
Abstract
Objectives
To examine the relationship between cervical screening uptake and political engagement, and to test whether political engagement and voting behaviour mediate the association between age and cervical screening uptake
Setting
A population-based survey of women in England in 2010.
Methods
Women aged 26-64 took part in home-based computer-assisted interviews (n = 890). Women were classified as ‘up to date’ or ‘overdue/never been screened’ for cervical screening.
Results
Most women (81%) were up-to-date with screening; 19% were overdue. Age and marital status were associated with screening status. Women who were not registered to vote, had not voted in previous general elections, and those who showed less interest in elections and lower intention to engage in political activities were more likely to be overdue for screening. In multivariate analyses (adjusting for all significant measures) ‘being on the electoral register’ was the only significant independent predictor of screening status. ‘Being on the electoral register’ was also the only measure of voting behaviour that mediated the association between age and screening status.
Conclusion
We found limited evidence for the hypothesis that falling attendance for cervical screening could be associated with a broader phenomenon of disillusionment as indexed by reported voting behaviour and other measures of political engagement. Alternative explanations should be considered in order to better understand falling cervical screening uptake, particularly among younger women.
Introduction
Non-attendance at cervical screening appears to be associated with younger age, being single, having fewer formal educational qualifications and being from an ethnic minority background.1,3–5 It has also been associated with lack of awareness about cervical cancer screening, 6 emotional barriers to screening, such as anticipated embarrassment 4 and practical barriers (lack of time and difficulty getting appointments). 7 Fewer studies have considered explanations for the recent decline in uptake, particularly among younger women. One explanation is that younger women now face increased practical barriers making it difficult to translate their intentions to be screened into actions.7,8 An alternative explanation is that a broader disillusionment with public services has led to a decline in societal participation, not unique to cancer screening. The disillusionment hypothesis for explaining the recent decline in cervical cancer screening coverage was first suggested by Lancuck et al. 1 in 2008. Few studies have examined the association between participation in cervical screening and participation in other public services. Waller et al. 8 found that women who do not attend cervical screening are also less likely to vote. However, this association could be explained by a number of variables which were not explored, for example, being registered to vote (which is associated with living at a permanent address and with sociodemographic factors 9 ).
A voting intention survey, conducted by Ipsos-MORI, involving 10,211 adults in the UK 10 showed that intended turnout for the 2010 general election differed by age and social class. In particular, intended participation increased with age, with 73% of 55-64 year olds intending to vote, compared with 55% of 25-34 year olds. Three-quarters (76%) of men and women from the highest social class (AB) reported being ‘absolutely certain to vote’ or had already voted, compared with only 57% of those from the lowest social class (DE). The 2010 UK Electoral Commission research on public opinion after the election reported that, in addition to sociodemographic characteristics, factors associated with not voting included circumstantial reasons, particularly lack of time and being busy, not being registered to vote and negative attitudes towards politics (disliking politicians and politics). 11 The 2005 Electoral Commission research report on electoral registration in Britain showed that not being registered to vote was associated with low knowledge or misunderstandings of the registration process, particularly among young people, and knowledge was found to be lower among those already unenthusiastic about politics. 9 These results suggest that engagement and interest in politics and voting are important drivers of electoral registration and voter turnout.
The present study was designed to extend previous work, exploring in more detail the association between cervical screening status and political engagement using a range of measures adapted from the British Election Study. 12 We hypothesized that women who were not registered to vote or had not voted in previous elections, and those who showed less interest in general elections, less positive attitudes towards voting, and who did not intend to engage in other political activities would be more likely to be overdue for screening. This study was carried out four months after the UK general election in 2010, so we were able to measure recent voting behaviour. We also explored the role of sociodemographic factors as potential confounders of the screening and voting association. A further aim of this study was to examine whether voting behaviour and political engagement were mediators of the relationship between age and screening status. An understanding of the specific factors that influence women's attendance at cervical screening will inform interventions designed to increase uptake.
Methods
Data were collected over two waves of the TNS Research International omnibus survey in September 2010. In each wave of the survey, 2000 adults aged over 15 years living across the UK were recruited to take part in home-based interviews. Random location sampling was used to select 143 sample points across the UK from the 2001 Census small area statistics and the postcode address file. Sampling of locations was stratified by Government Office Region and social grade. At each location, quotas were set (for gender, working status and presence of children) to ensure a representative sample of adults.
Questions for the present study were asked of participants who were female, living in England and aged 26–64 years. Although women in England are invited for their first cervical screen at 25, we excluded 25 year olds to minimize the likelihood that women taking part had not yet been invited for screening. Data were collected using home-based computer-assisted personal interviewing.
Measures
Outcome Variable
Participation in cervical screening was assessed by asking women to choose the option that best described when they last had a smear/Pap test: tested within the last three years; last test was 3-5 years ago; last test was more than five years ago; never been invited; never had the test; had a hysterectomy; never heard of cervical screening. Women were re-classified into those whose screening status was ‘up to date’ (26-49 year olds screened in the last 3 years, or 50-64 year olds screened in the last 5 years) and those who were overdue or had never been screened.
Main Independent Variables (Voting Behaviour And Political Engagement)
Women indicated whether their name was on the electoral register (yes, no/do not know); whether they voted in the general election on 6 May 2010 (yes, no/do not know); and whether they voted in past elections (all or most; some, not very many or none of them). They also indicated their interest in the general election on 6 May 2010 (very interested, somewhat interested, not very interested, not at all interested). These measures were taken from the British Election Study. 12
Women answered four questions about engagement in future political activities responding on a 10-point scale (‘very unlikely’ to ‘very likely’). A principal components analysis was conducted on the correlations of the four items and yielded two components reflecting a ‘medium-level’ political engagement score (‘vote in the next local government council election’; ‘discuss politics with family or friends’) and a ‘high-level’ political engagement score (‘work for a party or a candidate in an election campaign’; ‘participate in a protest, like a rally or demonstration, to show concern about a public issue or problem.’). Mean scores were calculated for each subscale.
Women also indicated their agreement with six statements about their attitudes to voting in general, responding to each on a 5-point scale (‘strongly disagree’ to ‘strongly agree’): (a) ‘I feel a sense of satisfaction when I vote’; (b) ‘Most people around here usually vote in general elections’; (c) ‘When people like me vote, they can really change the way that Britain is governed’; (d) ‘Democracy only works if most people vote’; (e) ‘I would feel very guilty if I didn't vote in a general election’; (f) ‘I would be seriously neglecting my duty as a citizen if I didn't vote’. In a principal components analysis all six variables loaded onto one component and showed good internal reliability (alpha score of 0.83). A mean score of the six-item scale was calculated for each participant.
Demographic Variables
Women were asked to report their age; education; social class by occupation; marital status; working status; number of children; age of having first child and ethnicity.
Analysis
We used a series of univariate logistic regression models to explore associations between screening status and voting behaviour and political engagement measures. We then used multivariate logistic regression to explore the independent effects of all variables that were significant in univariate analyses. We also ran a bootstrapping analysis to examine whether voting measures (significant in univariate analysis), mediated the association between age and cervical screening uptake. Analyses were carried out using SPSS 19.0 (IBM, Chicago, IL, USA). Data were weighted by gender, region, social grade and age.
Results
Demographic Characteristics
Overall, 1031 women completed the survey. Women were mostly white (90%), married (68%) and employed (64%). The mean age was 44 years (SD = 10.6). Ten percent did not know or refused to answer the screening status question and 4% had had a hysterectomy. These women were excluded (n = 141) leaving a sample size of 890 women. Women who did not know or refused to answer the screening question were more likely to be from lower social grades (D and E) compared with women who answered the question (37% versus 20%, χ 2 (3) = 21.16, P < 0.001), were more likely to be non-white (25% versus 10%, x 2 (1) = 21.79, P < 0.001), and not working (57% versus 37%, χ 2 (1) = 14.67, P < 0.001). They were less likely to be on the electoral roll (77% versus 92%) (χ 2 (1) = 17.64, P< 0.001) but, surprisingly, they reported greater high-level political engagement (mean score = 3.14 versus 2.32) (t (954) = -2.87, P = 0.02).
Of the 890 women included in analyses, most had been for cervical screening within the last three years (74%) and an additional 17% had last been screened within the last 3-5 years. Among the remaining women, 6% had been screened before but not in the last five years, 1% said they had never been invited and 2% said they had been invited but never attended. Women were reclassified as ‘up to date’ (81%, n = 717) or ‘overdue/never screened’ (19%, n = 173).
Voting Behaviour And Engagement In Politics
Most women in the survey reported having their names on the electoral register (86%) with around two-thirds saying they voted in most or all general elections (66%). Fifty-eight percent of respondents reported interest in the 2010 general election and 67% reported voting in it, comparable with actual voter turnout in England for that election which was 65.5% overall (data are not available for women only). 13 We also compared self-reported turnout in this survey and estimated voter turnout by age and social grade reported by Ipsos-MORI. 10 Results were similar, with both reported and estimated turnout being higher in older women and among middle class groups.
Mean scores (on a 10-point scale) for engagement in future political activities were mid-range for ‘medium-level’ engagement (M = 5.78, SD = 3.09) and low for ‘high-level’ engagement (M = 2.37, SD = 2.22). Finally, we assessed level of agreement (on a 5-point scale) with a series of statements about attitudes to voting in general. The mean score for these six statements was 3.32 (SD = 0.85).
Predictors of Screening Status
Predictors of being overdue for cervical screening are shown in Table 1. Younger women (26-35 years) were more likely to be overdue for screening compared with women in the oldest age group (56-64 year olds) (24% versus 12%). Women who were single were also more likely to be overdue for screening compared with women who were married (29% versus 19%), whereas women who were separated, divorced or widowed were less likely to be overdue for screening compared with those who were married (11% versus 19%).
Predictors of being overdue for cervical screening
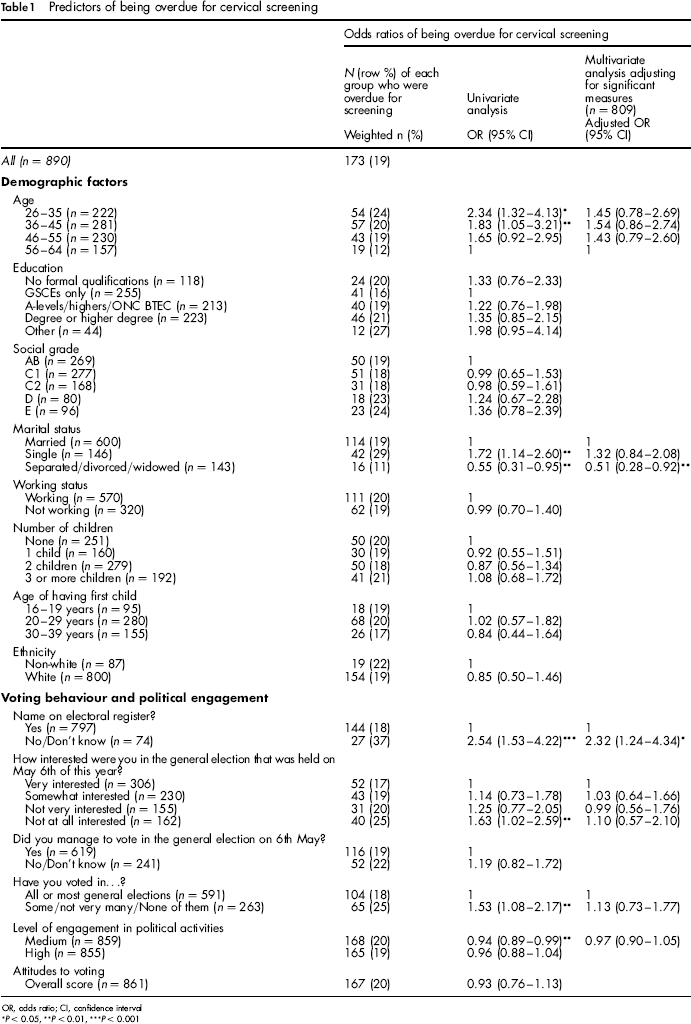
OR, odds ratio; CI, confidence interval
P < 0.05,
P < 0.01,
P < 0.001
Women who said their name was not on the electoral register, or who did not know if it was, were more likely to be overdue for cervical screening than women whose name was on the register (37% versus 18%). Women who reported they were not at all interested in the 2010 general election were more likely to be overdue for cervical screening than those who said they were very interested in the election (25% versus 17%), as were women who said they voted in only some or none of previous general elections compared with those who said they voted in all or most of previous elections (25% versus 18%).
Women who reported being likely to engage in political activities, such as voting in the next local government council election or discussing politics with family/friends were less likely to be overdue for screening than those who said they were not likely to engage in these activities (5.93 versus 5.30).
In a multivariate model adjusting for all significant variables, only one of the voting measures remained a significant predictor of screening status. As shown in Table 1, women who reported not being registered to vote were more likely to be overdue for screening (adjusted odds ratio: 2.32, 95% confidence interval [CI] 1.24-4.34, P = 0.009), compared with those who were on the electoral register.
Mediators of Age And Screening Association
Bootstrapping using syntax in SPSS 14 confirmed partial mediation of the association between age and screening status (parameter estimate = – 0.04, SE = 0.02, 95% CI -0.089 to -0.003, Nagelkerke R 2 = 0.0287), with an indirect effect for ‘electoral registration’ (parameter estimate = -0.02, SE = 0.01, 95% CI -0.054 to -0.005). No other voting or political engagement measures mediated the association between age and screening.
Discussion
This study examined predictors of self-reported cervical screening uptake among women in England. Consistent with the latest NHS cervical screening programme review, 15 age was associated with uptake, with screening attendance lowest in the youngest age groups. Marital status was also associated with screening status as has been found in other studies,4,16 with single women least likely to be up to date with screening. The finding that divorced, separated or widowed women were less likely to be overdue for screening compared with those who were married is, however, inconsistent with previous studies,4,17 and may require further investigation.
We explored the hypothesis that not attending for screening could be a marker of broader disillusionment using detailed measures of political engagement and self-reported voting behaviour. There was a robust association between being overdue for screening and not being on the electoral register. In addition, women who said they were not at all interested in the 2010 general election and those who reported not voting in many or any of the past general elections were more likely to be overdue for screening. We also found that those who reported being unlikely to engage in other political activities, such as discussing politics with friends/family or voting in local council elections were at higher odds of being overdue for screening.
In line with the suggestion by Lancuck et al., 1 lack of interest in the 2010 general election, non-registration and not voting in previous general elections was higher among younger women (26-35 years). However, level of engagement in other political activities and attitudes to voting did not vary with age.
In multivariate analysis, ‘being on the electoral register’ remained a significant predictor of screening status, with women who reported not having their name on the electoral register being more likely to be overdue for screening. Further analyses showed that the association between age and screening status was partially mediated by ‘being on the electoral register’. Age predicted whether or not women had their name on the electoral register, which in turn predicted screening status. This provides some limited support for the disillusionment hypothesis. Many of the measures of political engagement showed univariate associations with screening status, and the mediation analysis suggests that some of the variation in screening behaviour by age could be explained by more general disengagement, as indexed by not being on the electoral register.
However, other explanations for the associations found in this study are possible, for example, the increasing tendency for young people to live in privately rented accommodation, with private renters moving frequently could be one explanation. 18 Unstable tenure is likely to influence electoral registration: research after the May 2010 election showed that 13% of non-voters did not vote because of administrative factors, such as not being registered or not having received a polling card or postal vote. 11 Frequent changes in addresses may also affect being registered with the general practioner (GP) and receiving invitations for screening. It may therefore be that both not voting and non-attendance for screening are underpinned by practical factors associated with housing tenure rather than attitudinal factors like disillusionment.
Taken together, these findings provide limited support to the hypothesis that lower attendance at screening could be associated with a more general disillusionment. Rather than being less enthusiastic, younger women may perceive less benefit (or more barriers) of social and health actions, for example, registering to vote or going for screening, or they may simply move house more often and therefore be more likely to have out-of-date GP and voter registration. As suggested in our previous work, any apparent association with disillusionment may be explained by more practical constraints (e.g. lack of time or being too busy), rather than attitudes or beliefs. 7 Both registering to vote and attending for screening require a degree of organization and time management, and women who do not get round to register to vote might also be less likely to attend for screening. 8 Of course we acknowledge that some women make an informed choice not to attend for screening, and equally may decide not to vote. 7
To our knowledge, this is the first study describing the association between detailed measures of political engagement/voting and cervical screening uptake, and to examine whether these measures mediate the association between age and screening uptake. The study benefited from using a large national sample of women in the target age range (26–64 years).
This study had several limitations. First, most women in this survey reported that they had been for cervical screening within the last three years (74%) and an additional 17% had been screened within the last 3–5 years. The figure of 91% for 5 year coverage is substantially higher than the nationwide figure of 78.6%, 19 and indicates that women who do not attend regularly for screening were under-represented in our sample. 19 Second, data were collected using a quota sampling element, therefore, we had no information about non-responders and we cannot rule out the possibility of selection bias. Non-responders may have been less likely to attend regularly for screening. Third, a significant percentage of women (10%) did not know or refused to answer the screening status question and so they were excluded from the analysis. In addition, the measures of screening uptake and voting behaviour were based on self-report. Although the use of a range of social engagement measures (including voting and political engagement) constitutes a strength of the study, more work is needed to verify the validity of these measures. For instance, there was no evidence that attitudes to voting (e.g. ‘I feel a sense of satisfaction when I vote’) are associated with screening uptake. Other measures of general disillusionment with public services must be found if this line of inquiry is to be continued in future research. By focusing on political engagement, we were not able to measure other psychological constructs that have been found to predict screening participation, such as perceived benefits and risk perceptions.7,8,20–22
In conclusion, while being on the electoral register was associated with screening status in multivariate analyses, no other variables remained significant when adjusting for confounders. Therefore, the evidence of an association between political engagement and cervical screening attendance is limited. This study is important because it shows that the disillusionment hypothesis 1 is unlikely to be a key factor underlying the decline of cervical screening coverage among younger women. There is a need for further studies to explore alternative explanations for this phenomenon.