
Abstract
Objective
To identify factors associated with a false-positive result in a population-based colorectal cancer (CRC) screening programme with the faecal occult blood test (FOBT) in Catalonia between 2000 and 2010.
Methods
The study population consisted of participants of the Catalan CRC screening programme with a positive FOBT who underwent a colonoscopy for diagnostic confirmation from 2000 to 2010. A false-positive result was defined as having a positive test but detecting no high-risk adenoma or cancer in the follow-up colonoscopy. Multivariate logistic regression models were performed to identify sociodemographic and screening variables related to false-positive results. Adjusted odds ratios (OR) and their 95% confidence intervals (CI) were estimated.
Results
Over the screening period, 1074 (1.7%) of the 63,332 screening tests had a positive result in the Catalan CRC screening programme. The false-positive proportion was 55.2% (n = 546). Women were more likely to have a positive FOBT in the absence of CRC neoplasia than men (adjusted OR = 2.91; 95% CI: 2.22–3.28). During the first prevalence round, the proportion of false-positive results was higher than in subsequent rounds (69.5% vs. 48.9%; P < 0.05). Re-screening and having a bleeding pathology such as haemorrhoids or anal fissures were also associated with a false-positive result.
Conclusion
The proportion of false-positive results and the associated risks should be estimated to provide an eligible population with more reliable information on the adverse effects of screening.
Introduction
Methods
Screening Procedure
A detailed description of the screening procedure is provided elsewhere. 8 Briefly, a biennial screening programme for CRC using the guaiac faecal occult blood test (gFOBT) was implemented in Hospitalet de Llobregat. The target population (average of 65,000 individuals per screening round) included men and women aged 50–69 years who lived in the L'Hospitalet de Llobregat (screening area). Demographic data on this population was gathered from the Primary Healthcare Information System. Subjects were excluded according to the following criteria: history of CRC, adenomas or inflammatory bowel disease, criteria for hereditary CRC syndromes, colonoscopy in the previous five years or FOBT within the last two years, moving out of the screening area, terminal disease and severe disabling conditions.
From the first to third rounds, gFOBT was used as the screening test (Hema-screenTM). In the fourth round, two tests were used, gFOBT and the immunochemical quantitative test (FIT) OC Sensor®. We compared both tests in terms of performance and participation in our screening population. 9 The gFOBT was offered to 50,227 individuals and the FIT to 12,707. Six faecal samples (two samples from three separate bowel movements) were required to complete a gFOBT whereas only one sample was needed for the FIT. The presence of faecal occult blood in five or six samples (or in any sample after retesting if 1 to 4 positive samples) and a haemoglobin level of ≥ 100 ng/mL were used to designate a positive FOBT result. All participants with a positive test result were advised to have colonoscopy. If no lesions were found in the colonoscopy those subjects would be invited for screening again after 10 years.
Study Population
The study population consisted of participants of the CRC screening programme with a positive FOBT who underwent a colonoscopy for diagnostic confirmation from 2000 to 2010 (n = 989). A false-positive result was defined as a positive FOBT but no detected high-risk adenoma or cancer in the follow-up colonoscopy. Because there is ongoing debate concerning the target lesion in colorectal cancer screening we also performed a sensitivity analysis to examine the effect that including adenomas of any size would have on false-positive rates in our CRC screening programme. 6
Data Collection And Analysis
The CRC screening programme information system included data on patient identification, age, sex, participation, appointment dates, screening test and colonoscopy results. We differentiated between initial and subsequent screening, and revised colonoscopy reports to identify sources of rectal bleeding such as haemorrhoids and anal fissures and severe complications during the diagnostic procedure (perforation, bleeding requiring transfusion, vagal syndrome or peritonitis-like syndrome).
Multivariate logistic regression models were performed to identify sociodemographic and screening variables associated with a false-positive result (0: true-positive result; 1: false-positive result). Adjusted odds ratios (OR) and their 95% CI were estimated.
Results
False-Positive Results in the Crc Screening Programme
Over the screening period, 1074 (1.7%) of the 63,332 screening tests had a positive result in the Catalan CRC screening programme. Our analysis was restricted to those individuals who underwent a colonoscopy (
The sensitivity analysis showed the effect of including any adenoma on false-positive rates. The overall proportion of false-positive results ranged from 55.2% (
False-positive results in CCR screening in Catalonia (Spain), 2000–2010
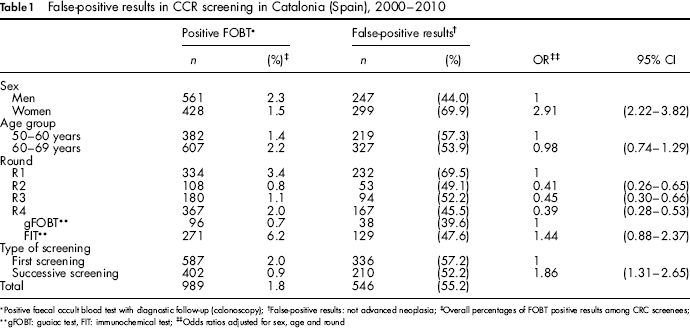
Positive faecal occult blood test with diagnostic follow-up (colonoscopy);
False-positive results: not advanced neoplasia;
Overall percentages of FOBT positive results among CRC screenees;
Odds ratios adjusted for sex, age and round
gFOBT: guaiac test, FIT: immunochemical test;
Sensitivity analysis: false-positive results in CCR screening in Catalonia (Spain), 2000–2010
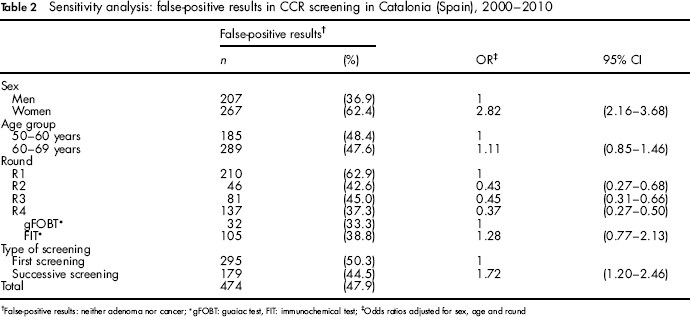
False-positive results: neither adenoma nor cancer;
gFOBT: guaiac test, FIT: immunochemical test;
Odds ratios adjusted for sex, age and round
Table 1 shows factors associated with false-positive results derived from multivariate analyses. The logistic regression models were adjusted for age, sex and round. Women were more likely to have a positive FOBT in the absence of CRC neoplasia than men (OR = 2.91; 95% CI: 2.22–3.28). No differences according to age were found.
During the first prevalence round, 69.5% of the participants with a positive FOBT had a negative colonoscopy result. Participants in subsequent rounds had on average 48.9% false-positive results (
In the fourth round, two screening strategies were compared (gFOBT and FIT). Among those individuals undergoing FIT, false-positive results were 8 percentage points higher than those who used the gFOBT, although the differences were not statistically significant.
Re-screening was associated with a false-positive result. Although the crude analysis suggested that a false-positive result was less likely in subsequent screenings than at first tests (52.2% vs. 57.2% of positive tests, respectively), after adjusting for potential confounding variables (age, sex and round) the direction of the effect was reversed from the crude estimate. Thus, those individuals who had previously participated in the CRC screening programme were more likely to have a false-positive result than those being initially screened (OR = 1.86; 95% CI: 1.31–2.65).
Factors Associated with Sex Differences in False-Positive Results
Table 3 shows the results from an analysis of factors associated with sex differences in false-positive results such as the screening strategy, haemorrhoids, anal fissures, menstrual bleeding or haemoglobin concentrations in blood. We reviewed the colonoscopy reports to determine whether the prevalence of bleeding pathology (haemorrhoids or anal fissures) could partly explain the sex differences in false-positive results. The prevalence of haemorrhoids and fissures among participants in our CRC screening was 24.5% (n = 242). Most of the screenees had only haemorrhoids (n = 239), both pathologies were reported in ten cases and finally anal fissures were identified in three individuals. Although having a bleeding pathology was a risk factor for false-positive results (sex-and age-adjusted OR: 1.84; 95% CI: 1.25–2.71), no sex differences regarding haemorrhoids and fissures were found (P = 0.96).
Potential factors associated with sex-differences among CRC screenees with a flase-positive result
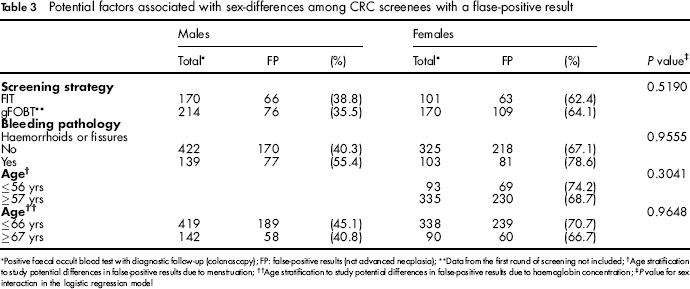
Positive faecal occult blood test with diagnostic follow-up (colonoscopy); FP: false-positive results (not advanced neoplasia);
Data from the first round of screening not included;
Age stratification to study potential differences in false-positive results due to menstruation;
Age stratification to study potential differences in false-positive results due to haemoglobin concentration;
Pvalue for sex interaction in the logistic regression model
We used age as a proxy indicator of menstrual bleeding and haemoglobin concentrations in blood, assuming that more than 97.5% of women at age 57 were already menopausal. 10 We also considered that ≥ 10 years after the menopause the blood haemoglobin concentrations in women became similar to that of age-matched men. 11 , 12 No differences according to any of the age groups were found.
Results from the sensitivity analysis were nearly identical (see Table 4).
Sensitivity analysis: potential factors associated with sex-differences among CRC screenees with a false-positive result
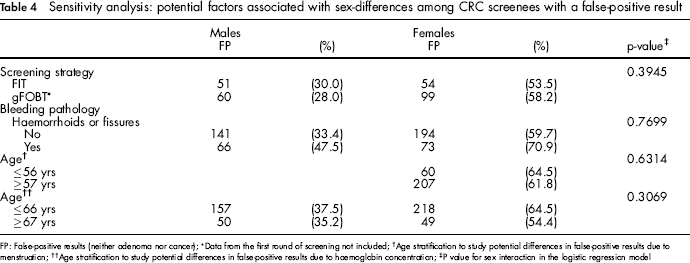
FP: False-positive results (neither adenoma nor cancer);
Data from the first round of screening not included;
Age stratification to study potential differences in false-positive results due to menstruation;
Age stratification to study potential differences in false-positive results due to haemoglobin concentration;
P value for sex interaction in the logistic regression model
Adverse Events After Colonoscopy
Through four screening rounds, the rate of severe complications after colonoscopy was 0.9%. Bowel perforation was reported in three cases and major bleeding was reported in six cases. All except one of these complications occurred in therapeutic colonoscopies following polypectomy.
Discussion
Half of the individuals with a positive FOBT had a negative finding on colonoscopy in our CRC screening programme. The first prevalent round produced a higher proportion of false-positive results. Although the screening programme is aimed at a healthy population, it is likely that in the first round some people with CRC symptoms or inflammatory bowel diseases were more likely to participate in the programme. A better selection of the eligible population in the subsequent rounds, in addition to the consolidation of the screening programme (leading to a better knowledge among health professionals and the target population) could be likely explanations for this finding. As has been found in other cancer screening programmes, 13 the risk of a false-positive result increased with successive screening participations. No statistically significant differences were found regarding the screening test, although the proportion of false-positive results with FIT was higher than with gFOBT, probably because FIT detects blood at lower concentrations than gFOBT. Whilst improved analytical specificity reduces false-positive tests from dietary blood, its increased analytical sensitivity means that small losses from inflammatory diseases or other physiological sources will bring new false-positives. 1 The more striking finding was the gender-differences in false-positive results. Women showed more than a twofold likelihood of a false-positive result than men. Menstrual bleeding and sex-differences in blood haemoglobin concentrations made little, if any, contribution to the false-positive results in our study population, because the effect was independent of age. A quarter of the screened individuals had haemorrhoids, but no differences by gender were found.
Potential interference of drug intake such as ant-iplatelet and anticoagulation therapy and nonsteroidal anti-inflammatory drugs (NSAIDs) on FOBT performance has been reported. 14 We did not collect information regarding medication in our screenees, although data from an unpublished study conducted among men and women aged 50–69 from the same screening area showed no statistical differences in the intake of NSAIDs in the overall group. However, women reported a significant higher intake of drugs for rheumatoid arthritis and osteoarthritis. Further research is needed to clarify the role of NSAIDS on false-positive results in order to recommend discontinuing NSAIDs, if clinically feasible, when collecting faecal samples.
There are no serious adverse health effects directly attributable to FOBT testing. The complications in a screening programme occur during follow-up of screened individuals with a positive test result, most of whom are disease-free. A high proportion of false-positive results leads to a number of unnecessary colonoscopies with associated costs and risks. Harm may arise from the preparation the patient undergoes before the procedure, the sedation used during the procedure, and the procedure itself. In randomized clinical trials, severe complications in FOBT screening programmes have been reported as 0.5% to 1.6%. 15 The relatively low rate of adverse events after colonoscopy 16 makes it difficult to differentiate acceptable from unacceptable incidence rates unless a large number of procedures are tracked over time. Another challenge is the accurate identification of those events presenting after dismissal from the endoscopy unit. 14 Late complications may still be underestimated because of under-reporting.
Our study has several limitations: firstly, the estimated proportion of false-positive results could be biased although the adherence to those individuals adequately refered to colonoscopy among screen-positive individuals was quite high (93.7%).
Secondly, even though colonoscopy is the most reliable method available to date for assessing presence of colorectal neoplasms, it is not perfect, and missed adenomas at colonoscopy might have led to some overestimation of false-positive rates of the FOBTs. 17
Thirdly, data concerning the follow-up of people with a false-positive result was not available at the time of the analysis. Follow-up data should be collected to identify interval cancers and to estimate the likelihood of testing positive again. Some studies suggested that the risk of CRC among individuals with a prior negative colonoscopy is very low for up to 20 years or longer. 18 , 19 The prevalence of advanced adenomas has also been reported to be very low for several years after a negative colonoscopy. 20 , 21 However, those studies estimated risk of CRC following a negative colonoscopy performed among average-risk people. In a recently published paper, Brenner et al. showed an association between interval cancers and the performance of the preceding colonoscopy due to a positive FOBT (adjusted OR = 2.93; 95% CI: 1.13–7.61). 22 Individuals aged under 60 when the false-positive result occurred will be invited to CRC screening 10 years after their false-positive result. Those individuals may have an increased likelihood of testing positive 10 years after the prior positive result. For example, haemorrhoids are a common condition in the target age range for CRC screening. Because this condition is often persistent, individuals with haemorrhoids who once tested positive at FOBT may also have a higher likelihood of receiving another positive result if they continue with FOBT. 23
Fourthly, we could not collect prospective data regarding potential factors associated with gender differences in false-positive results.
Finally, the study could not evaluate the adverse psychological effects associated with a false-positive result. To our knowledge only three studies to date have assessed the concern of screened individuals with a false-positive result.24–26 Parker and colleagues measured anxiety scores in 100 gFOBT-positive individuals and found that these were highest after notification of a positive gFOBT and before investigation by colonoscopy. In patients with false-positive results, scores fell the day after colonoscopy and remained low one month later. In general cancer screening programmes, anxiety, distress and depression symptoms can be reduced by a brief orientation programme at the clinic visit.
In conclusion, the large gender differences in false-positive results was the most remarkable finding and merits more research. In addition, the proportion of false-positive results and the associated risks should be estimated to provide eligible populations with more reliable information on the adverse effects of screening.