
Abstract
Objectives
The NHS bowel screening programme offers people aged 60–69 screening by faecal occult blood (FOB) testing, with colonoscopy as the diagnostic test. This paper describes the calculation of targets for the purpose of monitoring screening performance in the programme.
Methods
Targets were calculated for the prevalent round of screening in people aged 60–69, and for the ‘steady state’ of the programme when people will be offered their first screen at age 60 and subsequent screens at ages 62–69. Targets for the cancer and adenoma detection rates per 1000 people screened and per 100 colonoscopies were calculated using information from the English bowel cancer screening pilot.
Results
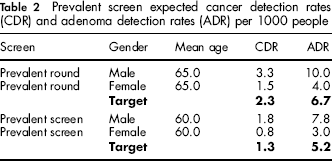
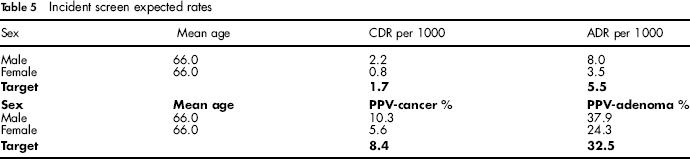
For the prevalent round, prevalent screen and incident screens the calculated targets for the cancer detection rate are 2.3, 1.3 and 1.7 per 1000 people respectively. For the adenoma detection rate the targets are 6.7, 5.2 and 5.5 per 1000 respectively. Targets for the cancer detection rate per 100 colonoscopies are 11.3, 7.5 and 8.4 and those for the adenoma detection rate are 32.0, 30.4 and 32.5 respectively.
Conclusions
The purpose of these targets is to ensure that the national bowel cancer screening programme is effective with a high quality of screening. The cancer detection and adenoma detection rates per 1000 people are those estimated to be necessary to achieve the expected mortality reduction. Rates per 100 colonoscopies (equivalent to the positive predictive value of referral to colonoscopy) are designed to maintain a high quality of screening by minimizing the number of false-positive referrals.
Introduction
Screening by faecal occult blood testing has been shown by randomized controlled trials (RCTs) to reduce mortality from bowel cancer. 2 Following these trials, in particular the Nottingham RCT, 3 a pilot study was conducted in England covering parts of Warwickshire, Coventry and Rugby to examine the feasibility of population screening. 4 , 5
Ideally, targets for the NHS BCSP for detection rates of cancer and adenoma per 1000 people screened would be calculated from the Nottingham trial, with the inference that if the targets are met an equivalent mortality reduction is likely to be achieved. However, use of the trial data for this purpose was found to be limited by the small numbers in individual age and gender subgroups. The larger numbers available in the English pilot (approximately three times the numbers in each age-gender subgroup) have therefore been used to determine expected rates in specific age-gender subgroups. This is considered a reasonable compromise because the protocol for the pilot (and that for the BCSP) was similar to that of the Nottingham RCT, even though the pilot itself was not designed to study outcome in terms of bowel cancer mortality. The Nottingham RCT demonstrated a 15% reduction in colorectal cancer mortality with an uptake of 60% in people aged 45 to 74 at entry.
The targets referred to in this paper are the standard detection rate expected for a screening centre or colonoscopist. Currently used figures are published by the NHS BCSP. 6
Methods
This paper considers four targets:
the cancer detection rate per 1000 people screened (CDR) the adenoma detection rate per 1000 people screened (ADR) the cancer detection rate per 100 colonoscopies (PPV-C) the adenoma detection rate per 100 colonoscopies (PPV-A).
The latter two measures are equivalent to the positive predictive values (PPVs) of colonoscopy for cancer (PPV-C) and for adenoma (PPV-A) respectively.
Each target has been calculated for the initial prevalent round of screening and for prevalent and incident (subsequent) screens when the programme is in a steady state, giving a total of 12 target values.
During the introduction of the screening programme, the whole population throughout the age range 60–69 will be invited (the ‘prevalent round’); these first prevalent screens will therefore occur at a mean age of approximately 65.0 years. Following the prevalent round the screening programme will enter a ‘steady state’ in which the first (prevalent) screens will occur at age 60 and subsequent (incident) screens between the ages of 62.0 and 69.9 (with an approximate mean age of 66.0).
Prevalent round and prevalent screen targets were therefore estimated from the prevalent round (round 1) of the English pilot for people aged 60–69 years and 60 years respectively, and incident screen targets using data from rounds 2 and 3 of the English pilot for people aged 62–69 previously screened with a negative result. Data on the numbers of adequate screens and adenomas and cancers detected stratified by gender and age and screening round were obtained from the English Pilot database held by the Cancer Screening Evaluation Unit at the Institute of Cancer Research, London.
Targets were calculated by fitting a logistic regression model to the data (using STATA version 10), with cancers or adenomas detected as the dependent variable, age as a continuous variable and sex as a categorical variable. This allows greater flexibility than the use of observed age-specific detection rates, as it allows the calculation of targets for any age within the 60–69-year age groups and with caution marginally outside this age range. The models could therefore be used to estimate revised targets as the age range of people invited by the NHS BCSP is extended.
We assumed, based on results from the English pilot, that 45% of people screened are male and that 60% of colonoscopies are in men. If these proportions vary, standardized targets by gender can be calculated for the CDR (or ADR) using ‘direct’ standardization as 0.45 x CDR (or ADR) per 1000 men + 0.55 x CDR (or ADR) per 1000 women and for PPV as (0.6 x PPV% in men + 0.4 x PPV% in women). This method of standardization is particularly useful if the numbers of men and women are sufficient to obtain a reliable estimate for each gender. Direct standardization has been used, which preserves the original target value but is subject to instability if numbers in any of the age or gender strata are small.
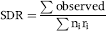
As an alternative, indirect standardization can be used to calculate a standardized detection ratio (SDR), which is the ratio of the observed to expected numbers of cancers or adenomas. This method is valid with small numbers in each strata; the target is now always 1.0.
The general formula is:
Results
Prevalent Round And Steady State Prevalent Screen Targets
Table 1 shows the outcomes of the prevalent screen from the English pilot.
Prevalent (first) screen outcomes from the English pilot

The expected prevalent screen adenoma detection rate per 1000 people at ages 60 to 69 is estimated from the logistic regression model fitted to the data in Table 1 as:

The prevalent screen target is calculated using a mean age of 60.0, giving an expected rate of 7.8 per 1000 for men and 3.0 per 1000 for women. The target is then 0.45 × 7.8 + 0.55 × 3.0 = 5.2 per 1000 people screened.
For the cancer detection rate per 1000 people screened the fitted model is:

The prevalent round and prevalent screen expected rates per 1000 people are shown in Table 2.
Prevalent screen expected cancer detection rates (CDR) and adenoma detection rates (ADR) per 1000 people
For the prevalent screen adenoma detection rate per 100 colonoscopies (PPV-A) the fitted model is:

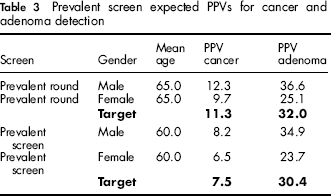
Estimated rates for men and women aged 60 are 34.9% and 23.7% respectively, and the target is therefore 0.6 × 34.9 + 0.4 × 23.7 = 30.4.
Similar calculations can be made for the cancer detection rate per 100 colonoscopies (PPV-C) where the expected can be calculated as:

The prevalent round and prevalent screen expected rates per 100 colonoscopies are shown in Table 3.
Prevalent screen expected PPVs for cancer and adenoma detection
Incident Screen Targets
The incident screen expected rates can be calculated as follows using the raw data shown in Table 4. Again gender takes on the value of 1 for men and 0 for women. Adenoma detection rate per 1000 people as:

Incident (subsequent) screen outcomes from the English pilot

Cancer detection rate per 1000 people as:

Adenoma detection rate per 100 colonoscopies as:

Cancer detection rate per 100 colonoscopies as:

The incident screen expected rates are shown in Table 5.
Incident screen expected rates
Age And Gender Standardization
As an example, consider a colonoscopist undertaking 1000 procedures at incident screens where 90% (900) of procedures were on women. If the adenoma detection rate was 28% (252/900) in women and 40% (40/100) in men then the crude PPV-A will be 29.2% (292/1000), which is below the target of 32.5. However, the gender standardized PPV, GS-PPV-A standardized to 60% male and 40% female = 0.6 × 40 + 0.4 × 28 = 35.2%, which is above the target.
Table 6 shows the use of indirect standardization for both age and gender on the PPV-A at incident screens for 1000 colonoscopies with a higher-than-average proportion of female patients. The number of procedures in each strata is multiplied by the expected rate to obtain the expected numbers. As these are incident screens the mean age in the 60–64-year age group is estimated to be 63.5 (midway between 62.0 and 64.9) and the mean age in the 65–69-year group to be 67.5. The expected number for each age-gender group is calculated from the formula:

Example standardized detection ratio for PPV-adenoma (based on data from 1000 colonoscopies of which 320 persons have adenoma detected)
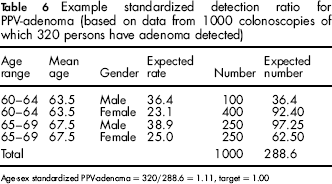
Age-sex standardized PPV-adenoma = 320/288.6 = 1.11, target = 1.00
Discussion
This paper describes the calculations underlying the target adenoma and cancer detection rates from prevalent and incident screens in the NHS BCSP, and considers techniques for age and sex standardization. The reasons for setting targets need to be made clear. Firstly, the targets for ADR and CDR rates per 1000 people screened are those estimated as necessary for the programme to achieve a mortality reduction of a similar level to that observed in the Nottingham trial. In contrast, the primary purpose of the target PPV values is to measure colonoscopist or screening centre performance and the quality of service delivery. A high-quality screening programme is one that delivers a high ADR and CDR detection rate per 1000 people with a high PPV, thus ensuring as few people as possible are unnecessarily referred to colonoscopy at the same time as achieving a high mortality reduction.
We have based the target values on data from the English pilot because of the small numbers in some subgroups in the Nottingham trial. Data from the English pilot can provide estimates for any age or gender group between 60 and 69 to enable age-gender standardized rates to be calculated. The models assume no interaction between age and sex and a term fitted in the model to test for interaction was not significant. There were some important differences between the English pilot study and the Nottingham trial. In particular the pilot study had a much lower PPV than the Nottingham trial, but a much higher positivity rate. Initial results from the NHS BCSP suggest a positivity rate much closer to the English pilot suggesting the use of the English pilot study for setting targets is appropriate. There are also similarities in uptake and population characteristics between the English pilot and Nottingham trial. Uptake of the first round of the pilot in England was 58.5% compared with 57.9% in the Nottingham trial. Uptake of screening in the second round was also similar. 4 This also suggests that using data from the pilot is appropriate to set targets with the aim of achieving a mortality reduction of a similar magnitude to that achieved by the Nottingham trial in people aged 60–69.
When setting targets we are often as interested in the relative performance between centres and individuals as much as the absolute performance and this becomes increasingly true the further in time we move from the start of the programme. With increasing time there is increasing uncertainty over the estimation of the background incidence in the absence of screening. In this paper we have assumed that the background incidence rate in the English Pilot area (Coventry, Warwickshire & Rugby) is similar to that in England as a whole. However, in the pilot, 3 it was observed that the incidence rates in West Midlands were higher than those for England, and in a further paper we will consider the use of background incidence correction factors. The calculations also assume that that the risk in the non-responder and responder groups in the NHS BCSP is the same as that for the English pilot. In the pilot, the incidence rate in the non-responders was lower than that in the general population. Overall the uptake in the NHS BCSP is similar to that in the pilot, but if there were significant variations in uptake the effect of selection bias should be considered.
The NHS BCSP in common with the other national screening programmes in cervical and breast cancer screening is constantly being amended. The programme has recently extended the upper age limit to 74 and the calculations in this paper could be extended to cover that age range.
The target values calculated in this paper should help the NHS bowel screening programme establish and maintain a high quality of screening. It is recommended that each of these targets is re-visited as national screening programme data become available, and that age-sex standardized targets for cancer and adenoma (SDR measures) be considered along with the production of background incidence correction figures. A similar process took place for the breast cancer screening targets 7 within a few years of the start of the programme. A recent development in bowel screening is that a one-off flexible sigmoidoscopy will soon be offered to people at age 55 and people will be able to request such screening up to their 60th birthday. Although it will be a few years before this screening is rolled out, it will have a major impact on expected rates and require a revision of the targets.
In screening it is particularly important to closely monitor and evaluate the performance of the population programme after its inception following evidence from RCTs. The goal of performance measurement in screening is to help continually help maximize the benefit from screening and minimize the harm.