
Abstract
Objective
Cancer screening guidelines often include discussion about the unintended negative consequences of routine screening. This prospective study examined effects of false-positive mammography results on women's adherence to subsequent breast cancer screening and psychological well-being. We also assessed whether barriers to screening exacerbated the effects of false-positive results.
Methods
We conducted secondary analyses of data from telephone interviews and medical claims records for 2406 insured women. The primary outcome was adherence to screening guidelines, defined as adherent (10–14 months), delayed (15–34 months), or no subsequent mammogram on record.
Results
About 8% of women reported that their most recent screening mammograms produced false-positive results. In the absence of self-reported advice from their physicians to be screened, women were more likely to have no subsequent mammograms on record if they received false-positive results than if they received normal results (18% vs. 7%, OR = 3.17, 95% CI = 1.30, 7.70). Receipt of false-positive results was not associated with this outcome for women who said their physicians had advised regular screening in the past year (7% vs. 10%, OR = 0.74, 95% CI = 0.38, 1.45). False-positive results were associated with greater breast cancer worry (P < .01), thinking more about the benefits of screening (P < .001), and belief that abnormal test results do not mean women have cancer (P < .01), regardless of physicians' screening recommendations.
Conclusion
False-positive mammography results, coupled with reports that women's physicians did not advise regular screening, could lead to non-adherence to future screening. Abnormal mammograms that do not result in cancer diagnoses are opportunities for physicians to stress the importance of regular screening.
INTRODUCTION
Among United States (U.S.) women who receive regular breast cancer screening over 10 years, an estimated 50% 1 to 63% 2 can expect to receive false-positive mammography results one or more times. Estimates for European screening programmes are lower but still substantial, likely reflecting different screening guidelines and definitions of abnormality. 3–5 Understanding how false-positive results affect subsequent screening behavior and psychological well-being is important, as reflected in the evolution of breast cancer screening guidelines, which now consider potential risks and benefits.
Previous research shows that false-positive mammography results can affect adherence to routine breast cancer screening, although findings vary by geographic region, according to our meta-analysis. 6 In the USA, women who received false-positive results were slightly more likely to return for subsequent mammography screening compared with women whose results were normal. 7,8 Studies conducted in European countries generally found no significant effect of false-positives on return for mammography screening, 9,10 although the European trend has been towards a slightly lower return rate for women with false-positives. 11–15 Canadian studies also suggest a negative effect of false-positives on subsequent mammography screening. 16,17
In addition to potential non-adherence to subsequent screening, false-positive results cause small but reliable increases in breast cancer-specific worry and perceptions of breast cancer risk. 6,18 Some studies found that these effects persisted months and even years after cancer was ruled out. 11,19 The U.S. Preventive Service Task Force's most recent report on breast cancer screening cited psychological distress associated with false-positives as one reason for shifting screening guidelines from an annual to biennial schedule, beginning at age 50. 20
The last U.S. study to directly address the question of whether false-positives influenced women's return for subsequent mammography screening was published in 2003, 8 several years before widespread debate emerged on health-care reform. It is possible that behaviors surrounding mammography have changed since that time. The primary goal of our analyses was to examine how false-positive results affect future mammography screening and beliefs.
Furthermore, our conceptual work suggests that some conditions known to discourage screening may exacerbate the negative influence of false-positive results. 21 We hypothesized that false-positive results would have more effect on future screening for women who had fewer financial resources or said their physicians had not advised them to go for regular screening. Women who receive false-positive results often are faced with follow-up testing charges. 22 For women of limited means, fear of incurring such charges again could potentially inhibit subsequent routine screening. Women with false-positive results whose physicians have not advised them to have mammograms also could be at risk for non-adherence to future screening. Physicians are important sources of information for women contemplating the benefits and risks of screening; 23,24 their recommendations for screening may be particularly important for women who receive false-positive results.
METHODS
The Institutional Review Boards for the University of North Carolina at Chapel Hill and Duke University approved the study. We present secondary data from PRISM (Personally Relevant Information about Screening Mammography), a four-year, National Institute of Health-funded, randomized controlled intervention trial to increase sustained adherence to mammography screening. For ethical reasons, all women received PRISM study interventions consisting of several kinds of reminders and, for some, individually-tailored telephone counselling. 25
Participants
PRISM study enrollment occurred between October 2004 and April 2005. Researchers identified potential participants through the North Carolina Teachers' and State Employees' Comprehensive Major Medical Plan, also known as the State Health Plan (SHP). The sample included North Carolina female residents who were between the ages of 40 and 75, enrolled with the SHP for two or more years prior to sampling, and had recent mammograms.
Following consent, women completed 30-minute baseline telephone interviews that assessed mammography-related beliefs and practices. Subsequent telephone interviews occurred at 12, 24, 36 and 42 months. Women who completed 36-month telephone interviews, conducted between 2007 and 2008, comprised the analytic sample for this study, because only these interviews included key study variables (see Figure 1). Women not reached for 12- or 24-month interviews were still eligible to participate in 36-month interviews. PRISM researchers received monthly claims information from the SHP with dates of women's mammograms; claims data were used to calculate the adherence outcome.

Data collection timing and source
The 36-month telephone interviews included 2979 women who had not previously received breast cancer diagnoses. We excluded data for women who had not had mammograms in the last 14 months (n = 358), were no longer members of the SHP (n = 160), and for whom records to confirm subsequent mammography screening were not available, or had a breast cancer diagnosis subsequent to their interviews (n = 55), suggesting their abnormal test results were ‘true positives’. The final analytic sample included 2406 women from all intervention arms. Preliminary analyses showed that intervention arm was not associated with receipt of a recent false-positive result.
Measures
Test result: Women reported results of their most recent screening mammograms (false-positive or normal) during study interviews. The SHP medical claims system provided information on women's mammography dates, but not test results. We defined ‘recent’ as occurring within 14 months prior to the 36-month interview. The survey item read: ‘Since we last spoke, have you had a mammogram when you were told the results were not normal, but no cancer was found?’ Previous research indicates that self-report of abnormal mammography results corresponds highly to medical records, 26 though accuracy may be lower for minority and low-education groups. 27
Adherence: The primary outcome measure was adherence to subsequent mammography screening, assessed using screening mammography dates obtained through SHP claims information and verified through self-reports for most women (see Figure 1). We classified women into three categories:
Adherent to subsequent screening (within 10–14 months of last screening); Received subsequent but delayed mammogram (within 15–34 months), or; Had no subsequent mammogram on record for our data collection period.
The lower boundary of 10 months excluded most diagnostic and short-interval rescreening mammograms. The upper boundary of 14 months reflects American Cancer Society recommendations for yearly mammograms with a two-month window for scheduling. 28 At the time of the study, women who received false-positive mammography results typically were advised to return for regular screening one year from the date of the screening exam that produced the abnormal result. 29
Women's beliefs about themselves: The first of two items to assess breast cancer-specific worry was: ‘Having yearly mammograms causes you worry or anxiety about breast cancer.’ A 4-point response scale ranged from ‘strongly agree’ to ‘strongly disagree’. The second item read: ‘How worried are you about getting breast cancer in your lifetime?’ A 5-point response scale ranged from ‘not at all’ to ‘a great deal’. We summed responses to create a single continuous measure that ranged from 2 to 9, with higher scores indicating more breast cancer worry. One item assessed perceptions of breast cancer risk: ‘How likely are you to get breast cancer in your lifetime compared with the average woman your age and risk?’ Response options were ‘less likely’, ‘about as likely’ and ‘more likely’ (coded 1–3). Thought about the benefits of mammography read: ‘In the past week, how often have you thought about the benefits you can gain by getting a mammogram when you are due?’ A 4-point response scale ranged from ‘none of the time’ to ‘most of the time’ (coded 1–4).
Women's beliefs about the test: We assessed perceptions of mammography accuracy through two items. The first read: ‘How often do you think an abnormal mammogram result means a woman has breast cancer?’ A 4-point response scale ranged from ‘rarely’ to ‘always’ (coded 1–4). The second item asked ‘How much do you trust mammograms to give accurate information about whether you have breast cancer?’ A four-point response scale ranged from ‘not at all’ to ‘completely’ (coded 1–4). One item assessed perceived effectiveness of mammography: ‘Thinking of women your age and race, how effective are mammograms for reducing deaths from breast cancer?’ A 4-point response scale ranged from ‘very ineffective’ to ‘very effective’ (coded 1–4).
Barriers to screening: The survey also assessed cost barriers and women's reports of whether their physicians had advised them to have mammograms. The item for cost as a barrier, taken from a list of reasons why women delayed mammograms, read: ‘The cost of the mammogram: do you agree or disagree that this could delay your getting a mammogram?’ A 4-point response scale ranged from ‘strongly agree’ to ‘strongly disagree’. Due to low frequency of some response categories, we created a dichotomous variable to reflect whether costs were a barrier to future screening (a response other than ‘strongly disagree’ = Yes). The survey item to assess physician recommendation for mammograms read: ‘In the last year, has a doctor advised you to have a mammogram?’ This item has been used repeatedly in mammography studies. 23,24
Data analyses
All analyses controlled for physician recommendations and receipt of previous false-positive results, factors associated with women's recent test results (see Table 1). We used generalized logits model analyses for multinominal outcomes to examine the association of recent test results (explanatory variable) with the three-level adherence to subsequent screening variable. 30 These analyses compared women adherent to subsequent screening with those who either received delayed mammograms or had no subsequent screening, adjusting for control variables (Table 2). We tested for moderation by including interaction terms in separate models. We examined the association of recent test results (explanatory variable) with women's thoughts about themselves and the test using separate multivariable regression models, adjusting for control variables (Table 3). We conducted all analyses using SAS v9.1.3. Tests were two-tailed, using a critical alpha of .05.
Demographic and medical characteristics of the sample
Notes: We do not report Hispanic ethnicity due to low frequencies; 1 P value is for comparison of Whites with Blacks
Adherence to subsequent mammography screening
Associations between false-positive status and women's thoughts about themselves and the screening test
*P < .01; ** P < .001
RESULTS
Women's mean age was 55 years (Table 1). The majority of women were white (88%), married (79%), and college-educated (65%). Few women (15%) reported that costs could delay having their next mammograms; 30% reported their physicians did not advise them to have mammograms in the past year. About 8% of women (184/2406) reported false-positive results on their recent screening mammograms. About one-half of women (51%) reported ever receiving previous false-positive results, not including recent false-positives.
Subsequent mammography screening
Overall, 9% (217/2406) of women did not have any subsequent screening mammograms on record, 16% (395/2406) received subsequent mammograms that were delayed, and 75% (1794/2406) were adherent to subsequent screening (Table 2). Proportions of women who had no subsequent screenings on record were similar for the false-positive and normal mammogram result groups (9% for both groups, OR = 1.09, 95% CI = 0.65, 1.86). However, women who reported recent false-positives were slightly more likely to have delayed subsequent mammograms compared with women whose recent results were normal (22% vs. 16%, OR = 1.50, 95% CI = 1.03, 2.18).
Effect of recent false-positive mammography results on adherence to subsequent screening was conditional upon receipt of a physician's recommendation for mammography screening. The interaction applied only to the comparison of women who did not have records of subsequent mammograms with those who were adherent (P = .01 for interaction). Among women who said their physicians had not advised them to have mammograms, those who received false-positive results were more likely to have no subsequent mammograms on record compared with women who received normal test results (18% vs. 7%, OR = 3.17, 95% CI = 1.30, 7.70) (Figure 2). However, among women who reported their physicians advised them to go for screening, proportions of women who had no subsequent mammogram on record were similar for the false-positive and normal test result groups (7% vs. 10%, OR = 0.74, 95% CI = 0.38, 1.45). Effect of false-positives on subsequent screening did not vary by whether women reported cost barriers to screening (P = .69 for interaction).
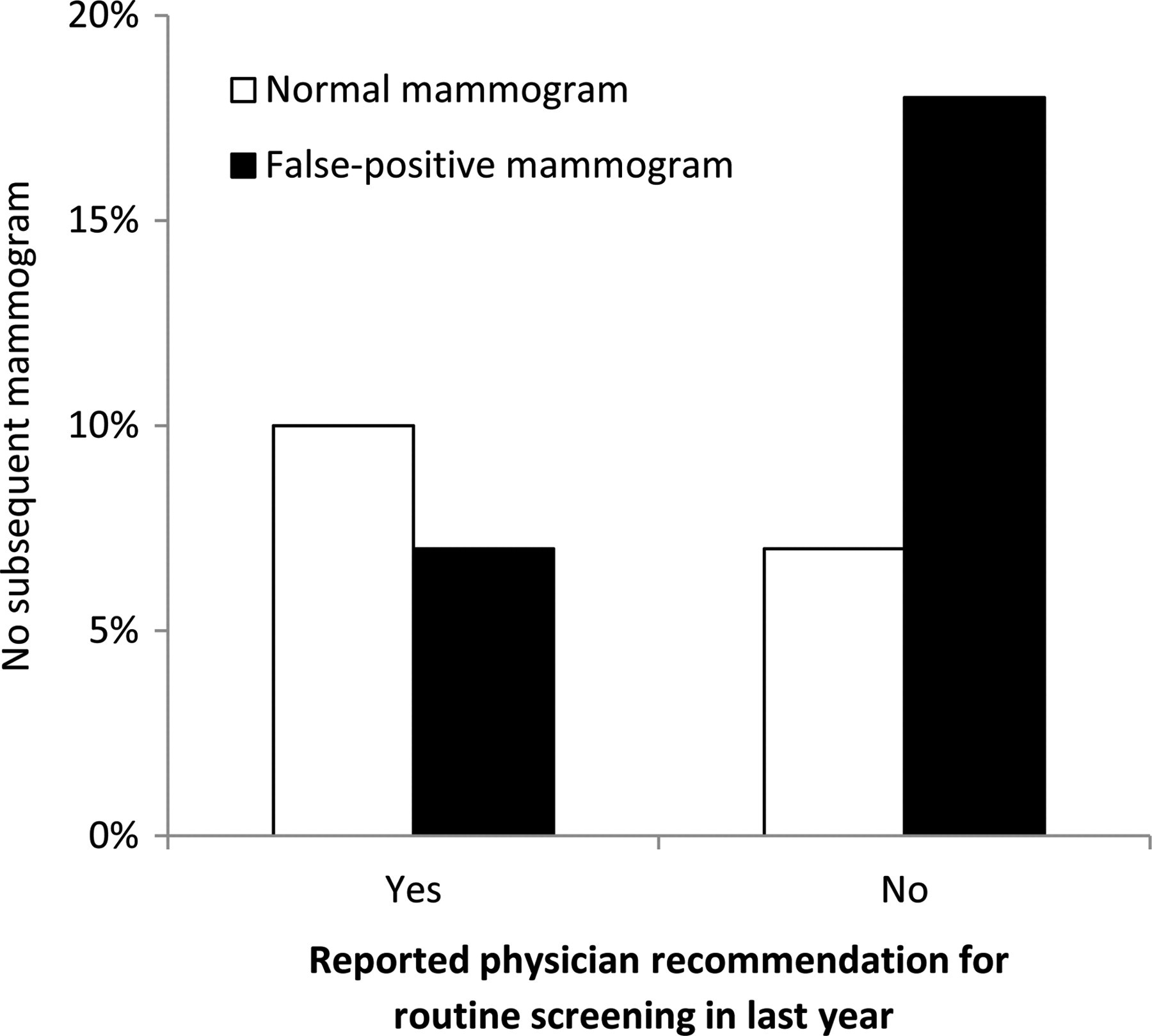
Impact of false-positive mammogram results on subsequent screening
Women's thoughts and beliefs
Compared with women whose mammography results were normal, women who received recent false-positive results had more breast cancer worry (P < .01), spent more time thinking about the benefits of regular mammography (P < .001), and believed abnormal test results were less likely to mean there was cancer (P < .01) (Table 3). None of these variables were associated with adherence to subsequent screening (all P > .05) nor was their association with false-positive results moderated by physician recommendations (all P > .05).
DISCUSSION
Consistent with national estimates, 1,2 our study found that over one-half of women reported ever receiving false-positive results on screening mammograms; 8% reported that their most recent mammograms were false-positives. While adherence to subsequent, annual screening was high for women in this study, those whose recent mammograms produced false-positive results were slightly more likely to delay subsequent screening mammograms compared with women whose recent mammograms were normal. Many women who reported false-positive results and said their doctors had not advised them to have mammograms for routine screening did not return at all. Other U.S. studies have shown that false-positives either had no effect on 31–33 or seemed to facilitate subsequent mammography use. 7,8 Our findings are more consistent with two Canadian 16,17 and several European studies 11–15 showing that false-positive results interfere with subsequent screening. Given controversy concerning the benefits and potential harms of mammography screening, 20 monitoring the effects of false-positive test results and whether physicians advise women to be screened should remain a public health priority.
It is possible that our findings more closely resemble those from European studies due to the way appointments are scheduled and paid for. Many European countries have mammography screening programmes that automatically schedule women for appointments and send reminders. These programmes require women to ‘opt-out’ of mammography screening should they choose not to attend. In the U.S. women must ‘opt-in’ to undergo regular screening; no national programme automatically invites women to attend regular mammography screening although there have been studies in which such approaches have resulted in increased screening rates. 34 In essence, PRISM created an ‘opt-out’ programme for study participants similar to that of European systems. Researchers sent PRISM participants annual reminders for their mammograms (although women's appointments were not pre-scheduled) and followed up with women who delayed screening. Also, like women enrolled in some European screening programmes, most mammography costs for PRISM participants were covered by insurance. It is possible that our study's ‘opt-out’ system may have encouraged women to consider their options more extensively, which in this case may have meant decreased screening among women with false-positives.
Another possible explanation for lower screening rates may be the slight downward trend in mammography in the U.S. 35 Perhaps for women in our study, who were already receiving regular mammograms, the false-positive experience could have created or exacerbated mammography fatigue. We did not have sufficient numbers of women with false-positives to conduct more fine-grained analyses to elucidate this possibility.
Among women who reported their physicians had not advised them to have mammograms in the past year, rates of return for subsequent screening were lower for women who received false-positive results, a finding that has not been documented previously in the screening literature. About 18% of women who received false-positive results and reported they were not advised by their physicians to have mammograms did not return for subsequent screening. Since physician recommendations are one of the strongest predictors of routine mammography screening, 23–24 it is not surprising that physicians' recommendations buffered negative effects for women who received false-positive reports. Abnormal mammograms that do not result in a cancer diagnosis are opportunities for physicians to stress the importance of regular screening. Women who report not receiving this advice could be at risk for not returning for future screening. Although we might expect that most patients and physicians communicate about the benefits and harms of breast cancer screening following false-positive experiences, few women report having such conversations. 36 Missed opportunities for women to discuss false-positive results with their physicians may be partly a function of the way health care is organized in the U.S. today, where test results may come directly from radiologists or other clinicians, and women may not see their physicians for another year after their test results.
Women who reported false-positive results were more worried about breast cancer, a finding well-documented in the research literature. 6,18 Research suggests that immediate follow-up and reading of test results can greatly reduce women's anxieties after abnormal mammograms. 37 However, same-day follow-up for abnormal test results is an uncommon practice, partly because many clinics require that mammograms be read by two radiologists. Clinics that cannot offer same-day services might consider providing women with printed or electronic information about the recall process 38 or with counselling from trained staff to answer questions and address benefits and potential harms of regular mammography screening. 39
Women in this study who received false-positive results spent more time thinking about the benefits of having regular mammograms, such as the possibility for early detection and feeling ‘peace of mind’ when results are normal. Thinking about the positive aspects of regular screening may serve as an effective coping response for women who receive false-positives, counterbalancing worry or anxiety elicited by test results. Women who received false-positive results in this study were slightly less likely to believe that an abnormal mammogram result meant they had breast cancer, which is appropriate given their recent false-positive experiences.
Strengths of the study include insurance coverage for all women, access to health claims records for identifying women's mammography dates, a large sample from a defined population, and the longitudinal study design. Limitations include that we did not have access to medical records to determine which mammograms were false-positives and had to rely on self-reports. Research shows that self-report can be an accurate method of determining whether women had false-positive screening results, 26 and the false-positive rate for recent mammograms in this study (8%) was very similar to national averages. 1,2 Information provided by the SHP did not differentiate screening from diagnostic or follow-up mammograms. To address this issue, and consistent with standard research practices, we excluded mammograms that occurred within 10 months of previous mammograms as we deemed them likely to be diagnostic or follow-up. Some women may have been advised to return for screening at six-month intervals after receiving false-positives. Thus, it is possible that some women classified as adherent to subsequent annual screening may have returned for second, short-interval (6-month) mammograms. Finally, all PRISM participants received study interventions, which may have diminished effects of false-positives on women's beliefs and behaviors. Sensitivity analyses suggest that the influence of false-positives on study outcomes was similar across PRISM intervention arms.
Our findings suggest that false-positive mammography results, coupled with women's reports that their physicians had not advised them to have mammograms, could lead to non-adherence to future screening. Gynaecologists, primary care physicians and their staff members are important sources of information about breast cancer screening and are well-positioned to provide advice and reassurance after false-positive results and strong, unequivocal recommendations about future mammograms. 23–24 In situations in which women may not see their providers for months after abnormal test results are resolved, it is important that record systems cue health-care providers to refer back to the abnormal result at the next visit. While it is not known if our findings are unique to the U.S., they may offer insights for more effective management of mammography screening in other countries that promote regular screening. For patients who have had false-positives, the effectiveness of interventions for communicating about the balance of potential harms and benefits of regular screening is an important area for future research in both the U.S. and abroad.
Funding
Funding for this research comes from the UNC Cancer Care and Quality Training Program (NCI R25 Grant, CA116339) and the American Cancer Society (MSRG-06-259-01-CPPB). PRISM was supported by National Cancer Institute grant 5R01CA105786.