
Abstract
Summary
Objectives
Using frameworks, such as the long-term conditions pyramid of healthcare, primary care organizations (PCOs) in England and Wales are exploring ways of developing services for people with long-term respiratory disease. We aimed to explore the current and planned respiratory services and the roles of people responsible for change.
Setting
A purposive sample of 30 PCOs in England and Wales.
Design
Semi-structured telephone interviews with the person responsible for driving the reconfiguration of respiratory services. Recorded interviews were transcribed and coded, and themes identified. The association of the composition of the team driving change with the breadth of services provided was explored using a matrix.
Results
All but two of the PCOs described clinical services developed to address the needs of people with respiratory conditions, usually with a focus on preventing admissions for chronic obstructive pulmonary disease (COPD). Although the majority identified the need to develop a strategic approach to service development and to meet educational needs of primary care professionals, relatively few described clearly developed plans for addressing these issues. Involvement of clinicians from both primary and secondary care was associated with a broad multifaceted approach to service development. Teamwork was often challenging, but could prove rewarding for participants and could result in a fruitful alignment of objectives. The imminent merger of PCOs and overriding financial constraints resulted in a ‘fluid’ context which challenged successful implementation of plans.
Conclusions
While the majority of PCOs are developing clinical services for people with complex needs (principally in order to reduce admissions), relatively few are addressing the broader strategic issues and providing for local educational needs. The presence of multidisciplinary teams, which integrated primary and secondary care clinicians with PCO management, was associated with more comprehensive service provision addressing the needs of all respiratory patients. Future research needs to provide insight into the structures, processes and inter-professional relationships that facilitate development of clinical, educational and policy initiatives which aim to enhance local delivery of respiratory care.
Introduction
The care of people with long-term conditions is universally recognized as a major challenge to healthcare services. 1, 2 Chronic obstructive pulmonary disease (COPD) is predicted to become a leading cause of morbidity and mortality worldwide by 2020. 3 In the UK, respiratory disease is already the third most common long-term condition. It is responsible for more primary care consultations than any other type of illness, is the major contributory factor in the winter bed crises and accounts for 13% of emergency hospital admissions at an annual cost to the National Health Service (NHS) of approximately £3 billion a year. 4, 5 Primary care organizations (PCOs), charged with commissioning primary and secondary care services for local populations in England and Wales, are responding to this challenge by exploring innovative models to provide cost-effective respiratory care to meet local need. 2, 6 7
The long-term conditions pyramid (LTC pyramid) of healthcare ( Pyramid of care for long-term conditions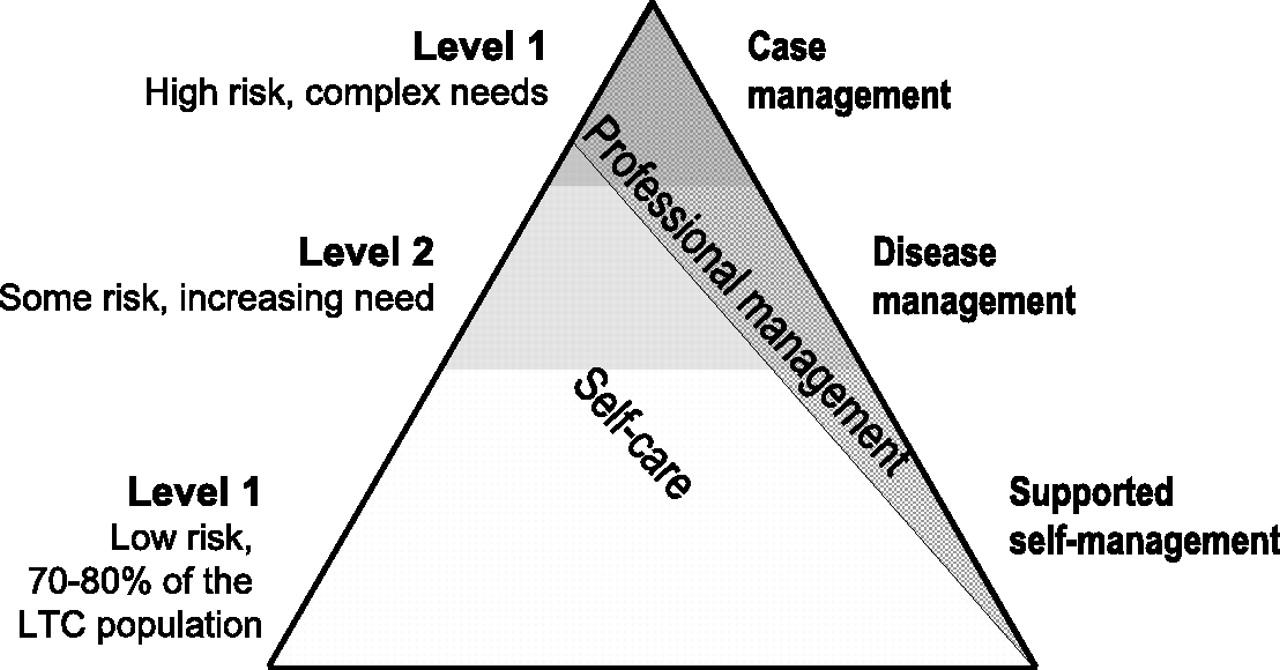
In a recent discussion paper, Gask suggested that although specialists (usually consultants in managed care organizations in the United States on which she builds her argument) traditionally provide clinical services for the minority of patients with complex needs, they also have responsibility for improving the quality of care at all levels of the LTC pyramid. 8 Important aspects of the specialist role, therefore, include addressing education and training needs, and adopting a leadership role in the strategic development of integrated services. Within the UK, healthcare professionals other than consultants, such as specialist nurses and General Practitioners with a Special Interest (GPwSIs), are developing specialist skills and may be expected to fulfil some or all of these additional roles. 9, 10, 11
Our study aimed to understand how PCOs are reconfiguring their workforces to develop respiratory services with a focus on different professional roles, specifically including respiratory GPwSI services. We describe here the initial phase of the study in which we explored the current and planned respiratory services and the roles of people responsible for driving change in a purposive sample of PCOs in England and Wales offering a spectrum of attitudes to the reconfiguration of respiratory services.
Methods
Our study was undertaken in March–June 2006 with the approval of South East multicentre research ethics committee and research governance approval from all relevant PCOs. 12
Sampling of PCOs and recruitment of interviewees
Based on findings from a previous survey, 13 supplemented by a database of trusts who had expressed interest at the time of the publication of the General Practice Airways Group Respiratory GPwSI resource pack, 14 we purposively sampled 30 PCOs in England and Wales representing a wide spectrum of attitudes to the reconfiguration of respiratory services (including ‘well advanced plans’, ‘early stage of considering the options’, ‘have a GPwSI in post’, ‘prefer alternative models of care’, ‘no plans for developing respiratory services’). In addition, we ensured a geographic spread with a range of population size and demography. We approached PCOs by letter, followed up by a phone call, requesting a 45-minute telephone interview with the person(s) responsible for driving the reconfiguration of respiratory services or the person responsible for other comparable chronic disease services in PCOs not planning reconfiguration of respiratory services.
Interview schedule
Based on our previous work, 13, 15 and our understanding of the literature relating to the management of long-term conditions 2, 8 16, 17 and the evolution of clinical roles, 10, 10, 14, 18 we devised a semi-structured interview schedule, collecting data on size and demographics of the PCO population, preferred model of care for respiratory disease, key drivers, person(s) responsible for the changes, and proposed management arrangements for new services. Appendix 1 shows the full schedule. Interviews were conducted by one researcher (AT) and we continued to recruit PCOs until no further themes emerged.
Data handling and analysis
Interviews were audio-recorded (excluding interviews 1 and 2 for technical reasons) and extensive notes taken on prestructured forms. Recorded interviews were anonymized and fully transcribed. Data analysis was carried out by two researchers (HP, SH) with discussion regarding emerging frameworks and coding strategies taking place at regular intervals with other members of the team.
Data analysis was iterative and emerging themes were used to inform the subsequent interviews. Analysis and consultation of the literature proceeded in parallel and we drew on literature in relation to the role of specialist services, 8 and the levels of care of people with long-term conditions. 2 We adopted the thematic approach to analysing qualitative data described by Ziebland et al. 19 searching specifically for unanticipated themes and deviant cases. Emergent themes were discussed by all members of the multidisciplinary team during a project workshop.
Description of the criteria for grading engagement of key stakeholders and the breadth of the specialist roles described
The PCOs: their demography, models of care and role of interviewees
Results
From an initial mailed approach to 110 PCOs, 40 considered our request for an interview and, after discussion with their line managers, 30 agreed to participate. Where a reason was given for non-participation, time, workload and lack of alignment with current priorities were cited. The demographic details of the PCOs, professional role of the interviewee, and preferred model of care are given in Table 2.
Functions of the specialist services
Examples of specialist services described by the PCOs
Clinical
Almost exclusively, the clinical services described were designed to meet the needs of patients with the most complex needs who were judged to be at significant risk of hospital admission.
The clinical priority for almost all the PCOs was the reduction in hospital bed-days, though the approach taken varied between localities: commonly a nurse-led intermediate care service, often complemented by community matrons providing case management for a few highly complex patients, though examples of other innovative approaches were also given (Table 1). For local reasons (e.g. low prevalence of COPD), two PCOs had not prioritized the provision of specialist COPD services.
Pulmonary rehabilitation was universally acknowledged as important, though few
interviewees were satisfied with the service they provided. Most described their
current service as ‘inadequate’, or ‘a pilot project’ with an uncertain future,
though hoped that in time they would be able to increase provision.
‘We started a community pulmonary rehab programme in addition to the
one that the Acute Trust runs but the funding runs out for that at the
end of March. So, at the moment, my responsibility is trying to ensure
that we get the funding to continue that through practice-based
commissioning.’ (PCO 9: Respiratory nurse team; Interviewee: PCO
manager)
Other clinical services described were isolated examples of innovative practice
(e.g. referral management, oxygen services, telemonitoring, Meteorological Office
health forecasting, palliative care services for people with COPD). Services for
respiratory conditions other than COPD, or for children with respiratory disease,
were rarely mentioned.
‘I think there's always been an aspiration that the team would move
on from COPD as well, that COPD would be its main focus to begin with
then as services are established and skills and expertise in that area
generally across the health community kind of increased that other
respiratory diseases would kind of come into being such as asthma and so
on, but again there are no definite plans for that to happen at this
point in time.’ (PCO 21: Respiratory nurse and community matron team;
Interviewee: Service development manager)
Educational
The need to raise standards of respiratory care in primary care was widely
acknowledged, though only a minority of PCOs had well-developed plans in place for
how this was to be achieved. While a few PCOs used audit tools and support
strategies such as in-house mentoring to work with practices, others relied on
educational methods known to be ineffective at changing practice (e.g. lectures,
distributing local guidelines).
20
Plans for training nurses were often described in clearer terms than
strategies to improve GPs skills.
‘What we try to do is we work with a longer pathway so we have for
example, we work with practices and we send in, we have what we call our
[specialist nurse], who's a nurse who basically just goes in and works
with practices to set up systems of identification and better management
and order etc … But she specifically works with primary care to develop
services within primary care.’ (PCO 17: GPwSI-led service; Interviewee:
GPwSI)
‘So the respiratory team have outlined, we have a CDM [chronic
disease management] monthly newsletter, so it's gone out in the
newsletter about what work up should happen for patients, what's expected
so we've been really clear about that. What tests and blood tests, etc.
need to be done before they go to a clinic.’ (PCO 11: Respiratory nurse
service; Interviewee: Service development manager)
Some PCOs were developing a ‘competency-based’ approach to defining training
needs, particularly in the context of community nursing, as district nurses,
specialist respiratory nurses and community matrons all contributed to the care of
people with COPD.
‘I think, very much in terms of defining the care pathways very
carefully. All the ones like mapping the service and then deciding who
needs to fit in where within that mapping and then the competencies for
each of those to be utilized and based on any kind of national competency
framework.’ (PCO 4: Respiratory specialist nurses; Interviewee:
Governance manager)
Strategic
The LTC pyramid (Figure 1) was widely cited
and, for most PCOs, was the basis of their strategic planning, though many
acknowledged that, at the moment, their focus was primarily ‘looking at the top of
the triangle for those most vulnerable patients’ with less clarity about how to
address the needs of the majority of patients at the lower levels of the pyramid.
Some PCOs had a respiratory strategy that was embedded ‘in the context of the
long-term conditions agenda’, potentially ‘connecting up’ care for people with
co-morbidity and dove-tailing with ‘expert patient’ programmes to ‘help people
take control of their own health’. At one end of the spectrum there were PCOs with
well-developed teams, often given a name and a clear identity, with a phased
programme of development. By contrast other PCOs were yet to develop a strategy.
‘Our programme for long-term conditions within this PCO is known
collectively as [team name] and in phase one of the programme we
established a community respiratory service, a community rapid response
service which was linked to intermediate care, the development of
community matrons and the further expansion of community beds. So while
they are all individual service developments they are all connected
together really to deliver an overall impact, if you like, in terms of
the development of services for improved management of people with
long-term conditions and particularly older people in that first phase.’
(PCO 21: Respiratory nurses and community matrons; Interviewee: Service
development manager)
Mindful of the impending reorganization of PCOs, some trusts were already discussing with colleagues from neighbouring PCOs how their strategies might align in the event of a merger, potentially enhancing services and sustainability. For many others, however, uncertainty about the future structures, and their own personal role within the reorganized trusts, was expressed in terms of ‘confusion’, ‘frustration’, ‘instability’ with a resultant sense of inertia making it ‘very, very, very difficult to plan anything’. Financial restrictions, often linked with the reorganization, were a major factor impeding development.
Teamwork
Teamwork between managers and representatives from primary and secondary sectors
emerged as a key factor in the effective development of services with stakeholders
perceived as offering diverse perspectives and complementary skills. Some
interviewees offered enthusiastic descriptions of coherent teams driving change.
‘What was very unique about our project team was the fact that we had
clinicians and managers working very closely together across primary,
secondary care. And I think that established the right team structure to
actually get things done.’ (PCO 17: GPwSI-led service; Interviewee:
GPwSI)
Roles within the team
PCO managers were seen as having an important facilitatory role, often providing
an essential drive ‘at the start of the programme’ by focusing attention on the
need to develop pathways to prevent ‘inappropriate’ admissions. The majority of
PCOs turned naturally to the acute sector for their clinical advice in setting up
‘Hospital at Home’ services especially in the absence of interest from GPs. Lack
of ‘buy-in’ from GPs was cited as a significant threat to implementation of
services.
‘Yes and there is a bit of a change I suppose within the PCO, about
well, there's no point in us doing this if this isn't going to be owned
by the practices, you know, it needs to come from them really now, every
service development now really should have the support of the practices
behind it.’ (PCO 21: Respiratory nurses and community matrons;
Interviewee: Service development manager)
Clinicians from primary or secondary care sometimes fulfilled the role of a champion, being described as ‘very, very committed to developing the service’ and people who ‘have a passion to move things on’. It was thought that to be effective, clinical leaders should be knowledgeable, visionary, enthusiastic and tenacious, locally respected clinicians who were good at building relationships and were supportive mentors who could set standards.
If natural leaders were not forthcoming, PCOs often sought ways to encourage
clinical engagement, for example by obtaining a ‘specific nominated lead in each
GP practice for respiratory disease’. Practice-based commissioning (PBC) was
widely seen as a potential mechanism for increased involvement of clinicians.
‘I mean we see it [PBC] as the real drive to get them much more in a
leadership position to say “Well, you know, this isn't right, how can we
provide it differently?” So I would say, you know, we anticipate it
having a huge impact on influencing where resources are going and their
referral patterns, etc.’ (PCO 10: Respiratory nursing team; Interviewee:
Nursing manager)
The importance of relationships
Tensions could arise between the PCO managers' need to achieve financial savings
and the clinicians' broader vision of improved services. Relationships between
primary and secondary care, or between respiratory nurse specialists and community
matrons, were sometimes fraught. Candid discussion between all stakeholders could
allow diverse perspectives to be appreciated and objectives aligned.
‘I think the PCO driving force is the economic side of things … so I
do feel that I'm basically trying to drive through a clinical area but
obviously understand that you will only achieve these things if you
satisfy other people's aims as well.’ (PCO 14: GPwSI service;
Interviewee: GPwSI)
Entrenched professional attitudes (variously described as ‘obstinate’,
‘resistant’, ‘territorial’, ‘prejudiced’) could block effective engagement of
clinicians, though some interviewees attributed obstructive attitudes to ‘a lack
of understanding’ which might respond to ‘an evolutionary approach’.
‘Correct, it's a little bit about protectionism and a little bit
about he loses control and a little bit about actually does the evidence
base support that these services can be developed safely, to be safe and
indeed effective.’ (PCO 12: Respiratory nurse team; Interviewee: Service
development manager)
‘No I don't think it's being obstinate I mean don't get me wrong
there are probably some individuals who are obstinate I think you'll find
that in all walks of life … I think generally it's about understanding
and you know what the ability of community and primary care can do.’ (PCO
19: Respiratory nurse service; Interviewee: Service development
manager)
Professional involvement and roles of specialist service
Association between increasing engagement of key stakeholders (PCO manager, primary and secondary care clinicians) and the breadth of the specialist roles described (clinical, strategic and educational)
Involvement of PCO managers, secondary and primary care clinicians are illustrated in the first three columns, the number of symbols reflects the degree of engagement. Table 1 shows details of grading
+ Limited engagement
++ Substantial engagement
Roles provided by the specialist service are illustrated in the second three columns, the number of symbols reflects the priority, and depth of the service provided
No provision
✓ Role mentioned, but with minimal corroborative evidence
✓✓ Role described, with some specific examples
✓✓✓ High priority given to role
Discussion
The services currently being developed by PCOs are aimed at the immediate goal of reducing COPD admissions and are therefore focussed on the care of people with high-risk, complex needs. Despite universal awareness of the LTC pyramid, only a minority of the PCOs had a coherent strategy to ensure that the majority of patients with less complex needs also had access to high quality respiratory care. The specialist services – most commonly nurse-led intermediate care – had a limited remit to provide education for primary care and few were actively involved in the strategic planning of services.
PCOs commonly turned to specialists in the acute trust for expert advice on developing ‘hospital at home’ services, but active involvement of clinicians from both primary and secondary care was less common. Teamwork with more explicit engagement of clinicians was associated with the provision of specialist services with a broader remit embracing not only the clinical needs of patients with a more diverse range of diseases and severity, but also strategic and educational roles. Where successful teamwork was achieved it was valued and resulted in a fruitful alignment of objectives, while in other PCOs, the challenge of overcoming lack of interest, antagonism, and entrenched attitudes could prove to be insurmountable. The imminent merger of PCOs, and financial constraints resulted in a ‘fluid’ context which further challenged successful implementation of plans.
Limitations and strengths
Our purposive sample of 30 PCOs may not have encompassed the full range of contexts in PCOs throughout England and Wales, and is likely to have favoured PCOs with an interest in respiratory services. However, we achieved a good geographic spread with a range of population size and demography and we continued to recruit until saturation was reached, specifically including two PCOs with no plans to develop respiratory care. Our data about each PCO are derived from one informant who may not have been fully aware of the situation in their PCO. Although we standardized our requests to PCOs, asking to speak to the person responsible for driving the reconfiguration of respiratory services, as expected the interviewees held diverse managerial and/or clinical roles. This flexible approach may have reduced the comparability of the reports we obtained, but enabled us to accommodate the diverse organizational models operating in PCOs. We recognize that they will have described the services from their perspective which may not be shared by other stakeholders in the trust. Interviewees may have omitted to mention some topics or services, though we used a structured topic guide to ensure that we asked specifically about relevant issues.
The idea that there might be an association between clinical engagement and breadth of service provision emerged during the analysis, so although our topic guide covered all the relevant issues, we did not systematically request information about this relationship. Importantly, our qualitative methodology limits inference about the direction of this observed relationship and the impact of confounding factors.
Although the analysis presented in this paper was led by one researcher (HP) potentially biasing interpretation of emerging themes, other members of the team (SH, GH) worked with the same data, 20 and the findings were discussed and agreed. A major strength is the multidisciplinary expertise (clinical, health service management, anthropological) available within the study team, ensuring balanced conclusions.
Interpretation of findings in relation to previously published work
Gask argues that a specialist (a consultant physician, or possibly a specialist nurse) should not only address the clinical needs of those with severe or complex illness, but also has a responsibility to ‘improve the quality of care for those who don't need specialist care’. 8 The evolution of the GPwSI concept reflects this broadening of emphasis as the initial description of a GP undertaking a specific clinical task 22 has been challenged in subsequent discussions, 10 and official guidance now recognizes the potential contribution GPwSIs can make to strategic development of services and raising standards in primary care. 18, 23 Previous surveys and qualitative work have endorsed this broader remit for GPwSIs. 13, 15 24 Our findings suggest that, at least in some PCOs, these roles may be incorporated into the design of a specialist service, with different professionals fulfilling clinical, educational and strategic roles to ensure a comprehensive service.
The importance of collaboration between clinicians and managers to improve local services, and the need for effective clinical leaders has recently been highlighted. 25 The challenges of working collaboratively, however, are well recognized, 26 and echoed by our interviewees who at times struggled to build effective teams against a background of financial constraints and reorganization. 20 Our data, however, suggest that involvement of both primary and secondary care clinicians may be important in ensuring that the needs of patients with long-term conditions at all levels of the pyramid are met. We thus provide support for the concerns expressed by Ham in his recent discussion paper that services for chronic disease are best served by ‘clinically integrated groups’ overseen by PCOs rather than by a ‘quasi market’ in which contracted services lack the flexibility to respond to complex clinical and social needs of people with long-term conditions. 27 Practice-based commissioning was in its infancy at the time of our study, but many of our interviewees supported the policy, believing that it had the potential to improve primary care clinical engagement. 28
An unresolved question is the organizational level at which teamwork operates most effectively. We investigated development at the level of the small pre-merger PCOs, while current English NHS policy recommends that networks should be established at the higher Strategic Health Authority level. 25 By comparison, in Scotland, Managed Clinical Networks advise on healthcare provision at a level intermediate between these two extremes. 29, 30 Since our interviews, the merger is likely to have impacted on the dynamics within the PCOs and further work will be needed to understand whether strong teamwork helped overcome the disruption of reorganization, or whether the new organizational structures damaged existing teams.
NHS policy is actively promoting clinical leadership. 31 Our observed association between teamwork involving primary and secondary care professionals with PCO managers and successful development of services may be seen to support a hypothesis that clinical engagement is a prerequisite for service improvement. This would, however, be too simplistic: clinical engagement may be necessary, but was not sufficient. Our interviewees offered examples of clinicians providing valued leadership, but also of obstructing progress. Established teams could be undermined by PCO reorganization and their plans thwarted by financial constraints. We also saw examples where clinicians were able to compensate for lack of engagement from another sector. In one PCO, lack of primary care involvement was balanced by a consultant working in the community; in another a GPwSI provided specialist expertise instead of a reluctant consultant. Exploration of these complex dynamics could yield an understanding of how clinical engagement and teamwork can be facilitated to support the effective reconfiguration of services.
Conclusions
While the majority of PCOs are developing clinical services for people with complex needs (principally in order to reduce admissions) relatively few are addressing the broader strategic issues and providing for local educational needs. The presence of multidisciplinary teams, which integrated primary and secondary care clinicians with PCO management, appears to be associated with comprehensive service provision addressing the needs of a wide range of respiratory patients. Future research needs to provide insight into the structures, processes and inter-professional relationships that facilitate development of clinical, educational and policy initiatives which aim to enhance local delivery of respiratory care.
Footnotes
DECLARATIONS
The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Department of Health
Footnotes
Acknowledgements
We thank the Independent Steering Committee, chaired by Bonnie Sibbald, for overseeing the project. We acknowledge the contribution of Rosemary Porteous who set up and transcribed interviews, and are grateful to our interviewees and their primary care organizations who gave of their time and expertise
Appendix 1 Topic guide for the interviews
Schedule for the initial semi-structured screening interview with the person responsible for driving the reconfiguration of respiratory services in up to 50 PCOs (Workforce 1 – PCO screening. Interview schedule v1. 2.10.05):