
Abstract
A history of cardiac disease, especially atrial fibrillation, together with symptoms such as loin or abdominal pain, and accompanied by an elevated lactate dehydrogenase should prompt a computed tomography scan to exclude the diagnosis of acute renal infarction.
Case history
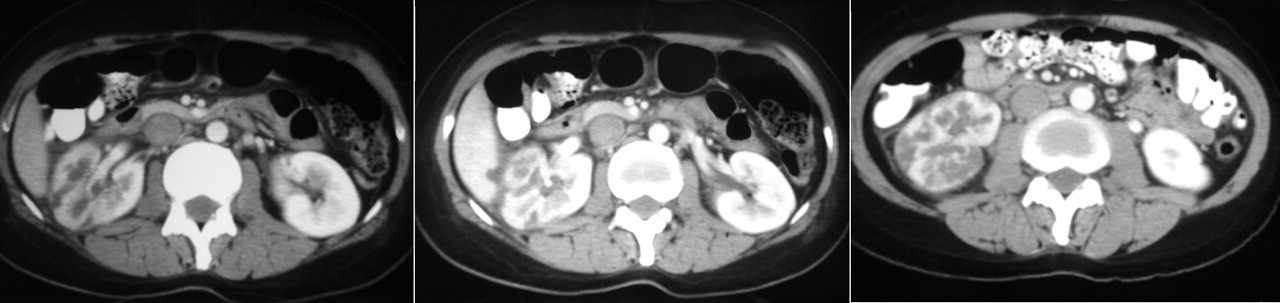
A 38-year-old lady was admitted to hospital with a two-day history of right loin pain and lethargy. The pain was colicky in nature and mostly experienced over the right lower abdominal quadrant and flank area. Physical examination showed a tired-looking patient with right costovertebral angle tenderness. Urinalysis showed microscopic haematuria 3+ and absence of pyuria. She had a white blood cell count of 13.9 × 109/L with 89% polymorphs and a blood creatinine level of 1.0 mg/dL (91 μmol/L). The alanine transaminase level was 168 U/L, and the lactate dehydrogenase level was 1083 U/L (normal value 87-213 U/L). Both abdominal plain film and ultrasound showed no evidence of hydronephrosis or renal calculi. The following day she developed fever without chills. She was treated empirically as pyelonephritis with ciprofloxacin, which did not alleviate her symptoms. She also complained of palpitation symptoms two days after hospitalization; the electrocardiogram showed atrial fibrillation and no evidence of pulmonary embolism. A contrast-enhanced computed tomography of the abdomen and pelvis (Figure 1) was performed five days after admission because of unresolved fever and symptoms. It demonstrated multiple wedge shaped hypodensities indicative of multifocal infarcts involving the right kidney, with evidence of filling defect (thrombus formation) in the main renal artery causing partial obstruction. The patient was anticoagulated and underwent transthoracic and transesophageal echocardiogram. Grossly enlarged atria secondary to rheumatic mitral stenosis was noted with an estimated mitral valve area of 0.76 cm2. Apart from an organized thrombus detected over her left atrial appendage, no vegetations were seen on any heart valves.
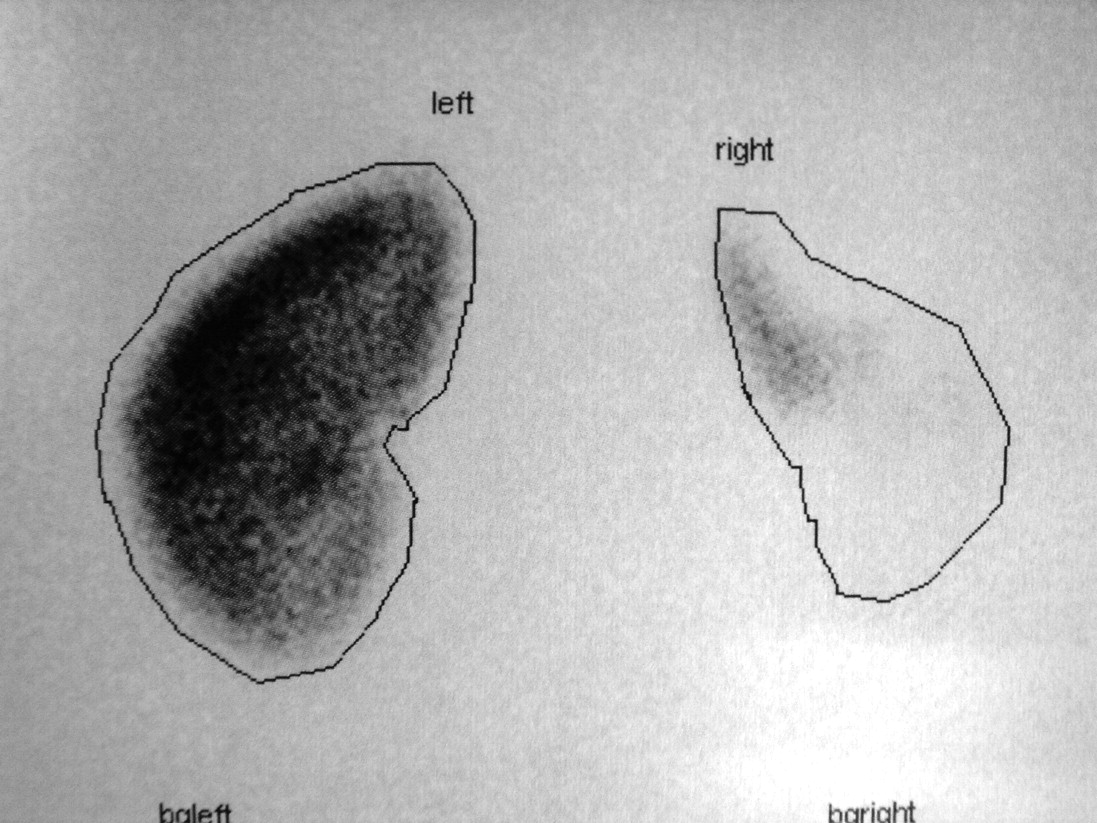
On the basis of the delay in the diagnosis of acute renal infarction secondary to atrial fibrillation and embolism, thrombolysis was not attempted. Treatment with anticoagulation was continued. Her renal function remained relatively well preserved, with a serum creatinine of 0.77 mg/dL (68μ mol/L) two months afterward. Diagnostic technetium-99m dimercaptosuccinate (DMSA) renal scintigraphy (Figure 2) revealed a severe loss of right renal cortical function, in keeping with a history of renal infarction. Our patient subsequently underwent mitral valve replacement, with no further embolic phenomena.
Discussion
The initial clinical manifestation of acute renal embolism in our patient, in retrospect, was clouded by the focus on acute pyelonephritis. However, the lack of response to antibiotic therapy should prompt a strong clinical suspicion of an alternative diagnosis and further evaluation. According to Bayesian reasoning, the elimination of a given diagnosis is linked to the heightened probability of an alternative diagnosis. Furthermore, the exceptionally high lactate dehydrogenase level, together with the presence of atrial fibrillation, has been shown to indicate a high likelihood of acute renal infarction. 1-3 According to the largest case series of renal embolus complication atrial fibrillation yet published, serum lactate dehydrogenase elevation >400 U/L occurred in 41 of 44 cases (93%). 1 Contrast-enhanced computed tomography of the abdomen can often improve the diagnostic yield. 4
That said, it is worth noting that late diagnosis of acute renal infarction, as opposed to acute myocardial infarction, has remained to be the norm. In fact, delayed diagnosis of this disease entity had been reported in 48-50% of the cases. 1,5 As such, treatment of this condition is largely aimed at prevention of embolization with anticoagulation because of the too-often late diagnosis.
Footnotes
DECLARATIONS