding figures for the final data gathering (T3) were 93% and 89%.
Figure 2 summarizes our findings in terms of the hospitals' dominant culture type as reported by senior managers at the three time‐points. Over the five‐year period between 2001–2002 and 2006–2007, ‘Clan’ remained the most dominant type of senior management team culture (53% and 46%, respectively), although its prevalence was in decline with a corresponding large rise in ‘Hierarchical’ cultures from 2001 (4%) to 2006–2007 (13%). Over the same period so‐called ‘Rational’ cultures accounted for a roughly consistent proportion of hospitals (30% and 31%, respectively). The proportion of ‘Developmental’ cultures also remained relatively constant.
However, one year later in 2007–2008 dominant ‘Rational’ culture had overtaken ‘Clan’ to become the most frequently reported dominant culture type (40% or Trusts; representing a 34% increase). These changes were matched by corresponding falls in the frequency of ‘Clan’ as dominant culture to 39%; and, to a lesser extent, ‘Developmental’ (down from 10% to 9%). The mean strength of the dominant culture (as defined above) also declined slightly over the study period from 36.6 to 33.8.
Discussion
The continued prominence of ‘Clan’ as the dominant culture from 2001–2002 (53%) to 2007–2008 (39%) is broadly consistent with the findings of qualitative empirical studies of NHS organizations over a long period 15 and is likely to be related to the degree of autonomy typically associated with professional work in formal organizations. 16 The rise in frequency of ‘Hierarchical’ as a dominant culture is consonant with contemporary commentary on the increasing manifestation in the NHS of bureaucratic rules (such as clinical guidelines and protocols, National Service Frameworks and other aspects of the current audit and inspection regime) over this period. 17, 18
The appearance of competitive ‘Rational’ dominant cultures as the most frequent type in 2007–2008 is also consistent with an NHS policy context in which such developments as ‘payment‐by‐results’ of hospitals, 9 practice‐based commissioning 19 and greater involvement of private sector providers 20 have become increasingly prominent. The inclusion of the word ‘competing’ in the title of our culture assessment tool (the CVF) reminds us that these shifts in dominant cultures do not imply that the characteristics of other culture types are suddenly absent from the hospitals studied; indeed, the slight decline in strength of prevailing dominant cultures reinforces point that even dominant cultures ‘compete’ with other values.
Government policy for the NHS has espoused the desirability of competition since the late 1980s, albeit with something of a respite between 1997 and 2002. Our data suggest that corresponding changes in the cultures of NHS hospitals, as reported by their senior managers, are finally beginning to occur, a conclusion that is consistent with the findings of international comparative research that associates differences in hospital culture with differences in countries' political economy. 12
Conclusions
Although we have collected CVF data (not reported here) in respect of less senior managers for 2006–2007 and 2007–2008 (which revealed similar findings), we have no comparable data at this level for 2001–2002. However, there are good theoretical and empirical reasons to expect that changes in senior managers' reports of their hospitals' dominant culture will have a substantive impact. First, the institutional economics literature suggests that the cultural contexts within which senior managers work do affect their motivations and behaviour. 21 In the context of NHS hospitals, this implies that senior managers espousing ‘Rational’ organizational culture will act in ways that affect the way in which subordinates construe their work and the way in which this relates to the hospital's performance. Second, our earlier work with 2001–2002 CVF data has confirmed that there are logical relationships between the dominant cultures of hospitals and their organizations' approach to defining and pursuing ‘performance’.22
In summary, we would expect NHS hospitals increasingly to adopt the kinds of ‘Rational’ strategy implied by Figure 1; that is, to focus on gaining resources by winning market share, and to use the existence of competition as the means of integrating work within the hospital. This will necessarily influence the environment and incentives within which health professionals work and future research is required to assess how these cultural changes will impact on professional behaviour (for good or ill), patient experience and clinical outcomes. Notwithstanding the idiosyncrasies of the English NHS and the implications of these for generalizing to other healthcare contexts, we might expect similar cultural changes in other health systems attempting to implement pro‐market reforms.
It is not our objective here to arrive at a normative position about these developments. ‘Clan’, ‘Hierarchical’ and ‘Rational’ organizational cultures in the public sector all have their proponents and critics. Rather, we seek to stress that real changes in the dominant cultures of English NHS hospitals are occurring and that these are in turn likely to make these organizations pursue more competitive strategies.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
We would like to thank Jeffrey Braithwaite for his useful comments on an earlier draft of this article