
Abstract
Summary
The great artist and one-time revolutionary, Jacques-Louis David died in 1825. The cause of his death has been open to speculation. An extraordinary sequence of portraits of the artist describes his transition from handsome middle age to a deformed old man. During this phase a swelling appears at the angle of his left jaw and over a period of 20 years a facial palsy can be diagnosed. We submit that this evidence suggests that malignant transformation of a pleomorphic adenoma of the parotid gland was the proximal cause of his death.
The life and times of Jacques-Louis David
Soon after the celebrated painter and one time regicide, Jacques-Louis David, died on 29
December 1825 at the age of 77, a Dr Chalupt carried out an autopsy and concluded that
death had occurred from hypertrophia of the heart.
1
The previous summer his breathing had been reported as beginning to be laboured
and his morale a little weakened: ‘… il a un commencement d’asthme et le morale un peu affaibli’ ‘…Il éprouve un étouffement continuel qui ne lui permet pas même de marcher et
fait présumer un anéurisme du coeur…’
(Talma in a letter to Ducis the date of which, however, is not certainly November of 1825), 1 and by the end of that month he had lost the use of his drawing hand. 1 On 19 December David managed to go to the theatre, 1 but then became more ill and in his final illness was conscious only intermittently. 1
This relatively peaceful end belied an eventful, even stressful, life in which after
early struggles he had successively claimed moral then actual leadership of the French
School, taken a leading part in the most radically republican phase of the French
Revolution, been twice imprisoned, and became Napoleon’s painter before going into exile
in Brussels in 1816 soon after the restoration of the French monarchy. It was above all
David’s political involvement during the Revolution as a supporter of figures such as
Robespierre and Marat, and as one who had voted for the execution of Louis XVI, which
earned him the undying enmity of monarchists and constitutionalists on both sides of the
Channel. This enmity seems to have influenced a number of disparaging remarks about his
physiognomy. Thus in July 1792 Le journal à 2 liards, directed by the
royalist Pouteau, wrote: ‘I have seen this David so dumb, so mean looking, and so truly tagged with the
seal of condemnation. No one is more hideous nor more diabolically ugly. If he is
not hung, you should not believe in physiognomy.’
1
When the author Walter Scott visited Paris in 1815 he is said to have thought that
David’s physiognomy was the most hideous he had ever seen, and his disgust was not
lessened by knowledge that he had just met the painter ‘of the blood-stained brush’.
2
Scott and Pouteau were both referring to a marked swelling of David’s left cheek. This
seems to have been apparent by 1784–1785 when the English gem-engraver, Nathaniel
Marchant,
3
met David in Rome and some 12 years later commented to the artist Farington: ‘One side of his face is much larger than the other and appears as if swelled’
Marchant′s reference to David′s wife, whom he had married in 1782, in another part of the diary entry cited makes it clear that he met David during the latter′s second stay in Rome in 1784–1785, and not during the artist′s first stay in 1775–1780. 4
By the time Marchant met David the latter was no more than 37 years old. According to
the artist’s grandson, himself reporting what David’s children had told him, the cause
of the swelling was a badly cared for sword wound to the upper jaw suffered by the
artist when he was about 25. This apparently led to ‘an exostosis which never stopped growing and added to his speech defect’.
5
Although Farington in 1802 described David’s right cheek as ‘much swelled’,
6
extant portraits of the artist show that it was his left cheek which was
affected – if they show the swelling at all. That the swelling was on the left side is
most apparent in a posthumous maquette of c. 1826 François Rude, 1794–1855, a portrait of Jacques-Louis David, c. 1826 Terracotta
maquette 22.5cm high. Daniel Katz Ltd., UK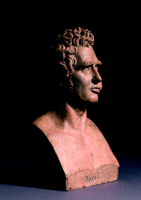
That the swelling was on the left side is also clear from a print made by Jean-Pierre-Marie Jazet (1788–1871) in 1822 after a drawing of the same or previous year by a former pupil Joseph Odevaere (1775–1830). 8
Unfortunately no certain portrait of David as a young man exists so, save in respect of Marchant’s testimony, it is impossible to say how early the swelling on his cheek became apparent. The earliest known portraits of David show him in profile, or virtual profile, from the right (so indirectly confirming the probability that his features were distorted on the left). Among these is a profile portrait by Jean-Baptiste Wicar (1762–1834) made in 1788 after a lost portrait by another pupil of David, Anne-Louis Girodet de Roucy-Trioson (1767–1824), itself perhaps made around 1786. 9 The same applies to another drawn portrait made by Jean-Baptiste Isabey (1767–1855) in 1789. David’s self-portraits of 1791 and 1794 are mirror images and show the artist’s left cheek in shadow, not that David was ever likely to feature what was said to be his nickname, namely ‘grosse joue’. 10 At all events by 1812 or 1813 when David’s trusted assistant, Georges Rouget, made a portrait of the master, the swollen cheek was evidently becoming impossible to ignore. 11
It was the art historian, Jacques Wilhelm, who in 1960 first mentioned that David’s swollen cheek might have a cause other than a poorly cared for wound. 5 In an article on portraits of David Wilhelm published Dr Ledoux-Lebard’s suggestion that the swelling was more likely the result of a mixed slowly evolving tumour of the parotid gland, 12 and this explanation has been generally accepted ever since.
Swellings of the parotid gland
The parotid gland overlies the angle of the jaw each side of the face and is the most important of the four major salivary glands (the other two being the submandibular glands). All medical students are taught that a swelling overlying the angle of the mandible arises from the parotid gland until proved otherwise. The parotid gland drains through its duct into the mouth just alongside the second molar tooth. Perhaps the commonest swelling of the parotid occurs in childhood as acute viral parotitis or ‘mumps’. Next in frequency is an impacted salivary stone that leads to a sudden painful swelling in this area aggravated by the smell or taste of food. Any swelling in the parotid area that is painless and slow growing is almost always a pleomorphic adenoma or ‘mixed parotid tumour’. 13 The parotid gland consists of a superficial and a deep lobe separated by the facial nerve that splits into five filaments like branches around an isthmus that joins the two lobes. The facial nerve supplies the muscles of facial expression. Fortunately for the surgeon the majority of mixed parotid tumours occur in the superficial lobe allowing for their removal without damaging the facial nerve. The consequences of damaging even one branch of the facial nerve can produce hideous changes known as facial nerve palsy. This appearance may occur spontaneously from an acute viral infection known as ‘Bell’s palsy’. Mixed parotid tumours grow slowly and are quite benign but are usually removed at an early stage so it is difficult nowadays to understand their natural history. The portraits of David allow us a rare opportunity to study how the condition progressed in the days before surgery might have been considered. Over a 30- or 40-year period we can see the slow growth of the swelling on the left side of the cheek.
However something dramatic appears to happen after about 20 years when David’s
physiognomy changes as the ugly drooping of the lip and flaccidity of the left side of
the face gradually develops. These are the characteristic signs of a facial palsy. Mixed
parotid tumours are benign and therefore cannot infiltrate or compress the facial nerve.
However in about 10% of neglected cases malignant transformation can occur
(adeno-carcinoma) leading to facial nerve palsy ( An elderly man with a malignant parotid tumour. Note drooping of the corner of
the mouth from infiltration of the buccal branch of the facial nerve
It was claimed that David’s disfigurement was as a result of a badly treated sword wound. This is highly unlikely as the facial palsy would have been instant had the facial nerve been transacted not of gradual onset over a number of years.
It was also claimed that David’s autopsy showed death from ‘hypertrophia’ of the heart. However this has no modern clinical meaning as a cause of death. For example, left ventricular hypertrophy might be as a result of uncontrolled hypertension; whereas right ventricular hypertrophy might result from chronic lung disease. If the unchecked growth of a parotid cancer slowly occluded his airways then a state of chronic hypoxia would have developed that in itself might lead to hypertrophy of both sides of the heart as it attempted to compensate for the diminished flow of oxygen by increasing the pump rate to exhaustion.
We can therefore reasonably claim that Jacques-Louis David died as a consequence of the unchecked spread of adeno-carcinoma of the parotid gland.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None