
Abstract
Objective
To compare the effectiveness of first trimester, second trimester, and integrated screening for Down's syndrome.
Setting
Two prenatal diagnosis centres in China.
Methods
A total of 11,966 pregnant women (≥18 years) were screened over 21 months. First trimester screening (11–13 weeks) comprised measurement of serum free beta-human chorionic gonadotrophin (β-hCG) and pregnancy-associated protein-A concentrations, and fetal nuchal translucency thickness. Second trimester screening (15–20 weeks) comprised measurement of β-hCG and alpha fetoprotein concentrations. Computer software was used to calculate the risk of carrying a Down's syndrome fetus.
Results
The overall incidence of Down's syndrome was 0.2% (23/11,966). When the false-positive rate was fixed at 5%, detection rates for first trimester, second trimester, and integrated screening were 73.9%, 69.6%, and 82.6%, respectively. When the false-positive rate was fixed at 3%, detection/sensitivity rates for first trimester, second trimester, and integrated screening were 65.2%, 56.5%, and 73.9%, respectively.
Conclusions
These findings suggest that integrated screening was the most effective means of screening for Down's syndrome in a Chinese population.
Introduction
Prenatal screening for DS is characterized by maternal age, timing (first trimester, second trimester, or integrated), and the choice of markers assessed. First trimester DS screening typically involves the measurement of nuchal translucency (NT) thickness by ultrasound, combined with assessment of maternal serum free beta-human chorionic gonadotrophin (β-hCG) and pregnancy-associated protein-A (PAPP-A) concentrations. 2 Second trimester DS screening typically involves the assessment of maternal serum β-hCG, alphafetoprotein (AFP), unconjugated oestriol (triple screening), and inhibin A (quadruple screening) concentrations 3 or the assessment of β-hCG and AFP (double screening) concentrations in some countries, including China. 4 , 5 Integrated screening involves performing assessments during both the first and second trimester and thereafter assessing DS risk. 3 , 6 Integrated screening has been reported to be associated with the highest DS detection rates (88% to 96%; 2% to 5% false-positive rates),6–9 followed by first trimester screening (85% to 94%; 3% to 5% false-positive rates),6,7,10 and then second trimester quadruple (81% to 85%; 5% to 6% false-positive rates) 6 , 7 and triple (69% to 85%; 5% to 9% false-positive rates) 6 , 7 screening. Second trimester double screening, commonly employed in China, has been reported to be associated with a detection rate of 60%. 4
There is room for optimization in DS screening. It is also important to note that there may be ethnic differences in concentrations of maternal serum markers assessed in DS screening; 11 hence, regional studies are essential. Few studies to date have reported on DS screening in China, and no study has reported on the results on integrated screening for DS in China. Hence, the aim of this study was to examine and compare the effectiveness of first trimester, second trimester, and integrated screening for DS in mainland China. First trimester combined and second trimester double screening was performed.
Methods
Study Design And Participants
This study took place from March 2009 to December 2010 and involved consecutively presenting pregnant women. The study protocol was approved by the Institutional Review Boards of Jiaxing University College of Medicine and The Second People's Hospital of Wenzhou. All participants provided written informed consent.
Pregnant women aged ≥ 18 years who underwent prenatal examination at Center of Prenatal Diagnosis, Maternity and Child Health Care Hospital or Center of Prenatal Diagnosis, the Second People's Hospital were eligible for inclusion in the study. Pregnant women were excluded from the study if they were: aged >35 years and had received amniocentesis or cordocentesis in the absence of measurement of serum markers; screened in the first trimester only; smokers; or diabetics. Women with non-singleton pregnancies, fetuses with hydroma, and those who had had previous DS births were also excluded. After a diagnostic test, women continued their pregnancies, with counselling offered to parents in the case of an affected pregnancy.
Study Protocol
Sampling And Sample Analysis
Venous blood (2 mL) was collected from participants between weeks 11 and 13 (first trimester) and between weeks 15 and 20 (second trimester) of gestation. Gestational age was calculated according to each participant's last menstrual period. For participants who could not provide the time of their last menstrual period or who had irregular menstrual cycles, ultrasonography was performed in the first trimester to measure fetal crown-rump length and biparietal diameter, to determine gestational age. Serum was isolated at room temperature and stored at -20 °C for measurement of free β-hCG (first and second trimester), PAPP-A (first trimester), and AFP (second trimester) by dissociation-enhanced lanthanide fluorescence immunoassay (DELFIA1235: Perkin Elmer, Waltham, MA). Fetal NT thickness was measured during the first trimester using ultrasound (2–5 mHz). Measurements were made by three trained physicians (note: these physicians were not Fetal Medicine Foundation trained in assessing fetal NT thickness). Values for β-hCG, PAPP-A, NT, and AFP are presented as multiples of the median (MoM) and were determined by normalizing the obtained value to the corresponding normal median value for the appropriate gestational age using data obtained from nearly 20,000 local Chinese women who underwent prenatal examinations at our institutions from March 2009 to January 2012.
MoM values were calculated as follows: first, for unaffected pregnancies, the relationship between gestational age and the median marker level at the corresponding gestational age was determined by generating equations using log-linear regression. Second, the marker levels were transformed to MoM values by dividing the medians at the corresponding gestational age. Finally, the MoM values were further corrected for weight by generating equations using log-linear or reciprocal regression analyses. The MoM values were used for risk analysis calculations.
Down'S Syndrome Risk Analysis
The standardized MoM values were compared with the known distributions in affected and unaffected pregnancies in order to calculate the likelihood ratio and the modified risk of an affected pregnancy. Analysis was performed using Wallace LifeCycleTM Elipse analysis software (Perkin Elmer) to determine the risk of carrying a fetus with DS in the first trimester and second trimester. The integrated risk (both trimesters) was also determined.
Women classified as having a high risk of carrying a fetus with DS were referred to genetic counsellors and offered amniocentesis (weeks 19 to 21 of gestation) or cordocentesis (weeks 22 to 28 of gestation) for cytogenetic analysis to confirm or rule out DS. Amniocentesis and cordocentesis were optional; participants provided informed consent before undergoing either procedure.
Participants at high risk who opted not to undergo amniocentesis or cordocentesis, and those at low risk, were followed up by examining medical records and/or by telephone interview to determine the outcome of pregnancy.
Statistical Analysis
Continuous variables are summarized as median and inter-quartile range (the range between the 25th and 75th percentile) and were compared between the DS and non-DS groups by non-parametric Mann-Whitney test. Detection rates with 95% confidence intervals (CI) were calculated for fixed false-positive rates of 3% and 5%. A P value less than 0.05 was considered to be statistically significant. All analyses were performed using SPSS 15.0 statistical software (SPSS Inc, Chicago, IL).
Results
Participant Characteristics
A total of 11,966 pregnant women completed first and second trimester screening tests for DS during the study period and were included in the study. The median maternal age was 26.7 and the overall incidence of DS was 0.2% (23/11,966). Women who gave birth to children with DS were significantly older than women who gave birth to children who did not have DS (Table 1). Women who gave birth to children with DS also had significantly higher β-hCG (P < 0.001) and NT (P < 0.001) at the first trimester assessment, and significantly lower AFP MoM values (P = 0.043) and higher β-hCG at the second trimester assessment (P < 0.001) compared with women who gave birth to children who did not have DS.
Characteristics of women who gave birth to children who did and did not have Down's syndrome
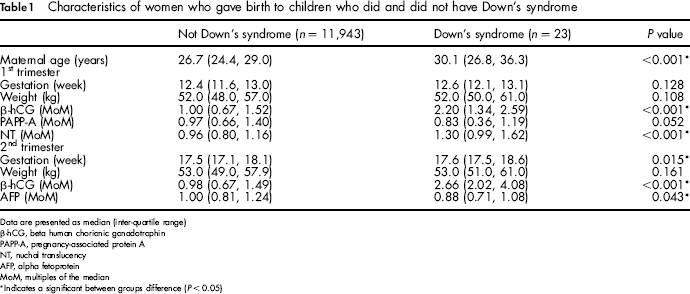
Data are presented as median (inter-quartile range)
β-hCG, beta human chorionic gonadotrophin
PAPP-A, pregnancy-associated protein A
NT, nuchal translucency
AFP, alpha fetoprotein
MoM, multiples of the median
Indicates a significant between groups difference (P < 0.05)
With the false-positive rate fixed at 3%, integrated screening had the highest detection rate (73.9%), followed by first trimester screening (65.2%), and second trimester screening (56.5%). With the false-positive rate fixed at 5%, integrated screening had the highest detection rate (82.6%), followed by first trimester screening (73.9%), and second trimester screening (69.6%) (Table 2).
Detection rates for specified false-positive rates for each screening method
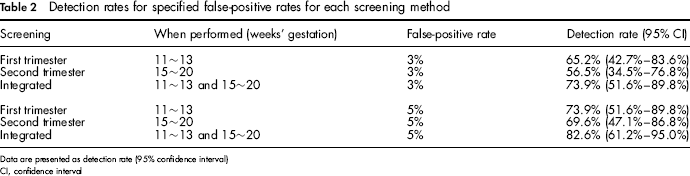
Data are presented as detection rate (95% confidence interval)
CI, confidence interval
Discussion
This is the first study to compare the effectiveness of first trimester combined, second trimester double, and integrated screening for DS in China. We found that integrated (first and second trimester) screening yielded the highest DS detection rate when false-positive rates were fixed at 3% or 5%. Detection rates were ≥69.6% for all three types of screening when the false-positive rate was set at 5%. Second trimester screening yielded a low DS detection rate when the false-positive rate was set at 3%.
Our finding, that integrated screening (first trimester combined and second trimester double) yields relatively high DS detection rates, is consistent with previous reports describing the results of large-scale studies involving Caucasian women in which detection rates ranged from 88% to 95%.6–9 Similarly, previous studies comparing screening approaches have also found that integrated screening yields higher detection rates than first and/or second trimester screening.6–9
First trimester DS detection rates (85% to 90%) in previous studies involving Caucasian women have been slightly lower than detection rates for integrated screening,6,7,10 but higher than the first trimester detection rates in our study (73.9% at a 5% false-positive rate and 65.2% at a 3% false-positive rate). We believe the seemingly lower DS detection rates in our study may be more a reflection of the small number of DS pregnancies in our cohort. Indeed, the upper limit of the 95% confidence interval for first trimester screening in our study was 89.8% for a false positive rate of 5%. An alternative, but less likely, explanation is that the low DS detection rates for first trimester combined screening may be a consequence of ethnic differences between Chinese and Caucasian populations. 11 Continued monitoring is needed to determine whether our findings are simply a reflection of the small number of DS pregnancies or if ethnicity is important in this context.
Our second trimester double screening detection rate of 69.6% (5% false-positive rate) is lower than previously reported second trimester quadruple rates, and comparable with previously reported triple screening detection rates for studies with similar false-positive rates involving Caucasian women. 6 , 7 By contrast, our double screening detection rate of 69.6% is higher than rates reported in previous studies examining second trimester double screening in Chinese women (50 to 60%). 4 , 5 The explanation for a seemingly higher detection rate in the present study is unclear, and we are continuing to monitor the results of second trimester double screening for DS to confirm whether the detection rate reported is real or a statistical anomaly. It is worth noting that we found that the second trimester double screening detection rate was markedly lower (56.5%) when the false-positive rate was fixed at 3.0%.
Our study has several limitations. Firstly, this was a single institution study, and the findings may not therefore be generalizable to other regions of China. Secondly, the level of expertise in the assessment of NT thickness may not have been sufficient in our study, thus reducing the accuracy of the first trimester and integrated screening results. Integrated screening, and NT thickness assessment, was introduced relatively recently (March 2009) at our institution. Given that technical expertise is critical for the accurate assessment of NT thickness, 12 the assessments performed by the relatively inexperienced personnel at our institution may have been less reliable than those performed at other institutions where the technique is well established and performed by experienced personnel. Indeed, in settings where the accuracy of NT thickness assessment cannot be assured (the case in much of China), serological screening should be performed for both test accuracy and cost reasons. Many physicians in China prefer second trimester serological screening for these reasons. Further studies are needed to clarify the effectiveness of first trimester, second trimester, and integrated screening for DS in China, particularly as physicians become more familiar with and skilled at performing NT thickness assessments.
In conclusion, our findings suggest that integrated screening is the most effective means of screening for DS in China, followed by first trimester combined screening. We believe that studies such as ours are important and necessary for the optimization of DS screening in developing countries such as China, where the balance between financial cost/benefit to the patient and screening effectiveness may be of more concern than in Western countries.