
Abstract
Objective
Despite premarital screening, prenatal diagnosis and the option for voluntary termination of pregnancy, some Iranian couples continue a pregnancy with a fetus affected with beta-thalassaemia major (β-TM). We examined the reasons for this decision, to evaluate the sociocultural challenges these couples face.
Methods
A retrospective evaluation of medical records of all fetuses aborted was conducted to identify those with β-TM, to determine the frequency of β-TM births and to establish the number of couples with β-thalassaemia who declined prenatal diagnosis or a termination of pregnancy in this period. We investigated the reasons for declining these options.
Results
The birth prevalence of β-TM decreased from 39.38 to 2.68 in 100,000 live births from 2005 to 2010. Terminations of pregnancy for affected fetuses increased from 67 in 2005 to 135 in 2010. We identified eight couples as β-thalassaemia carriers who declined prenatal diagnosis or a termination of pregnancy. All but one couple already had a child with β-TM. The reasons for declining prenatal diagnosis were strong religious beliefs, superstition and faith in a supernatural solution in six couples. Economic and cultural factors, and previous termination of pregnancy were also mentioned as reasons by the other two couples.
Conclusion
Although most of the couples had a β-TM child and related socioeconomic problems, their reasons for refusing prenatal diagnosis or termination remain a challenge for the healthcare system in Iran. Couple screening and educational programmes have effectively decreased the rates of refusal in at-risk couples in recent years.
INTRODUCTION
Thalassaemia is the most prevalent hereditary genetic disorder worldwide, and is especially prevalent in Iran, 1 with approximately 3,750,000 β-thalassaemia carriers, and 20,000 persons with a diagnosis of beta-thalassaaemia major (β-TM).
Premarital screening for β-thalassaemia started in 1991 locally in Shiraz, the capital of Fars province in southwestern Iran, and was extended to the entire Fars province in 1993, and to the entire country in 1996. Genetic screening and prenatal diagnosis for β-thalassaemia have been offered under the auspices of the Secretary for Treatment Affairs at the Ministry of Health and Medical Education since 1998, when a policy was initiated for voluntary termination of pregnancy for affected families. 2 Screening for β-thalassaemia in Iran currently includes premarital screening, genetic consultation and pedigree studies to identify family antecedents.
Increased levels of public knowledge, economic challenges faced by many families in our setting, and the inability to provide basic child care for infants and children with special needs, along with other related factors, can make therapeutic abortion an acceptable option for some families. However, despite increasing public awareness and a policy of support for voluntary termination of pregnancy through the public health-care service under certain circumstances (before 16 weeks of gestational age in Iran), some families opt to allow an affected pregnancy to continue to term.
We aimed to identify the sociocultural factors that affect the decision to decline a termination when prenatal diagnosis has identified a fetus affected with β-TM.
METHODS
We retrospectively evaluated the medical records of fetuses aborted during the years 2005–2010 inclusive, to identify those affected by β-TM. We also recorded the number and frequency of newborns affected with β-TM in this period.
Couples are identified as carriers of β-thalassaemia during the screening process for hereditary diseases. Once carriers are identified, they are offered prenatal diagnosis. All prospective parents who are carriers of β-thalassaemia in southern Iran are referred to the Hematology Research Center of Shiraz University of Medical Sciences in Shiraz, where genetic counselors explain the cause and symptoms of thalassaemia and the probability of disease transmission. Parents are given information about prenatal diagnosis and its procedures, risk factors and possible errors. An increased understanding of the disease helps families to make better decisions in relation to the preventive and support programmes. Written informed consent is obtained from each couple.
National beta-thalassaemia screening programme
To detect all couples at high risk of having a child with β-TM, the screening programme includes three strategies as follows:
In strategy 1, all couples who apply for a marriage license and who are diagnosed as having β-thalassaemia minor by the premarital screening test are referred for prenatal diagnosis. In strategy 2, parents who have children with β-TM are referred by specialist physicians for genetic counselling to their nearest regional haematology research centre. In strategy 3, couples with β-thalassaemia minor who were married before 1996 (when the nationwide premarital screening programme started) are referred to their nearest regional haematology research centre when the mother presents for her first prenatal care visit.
To obtain insight into the reasons for declining prenatal diagnosis or a termination of pregnancy, we interviewed couples who were carriers of β-thalassaemia who declined these options between 2005 and 2010. An ad hoc questionnaire solicited information about the parents’ age, the duration (in years) and status of their marriage, premarital screening, place of residence, parents’ employment, educational level, economic status, religion, number of pregnancies and terminations, number of living children with and without β-TM, and their reasons for declining prenatal diagnosis or a termination of pregnancy.
The data were analysed with SPSS v.15 software, and the results are presented as descriptive indices.
RESULTS
The trends in the frequency of β-TM births, aborted fetuses with β-TM, pregnancies in at-risk couples and declined the prenatal diagnosis or termination of pregnancy between 2005 and 2010 are shown in Figure 1. The frequency of β-TM births decreased from 27 in 2005 to two in 2010. The birth prevalence of β-TM decreased from 39.38 to 2.68 in 100,000 live births, and the frequency of terminations for affected fetuses increased from 67 in 2005 to 135 in 2010. The frequency of pregnancies in at-risk couples increased from 192 to 387. The number of refusals of prenatal diagnosis or termination of pregnancy decreased from two in 2005 to zero in 2010. The prevalence of refusal of these options in 1000 pregnancies among at-risk couples from 2005 to 2010 was: 10.41, 9.17, 7.57, 3.46, 2.98 and 0.
Frequency of thalassaemia major births, aborted fetuses, pregnancies in at-risk couples, and declined prenatal diagnosis (PND) or voluntary termination of pregnancy (VTP) during 2005–2010 in southern Iran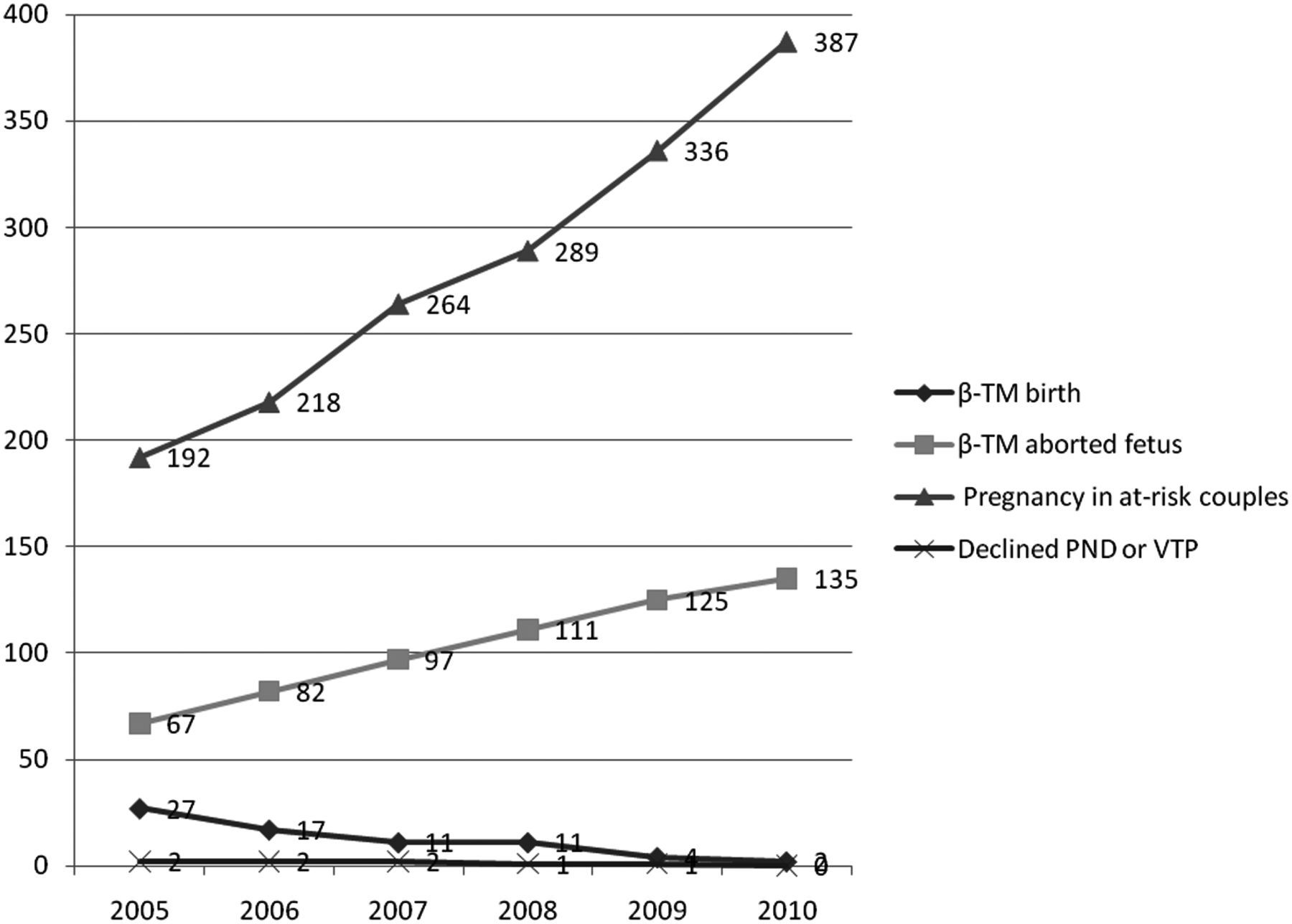
Eight couples were identified as carriers of β-thalassaemia who declined prenatal diagnosis or a termination after genetic counselling between 2005 and 2010. Their mean age was 41 ± 10 (range 24–56 years) for men and 32 ± 5 (range 26–43 years) for women. Five men had received education to the elementary school level, and the other three men had received education to the secondary school level. One of the women in this subsample was illiterate, five had received education to the elementary level and two had completed secondary education. All identified themselves as Muslims. Monthly income was about USD 300 for four couples, USD 300–420 for three couples, and USD 480 for one couple (exchange rates taken as at October 2010). All but one of the couples had a child with β-TM. Four couples had children all with β-TM, and three couples had both a child with β-TM and a healthy child. Four women had a history of between one and three terminations of pregnancy.
The decision to decline prenatal diagnosis or a termination of pregnancy was made by only one of the parents in two couples, and by both parents in six. Four couples refused prenatal diagnosis, and four couples refused a termination of pregnancy having been informed that the fetus was very likely to have β-TM. The reasons for declining were strong religious beliefs, superstition and faith in a supernatural solution in six couples. Economic and cultural factors as well as previous terminations were also mentioned as reasons by the other two couples.
DISCUSSION
We attempted to identify some of the sociocultural challenges faced by couples with β-thalassaemia when they are offered the option of a termination. As reported by Karimi and Jamalian, 3 our data showed that the frequency of β-TM births has declined since the implementation of premarital and prenatal screening programmes. The frequency of terminations of affected fetuses has increased as a result of the preventive screening programme for couples who are planning marriage, and increased knowledge in the general population. 3
Despite the implementation of these strategies, between 2005 and 2010 inclusive, 72 infants were born with β-TM in southern Iran. Some parents declined prenatal diagnosis or a termination for different sociocultural reasons. Some of the affected children were born for reasons related with ethical problems, and in some cases the parents did not request screening because of the questionable legality of the father's relationship with the mother. Some fetuses with β-TM were not detected, possibly as a result of false-negative laboratory results, or because of the lack of an accurate surveillance and follow-up system.
Improvements in public health-care delivery during the 20th century, and major developments in genetic science have contributed to gains in health status in societies. 4 Prevention is a preferable option compared with treatment, and preventive measures are resulting in decreasing mortality, morbidity and disease prevalence. In addition, prevention helps to create better economic welfare. 5 The therapeutic management of patients with β-TM is expensive, and blood transfusion remains the main treatment in these patients, but shortages of blood products, especially in developing countries, as well as the associated side-effects, are causes for concern. Only a few patients have an access to bone marrow transplantation. Gene therapy is not practicable yet and appears likely be expensive and not applicable to the general population. 6
Based on our results, although the number of pregnancies in at-risk couples has increased, β-TM births has decreased, and refusals of prenatal diagnosis or pregnancy termination are now restricted to only a few special cases. It seems that the preventive couple-screening programme, education programme and other related efforts in Iran have been successful in decreasing β-TM births. Higher educational level has been reported as an important factor to create positive attitudes toward prevention of thalassaemia. 7–9 In the present study all the couples we interviewed were from small towns and most of them had received education only to elementary school level. 10 More training about genetic testing and prenatal diagnosis is needed for general practitioners, as these health-care providers have a potentially positive impact on the patient's attitude to these options. 11
For all carriers of β-thalassaemia in Iran, public health insurance covers the cost of prenatal diagnosis, which is consequently free of charge. In contrast to studies in other countries, 12 the cost of the procedure is not a factor in the decision to decline prenatal diagnosis in Iran, although the socioeconomic status and income level were low for all of our participants.
Historically, abortion has not been allowed for Muslims, and legal exceptions are strictly regulated by directions issued by religious scholars, 13 who have decreed that abortion cannot be performed (except to save the mother's life) after the fourth month of gestation. 14
Seven of the eight couples we interviewed (87.5%) had a child with transfusion-dependent β-TM. Based on our results, the most frequent reasons for declining prenatal diagnosis or a termination of pregnancy were religious values, such as the belief in providence, and hope of a cure from God. 15 The other reason for declining these options in some women was the negative mental effects of previous terminations.
CONCLUSION
Religious beliefs, superstition and faith in a supernatural solution were the main factors that led couples affected by β-thalassaemia minor to decline prenatal diagnosis and the offer of a termination of pregnancy. Although these couples had a child with β-TM and had therefore already experienced the related socioeconomic problems, their reasons for refusing these options remain an important sociocultural challenge faced by the health-care system in Iran. Couple-screening and educational programmes have been effective in decreasing the prevalence of refusal among at-risk couples in the recent years.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the Shiraz University of Medical Sciences. We thank Shirin Parand at the Hematology Research Center, Nemazee Hospital in Shiraz, for editorial assistance, K Shashok (AuthorAID in the Eastern Mediterranean) for improving the use of English in the manuscript and Mojtaba Mahmoodi for administrative assistance.