
Abstract
Summary
Objectives
A shortfall exists of female doctors in senior academic posts in the United Kingdom. Career progression depends on measures of esteem, including publication in prestigious journals. This study investigates gender differences in first and senior authorship in six peer-reviewed British journals and factors that are associated with publication rates.
Design and main outcome measures
Data was collected on United Kingdom first and senior authors who had published in the British Medical Journal, Lancet, British Journal of Surgery, Gut, British Journal of Obstetrics and Gynaecology and the Archives of Diseases in Childhood. Authorship and gender were quantified for 1970, 1980, 1990, 2000 and 2004 (n=6457). In addition, selected questions from the Athena Survey of Science Engineering and Technology (ASSET2006), web-based doctor's self-report of publications were also analysed (n=1162).
Results
Female first authors increased from 10.5% in 1970 to 36.5% in 2004 (p<0.001) while female senior authors only increased from 12.3% to 16.5% (p=0.046). Within individual journals, the largest rise was in British Journal of Obstetric and Gynaecology with 4.5- and 3-fold increases for first and senior authors, respectively. In contrast, female senior authors marginally declined in Gut and Lancet by 2.8% and 2.2%, respectively. ASSET2006 identified that female respondents who were parents were less likely to have publications as sole (p=0.02) and joint authors (p<0.001) compared to male respondents. Female respondents with care responsibilities for parents/partner also had less publications as lead authors compared to those without carer responsibilities (p<0.001).
Conclusion
The increase in UK female first authors is encouraging. In contrast, there is considerable lag and in some specialties a decline in female senior authors. Factors that could narrow the gender gap in authorship should be sought and addressed.
Introduction
The number of female medical students in the United Kingdom has gradually risen over the
years. Women now represent 59% of the yearly intake in contrast to 32% in 1977.
1,
2
Percentage of women in medical schools in the UK in 1977–2006. Percentages
plotted in this figure are based on HEFCE data and previously published census
data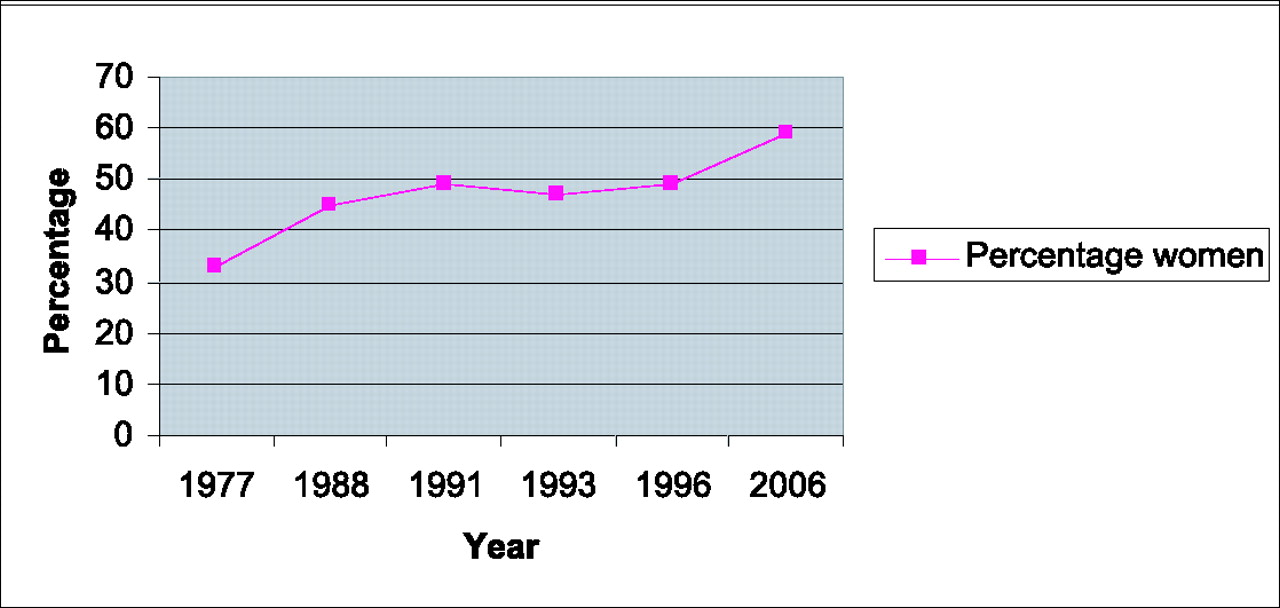
Despite this encouraging increase, there is considerable evidence that women continue to be under-represented in academic medicine and higher academic posts. The United Kingdom (UK) Council of Heads of Medical Schools (CHMS) annual census has shown that in 2006, female doctors only accounted for 11% of all professorships and only 36% of clinical lecturers' posts. This census revealed evidence of a decline in the number of women represented at each step of the academic career ladder and also showed that the ratio of women to men at each grade (from lecturer to senior lecturer to professor) has failed to improve over the years. 6 A qualitative survey carried out by the Medical Schools Council Working Group on senior clinical academics who graduated in the 1970s also found that women made career choices and entered academic medicine somewhat later than men. 6 In the USA, studies have shown consistently that women are less likely to achieve academic promotions than their male faculty members (with similar durations of faculty appointments). 7
The career pathways of women are often affected by family life, for example, maternity leave and flexible training for child care. 8 A female doctor's career, as distinct from her male equivalent, has been described as an M shape with two peaks, one in the early years and a potential rise in the later years when time required for childcare may be less demanding. 9 These time-related gender differences in career progression may hinder promotion for women as highlighted by the United Kingdom National Institute of Economic and Social Research in 2005. 8
Within the UK, the current Research Assessment Exercise (RAE) 2008 has been introduced by the government to alter the way funding is distributed and to potentially have a positive impact on the quality and competitiveness of research. 10 However, the Research Assessment Exercise 2008 also includes an update to ensure gender and employment equality are complied with, in preparing and selecting staff for RAE submission. 11 This is in accordance with the new UK legislation of Gender Equality Duty for England that was implemented in April 2007.
Although these UK-based surveys indicate that there may be a gender imbalance in academic medicine, this has never been quantified in the UK, using a surrogate marker such as authorship of scientific publications (unlike in the USA). 12 Our aim was to determine if there were gender differences in first and senior authorship in six peer-reviewed British journals and using a web-based questionnaire to assess which factors may affect publication rates. 13
Methods
Publication rates
Six prominent medical journals published in the UK were selected. They were the British Medical Journal (BMJ), Lancet, British Journal of Surgery, Gut, British Journal of Obstetrics and Gynaecology (BJOG) and the Archives of Disease in Childhood. We considered that these journals provided an appropriate representation of both high impact, general and specialist journals.
We did not specifically choose a general practice journal. As the British Journal of General Practice has only been published since 1990, it would have been difficult to make comparisons with other journals. In addition, we felt that some inferred observations could be made (about general practice) by selecting the BMJ as one of our core journals because the BMJ is focused on both primary and secondary care.
Overall UK female representation in the six journals from 1970–2004 (%)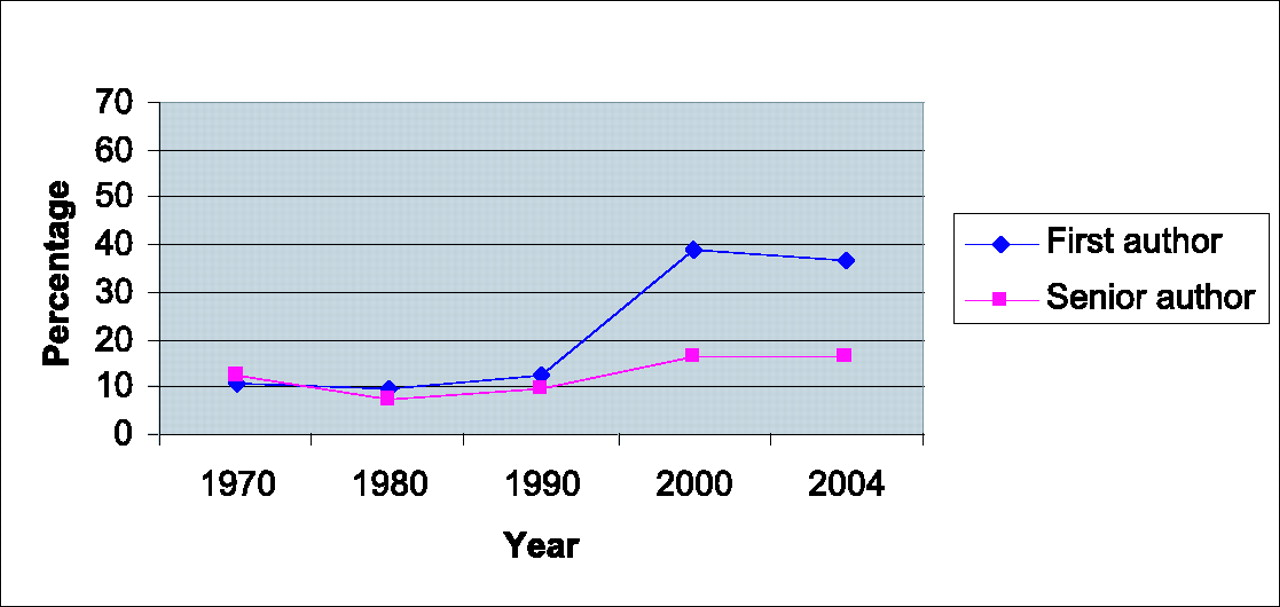
We attributed the last author as having senior author status. This is widely accepted academic practice. However in order to be certain, as some practices may vary, we also studied manuscripts to assess for a statement of authorship within the contributor list and where necessary we contacted the authors individually or via the institution for clarification.
On-line survey
Recently the Athena Survey of Science Engineering and Technology (ASSET2006) was conducted. This was a web-based self-selected on-line questionnaire. Related to Athena Survey of Science Engineering and Technology is the Women in Academic Medicine project. 14 This project identified individuals within the ASSET survey who were male and female medical doctors working in UK healthcare. 13 The respondents were self-selected and came from both healthcare and higher education divisions. One aspect of this survey included doctors' self-report of peer-reviewed research publications as ‘sole’, ‘joint’ and ‘lead’ authors in the past three years and factors which may have affected publication rates. We obtained collaborative permission from Athena Survey of Science Engineering and Technology to analyse novel data on gender differences in publications. From this web-based questionnaire responses to selected questions on frequency of publications and care responsibilities as a parent or for a partner/parent were measured.
The data was analysed using Statistical Package for Social Sciences (SPSS) version 13.0 and the University of Sheffield statistics department was consulted. Chi squared tests were used to analyse differences between gender groups.
Results
Publication rates
We assessed 6457 original articles for country of origin and gender over the five study years from 1970 to 2004. Fifty-two percent of publications originated from the UK in the six journals. The author's gender was successfully determined in 94% of the articles. The percentage of female first authors overall in all six journals increased from 10.5% in 1970 to 36.7% in 2004 (p<0.001, OR 4.9, 95% CI 3.7–6.6) while senior female authors represented 12.3% of authorship in 1970 compared to 16.5% in 2004 (p=0.046, OR 1.4, 95% CI 1.0–2.0). The trend of UK first and senior authors over the studied years is shown in Figure 2.
Representation of women among first and senior authors of published original research in the UK: number/total number of authors (%)
BMJ=British Medical Journal; BJS=British Journal of Surgery; BJOG=British Journal of Obstetrics and Gynaecology; ADC=Archives of Diseases in Childhood
On-line survey
The Women in Academic Medicine cohort of Athena Survey of Science Engineering and Technology (ASSET2006) had 1162 respondents (73% female doctors, 27% male doctors in clinical medicine) of which 53% comprised of doctors in the National Health Service, 38% within universities and 9% who were in other sectors or on a career break. Both men and women in universities and women in the National Health Service rated research publications as the most important factor contributing to successful career progression within their current employment. 15 Female respondents who were parents (n=511/851) were less likely to have one or more publications as sole (p=0.02) or joint authors (p=0.001) compared to male respondents (n=244/311). However being a parent did not have a significant impact on publication rates as lead author between the two genders (p=0.26). Female respondents who had care responsibilities for parents/partner (n=114/819) were also less likely to have publications as lead authors compared to those females without carer responsibilities (p<0.001). There was no significant difference in publication rates as lead authors between male and female respondents who were carers, (p=0.126), however the number of male respondents in this group was small (21/311).
Discussion
This is the first study to determine gender authorship of academic medical literature as a surrogate marker of gender imbalance within the UK. Our data are encouraging as first authors who were female have increased 3-fold from 10.5% in 1970 to 36.7% in 2004. The rise in female authorship was particularly notable at the turn of the 21st century however this momentum may be reaching a plateau. This rise has also been in conjunction with the increase in the number of women entering medical school (Figure 1). When compared to the medical workforce, 9% of doctors first appointed to consultant/attending posts in 1962–1976 were women, as were 30% of consultants who were first appointed in 1997–2001. 16 The trend in senior female authors has been less impressive with an overall increase of only 4.2% over a 35-year period (from 12.3% in 1970 to 16.5% in 2004).
In this study, we have used the last person listed as the senior author. The assumption that the last listed is the senior author may be perceived as a limitation of the study. However this methodology is similar to Jagsi et al., 12 allowing us to make useful comparisons in this field. In cases where it was unclear, the individual institutions were contacted for clarification.
This study has also shown that variations exist within subspecialties. For example, although obstetrics and gynaecology and paediatrics demonstrate a persistent rise in female authorship this has not been the case within all medical subspecialties with both Gut and Lancet having a decline in the number of senior female authors. This disparity may represent and be determined by the number of women within the different subspecialties. We perceive that the more women within a subspecialty, the more likely there will be prominent female authors. 12
The use of gender authorship of academic medical literature as a surrogate marker of gender imbalance has been validated previously by other investigators. 12, 17, 18 A recent USA study over a similar timespan also observed a similar trend (with overall rates of female authorship rising from 5.9% in 1970 to 29.3% by 2004). 12 The investigators concluded that despite an increase in the number of female first and senior authors (of original research in the USA), women still comprised a minority of original research in the journals studied. The reasons behind the gender disparity have been widely debated, particularly in the USA. A qualitative American study described three main ‘barriers’: historical developments (for example, a shortage of women in the pipeline); broad social forces (gender roles and socialization patterns affecting women's status); and the expression of these forces in the medical environment (for example, sexism in recruitment and promotion practices and a shortage of effective mentors for women). 19 It has been suggested that as long as there is a paucity of women in professorships then it will logically follow that there will be a lack of role models and mentors for female students and residents who wish to seek advice on combining a medical career and raising a family. 20 Part of the Women in Academic Medicine cohort of the Athena Survey of Science Engineering and Technology (ASSET2006) questionnaire that was recently published similarly demonstrated that UK female academics perceived the lack of role models as having a detrimental effect on career progression, more often than their male colleagues. 15
Inherently, women are often at the forefront of child-rearing and caring for elderly parents. While success in academic medicine frequently requires working 70 hours per week or more, this is potentially incompatible with the carer responsibilities. 21 The Department of Health's key report entitled ‘Recruitment and Retention of Academic Staff in Higher Education’ found that career breaks and part-time working may have a detrimental effect on women's careers in terms of research activity. 8 The Athena Survey of Science Engineering and Technology (ASSET2006) survey analysis has also shown that female respondents who had carer responsibilities for parents/partner were less likely to have publications as lead authors compared to those women without carer responsibilities (p<0.001). Furthermore, promotion and tenure in some academic institutions is time dependent or limited. 22 This issue clearly poses a hindrance to women who choose to take time out for childbearing or to reduce hours for family purposes. In addition, there may be less institutional support for female faculty with children. 23
How can this apparent gender imbalance be addressed? There are a number of possible mechanisms that we would suggest: incorporating more part-time options into the currently available research training programmes; 20 career paths in academic medicine should also be more flexible and less narrowly defined; 21 apart from recruitment, attention should also be paid towards the enhancement and advancement of women in academic medicine with the appropriate advice and guidance being readily available from identifiable individuals within every institution.
Conclusion
We conclude that there has been an encouraging increase in the number of female doctors contributing to academic medicine as first authors. In contrast, there is still a considerable lag and in some cases a decline in the number of female senior authors. In the UK, factors that could narrow the gender gap in authorship should be sought and addressed.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
The Women in Academic Medicine project for inclusion of results from the Athena Survey of Science Engineering and Technology (ASSET2006) questionnaire in this body of work