
Abstract
Objectives
In 2009 more women attended cervical screening in England and Wales than in the previous year. Described as the ‘Jade Goody Effect’ this was attributed to the death from cervical cancer of a UK celebrity. The present study aimed to establish which sociodemographic characteristics were associated with being influenced by Jade Goody's story.
Methods
Data were collected as part of a Taylor Nelson Sofres (TNS) omnibus survey using random location sampling. Women in England aged 26-64 years were asked to report whether they felt Jade Goody's story had influenced their decisions about cervical screening over the 18 months between her death and the time of the survey.
Results
Data from 890 participants was included in analysis. Over a third of women felt Goody's story had influenced their decisions about cervical screening (40%). Younger women (aged 26-35 years) were more likely to have been influenced by Goody's story than older women (56-64 year olds). There was also evidence of socioeconomic variation with women from lower socioeconomic class groups and those with fewer educational qualifications more likely to say they had been influenced by Goody's story.
Conclusions
The ‘Jade Goody Effect’, as acknowledged by women themselves, was more pronounced among young women and influenced screening decisions more markedly among those from lower socioeconomic backgrounds. Narrative communication may be an effective way to encourage attendance at cervical cancer screening and reach groups of the population that are difficult to reach using traditional intervention methods.
Introduction
In 2008-2009 an additional 0.4 million women in England attended cervical cancer screening compared with the previous year, 5 a rise that has been attributed to the high-profile diagnosis and death from cervical cancer of the young celebrity, Jade Goody.6–8 Across England and Wales, there were peaks in screening attendance following Goody's diagnosis and death,5,9 with decreased response time to invitations and increased referrals to and attendance at colposcopy. A large proportion of the extra attenders were overdue for screening, 5 and increased diagnosis with dyskaryosis, cervical carcinoma in situ and invasive cancer suggest that many of the women who attended following Goody's story were at high risk for cervical cancer.9,10 The ‘Jade Goody Effect’ seemed to have most impact on younger women,5,9,10 which is encouraging given that coverage is poorest in this group. 11
The finding that Jade Goody's experience of cancer resulted in increased screening uptake is consistent with other celebrity cancer diagnoses,12,13 and TV storylines.14,15 Coverage of celebrity cancer experiences through the mass media has the potential to reach large proportions of the population, many of whom may not be easily accessible through traditional health promotion routes. Goody's story also received more coverage through tabloid newspapers 8 which attract readers from lower socioeconomic groups, arguably those who are most in need of exposure to information highlighting the importance of cervical screening.16,17
Media coverage of celebrity cancer experiences also offers a personal level of communication in the form of a narrative with which the audience can identify, in contrast to traditional public health campaigns which focus on facts and figures (non-narrative information). This distinction between narrative and non-narrative forms of cancer communication has recently begun to attract attention.18–20 Narrative communication refers to ‘any cohesive and coherent story with an identifiable beginning, middle and end that provides information about scene, scene characters and conflict’ (ref. 19 p. 778). Goody's story is a good example of a form of narrative communication, following her experience from diagnosis, through treatment to death, including details about her behaviours and emotions and setting these in the wider context of her family situation. Narrative cancer communication offers social connections relevant to cancer, allowing the audience to develop a relationship with the character in the story, identify with the character and feel a sense of involvement. 20 This form of communication makes information easier to remember and more difficult to refute. 19
Narratives seem to work best when the audience identifies with the character, 21 which is consistent with the finding that the ‘Jade Goody Effect’ had most influence on younger women closer to Goody's own age. Few studies have explored other sociodemographic predictors of being influenced by Goody's story. We aimed to establish the sociodemographic characteristics that were associated with being influenced by Jade Goody's cancer diagnosis.
Methods
Participants
Data were collected as part of the TNS omnibus survey. Random location sampling was used to select 143 sampling points, within which a postcode sector was selected. At each location participants were recruited in accordance with pre-set quotas (based on gender, employment and children within the home). This ensured that the sample broadly represented the population. We commissioned questions on cervical screening to be asked of women aged 26-64, living in England, who took part in two waves of the survey in September 2010 (18 months after Goody's death). The study did not require University College London (UCL) Research Ethics approval because data were collected anonymously. TNS abide by the Market Research Society Code of Conduct and data protection legislation.
Measures
Women self-completed the survey on a device similar to a laptop. They read the statement ‘You may remember that Jade Goody, the TV personality who became famous after appearing on Big Brother, died of cervical cancer in March 2009. Some women were influenced by her story’ followed by the question ‘How much would you agree or disagree that Jade's story has influenced your decisions about cervical screening in the last 18 months?’ (Strongly disagree, Disagree, Neither agree nor disagree, Agree, Strongly agree).
Women also responded to questions assessing sociodemographic background (see Table 1). Socioeconomic class (SEC) was assessed using the profession of the chief household earner. 22 Responses were coded as AB (managerial/professional); C1 (supervisory); C2 (skilled manual); D (semi-skilled/unskilled manual) or E (state pensioners or causal lowest grade workers). Cervical screening status was assessed by asking women to select from the following: I have had a test within the last three years; my last test was 3-5 years ago; my last test was more than five years ago; I have never been invited to have a test; I have been invited but have never had a test; I have had a hysterectomy so I don't need to have tests; I have never heard of cervical screening. Women were coded as up to date with cervical screening if they reported that they had attended in the last three (26-49 year olds) or five years (50-64-year olds).
Sociodemographic predictors of being influenced by Jade Goody's story
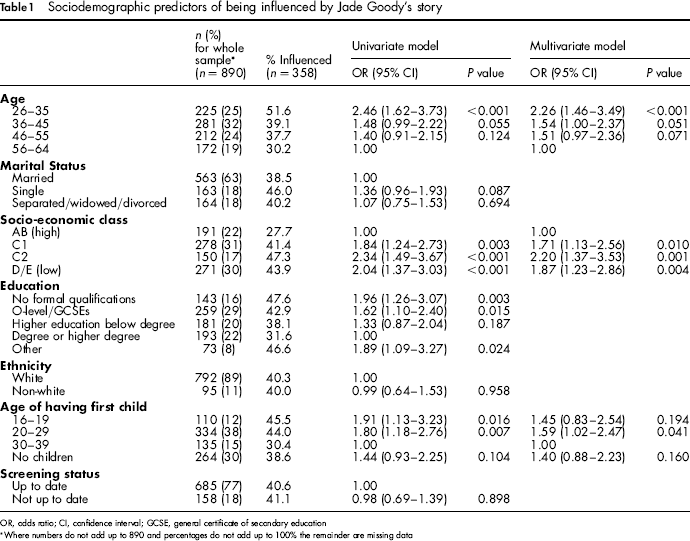
OR, odds ratio; CI, confidence interval; GCSE, general certificate of secondary education
Where numbers do not add up to 890 and percentages do not add up to 100% the remainder are missing data
Analysis
Data were analysed in Predictive Analysis Software Statistics version 18 (IBM, New York). Logistic regression was used to establish correlates of being influenced by Goody's story. Women were coded as ‘influenced’ (agree/strongly agree) or ‘not influenced’ (disagree/strongly disagree/neither agree nor disagree). Significant variables were entered in a multivariate model.
Results
A total of 1031 women took part in the survey. Women were excluded from analyses if they had had a hysterectomy or had never heard of cervical screening (n = 47), refused to answer the question about being influenced by Goody's story (n = 54) or responded ‘don't know’ (n = 40). Demographic characteristics of the remaining 890 women are shown in Table 1 and demonstrate a good range of age and social class groups.
Overall 40% (n = 358) of respondents agreed or strongly agreed that Goody's story had influenced their decisions about cervical screening in the 18 months since her death. A similar proportion disagreed or strongly disagreed (37%, n = 329) and 23% (n = 203) neither agreed nor disagreed.
Univariate logistic regression was used to explore the predictors of being influenced (n = 358) versus not being influenced (n = 532) by Goody's story (see Table 1). Being younger and having a first child at a younger age were both associated with reporting having been influenced by Goody's story. We also found evidence of socioeconomic differences, with those from lower SECs more likely to say they had been influenced by Goody's story. A similar pattern was shown with education, with those who had no formal qualifications or General Certificate of Secondary Education or equivalent more likely to be influenced than those with a degree. Being influenced by Goody's story was not associated with marital status, ethnicity or screening status.
We ran a multivariate logistic regression including age, SEC and age of having first child. Although education was significant in univariate analyses we decided not to include this in the multivariate model to avoid multicollinearity (education and SEC were highly correlated). The model was significant (χ 2 (9) = 35.53, P < 0.001) explaining 6% of the variance in being influenced by Goody's story (Nagelkerke R 2 = 0.056). Age and SEC remained significant, as did age of having first child, although having first child at 16-19 years was no longer significantly different from the comparison group (possibly due to reduced power).
Discussion
In this population-based survey of women in England eligible for cervical screening, over a third felt that Jade Goody's story had influenced their decisions about cervical screening in the 18 months since her death. This proportion varied greatly by sociodemographic background, with around half of women in some subgroups reporting being influenced by the story, (e.g. 26-35-year olds and those with no formal education). Consistent with previous data from the national screening programme, women from younger age groups seemed to be most influenced by Goody's story.5,9 Having had children at a younger age was also associated with being influenced by Goody's story. One explanation for these women being particularly influenced by the story is that Goody herself was young (27 when she died) and had two young children. Previous studies have shown that narrative communication is most influential for those that are most similar to the celebrity or character in the story. 21
Women from lower SEC groups and with fewer educational qualifications were more likely to say they had been influenced by Goody's story. This contrasts with data showing no association between area-level deprivation and attendance at cervical screening in Wales after her death; 9 however, it is possible that area-level deprivation measures are too crude to identify fine-grained socioeconomic patterning. Goody was from a lower socioeconomic background herself, and so these groups of women may have identified with her more strongly. Alternatively, media coverage of the story was predominantly in sources read by lower socioeconomic groups, 8 so the SEC differences could be due to increased exposure. The finding that lower SEC women were more influenced by the story is encouraging, as there is higher incidence of cervical cancer in more deprived groups and this is partly explained by lower attendance at cervical screening.23,24 It can be difficult to engage these groups with interventions that aim to increase screening uptake 25 and studies have shown that narrative approaches can effectively increase screening participation among low SEC women. 26 The potential for narrative communication to decrease social inequalities in attendance should be explored further.
Although those working in health promotion do not control public exposure to celebrity cancer stories or the insertion of such story lines in television soap operas, certain aspects of narrative communication can be used in health promotion materials. However, this means of encouraging screening uptake may not be in line with the principles of informed decision-making. 27 One study found that clear public health messages were largely absent from media coverage of Goody's story. 7
There are also remaining questions about what exactly made Jade Goody's story influential. For example, it is not clear whether the narrative aspect of reporting was the important component or whether it was Goody's celebrity status that made her story easily accessible to women (availability heuristic). 28 In addition, Goody was a real person, not a fictional character, so her story may have been more influential than, for example, a soap opera storyline. It is also unclear whether reading about Goody's story once would have been as influential as the continued coverage that her story received.
Goody's publicist claimed that cervical screening had increased as a result of her experience, and although unsupported at the time, this attracted widespread publicity and became part of the narrative itself. Hearing that other women had attended screening because of Goody's story may have encouraged some to go for screening, either by setting the expectation that women should change their behaviour, or by increasing social norms.
There are limitations to this study. Firstly, the study is based on self-reported data, and we were unable to objectively assess whether participants’ screening behaviour had changed. We also did not specify what we meant by an ‘influence on their screening decisions’. For some women this may have been attendance when they were overdue for screening, for others this may have been prompt response to an invitation received. Although previous findings suggest that Goody's story encouraged women who were overdue for screening to attend, we did not find that screening status was associated with being influenced by Goody's story. Stratifying the sample by age to reflect different screening recommendations (26-49 years and 50-64 years) made no difference to the findings; screening status showed no association with self-reported influence in either group. Our measure assessed screening status at the time of the survey (18 months after Goody's death) rather than before exposure to the story, and this finding should therefore be interpreted with caution.
We embedded the question about influence of Goody's story in a large survey covering a range of topics, which should have reduced the likelihood of systematic participation biases. Although the survey was designed to be representative in the population, there was a quota sampling element to recruitment and no response rate is available, so it is difficult to ascertain whether these findings can be generalized to all women in England. Overall, only a small proportion of the variance was explained by the final model suggesting that although sociodemographics do play a role, there are other factors not considered here which are likely to be more important.
Conclusions
This paper adds to the evidence that the ‘Jade Goody Effect’, assessed using self-reported behaviour change, was more pronounced among young women, and suggests that her story also influenced screening decisions more markedly among those from lower socioeconomic backgrounds. Narrative communication may be one way to encourage cancer-protective behaviours and reach groups of the population that are difficult to reach using traditional intervention methods.