
Abstract
Objective
To estimate the pre-eclampsia screening performance of placental growth factor (PlGF) and endoglin with second-trimester Quadruple test markers used for antenatal Down's syndrome screening.
Methods
A nested case-control study of 88 pregnant women with known early second-trimester Down's syndrome Quadruple test marker levels who subsequently developed pre-eclampsia and 275 unaffected controls. Frozen maternal serum samples were thawed and assayed for PlGF and endoglin. Monte Carlo simulation was used to estimate the pre-eclampsia screening performance of a pre-eclampsia detection algorithm using the Quadruple test markers with or without the addition of PlGF and/or endoglin.
Results
Median PlGF was 33% lower (95% confidence interval 24–41%) and endoglin 31% (20–43%) higher in pre-eclampsia than in unaffected pregnancies. Adding PlGF to the Quadruple test markers increased the pre-eclampsia detection rate from 34% to 45% at a 5% false-positive rate – it increased it to 43% with endoglin and to 50% with both. The corresponding estimates for early pre-eclampsia (before 36 weeks’ gestation) were a few percentage points higher (48%, 48% and 55% respectively). Including information on parity, pre-eclampsia in a previous pregnancy, family history (woman's mother) and assuming a pre-eclampsia prevalence of 2%, the detection rates for a 5% false-positive rate were 39% with the Quadruple test markers, 48% with addition of endoglin, 49% with addition of PlGF, and 54% with addition of both.
Conclusions
Adding PlGF to the Quadruple test Down's syndrome screening markers improves pre-eclampsia screening performance. There is a modest extra benefit in also adding the measurement of endoglin.
Introduction
Of the antiangiogenic soluble receptor components, endoglin has been shown to be the most useful in predicting the development of pre-eclampsia, being, on average, 21% higher in women who develop pre-eclampsia compared with women who do not. 5 PlGF has also been shown to be useful, being on average 40% lower in women who develop pre-eclampsia compared with women who do not. 5
We here combine early second-trimester PlGF and endoglin values with second-trimester serum markers for Down's syndrome (alphafetoprotein [AFP], unconjugated oestriol [uE3], human chorionic gonadotrophin [hCG] [total or free β] and inhibin-A) to assess the pre-eclampsia screening performance of combinations of these markers.
Methods
We used a previously described dataset and stored early second-trimester serum samples relating to clinically confirmed pre-eclampsia (either [i] eclamptic fits, and/or [ii] raised blood pressure after 20 weeks, but not before, based on diastolic blood pressure ≥ 90 mmHg on two occasions at least one day apart, together with urinary proteinuria based on 24h urinary protein excretion ≥500 mg or at least two ‘abnormal’ spot urine tests classified as at least ‘++’ on different days) and five controls for each case (matched according to gestational age [within the same week], calendar quarter, age [+ 2 years], parity [nulliparous or multiparous] and ethnicity) 2 for which Ethics Committee approval was obtained. Second trimester serum markers for Down's syndrome had been measured as part of our previous study. On grounds of economy, three of the five controls matched to each of the original 96 cases were randomly selected for assay. Serum samples were retrieved, thawed and there were sufficient sera available for assay in 88 of the 96 pre-eclampsia pregnancies and 275 of the 288 controls. Samples were assayed for endoglin using the Quantikine® Human Endoglin/CD105 Immunoassay and for placental growth factor using the Quantikine® Human PlGF Immunoassay (both R&D Systems® Europe, Ltd). The samples were assayed ‘blind’ i.e. without knowledge of whether the samples were from an affected (pre-eclampsia) or unaffected pregnancy.
Endoglin and PlGF concentrations were expressed as multiples of the median (MoM) for unaffected pregnancies of the same gestational age. This was done by performing a regression of the log median marker concentration against median gestational age in each completed week of gestation (weighted by the number of women in each week). Each observed concentration was then divided by the regressed (i.e. expected) concentration for the same gestational age to obtain the MoM value. MoM values were then adjusted for maternal weight by performing a regression of the log median MoM values against median weight in categories of weight (weighted by the number of women in the category) and dividing MoM values by the regressed value for the same weight. Probability plots and, if appropriate, the approximate point of risk reversal (to ensure risk estimation is a monotonic function of the marker value 6 )were used to specify truncation limits within which the range of values for both endoglin and PlGF approximately followed log-Gaussian distributions in affected and unaffected pregnancies.
The log median endoglin and PlGF MoM values were used as the measure of central tendency to avoid the influence of outliers. Standard deviations (log) were calculated by regression of the points on the probability plots between the 10th and 90th centiles and correlation coefficients were calculated after excluding points more than 3.5 standard deviations away from the log median. Log means and standard deviations of the Down's syndrome screening markers and correlation coefficients for the Quadruple test markers from our previous study were revised as a result of correcting for maternal weight, which was not previously done. 2
Monte Carlo simulation used these Gaussian distributions to generate hypothetical random samples of 100,000 pregnancies which would develop pre-eclampsia and 100,000 unaffected pregnancies. For each pregnancy the odds of having a pregnancy that would develop pre-eclampsia was calculated by multiplying the prior odds (prevalence of pre-eclampsia, expressed as an odds) by the likelihood ratio (for a given set of marker values) obtained from the Gaussian distributions of marker levels in affected and unaffected pregnancies, taking account of correlations between markers. A woman was classified as screen positive if her risk of having a pregnancy with pre-eclampsia was greater than or equal to a specified risk cut-off level. Screening performance estimates were calculated as the detection rate (DR) of all pre-eclampsia for false-positive rates (FPR) of 5 and 10%. Estimates of screening performance were obtained for (i) all pre-eclampsia, (ii) early pre-eclampsia (before 36 weeks’ gestation) and (iii) late pre-eclampsia. To avoid producing two separate risk estimates (one for early and one for late) the screening performance for early pre-eclampsia was based on simulating a population of pregnancies using the early pre-eclampsia distribution parameters but the risk cut-offs were based on all pre-eclampsia pregnancies. Similarly, the screening performance for late pre-eclampsia was based on simulating a population of pregnancies using the late pre-eclampsia distribution parameters but the risk cut-offs were based on all pre-eclampsia pregnancies.
Estimates for all pre-eclampsia were also derived using information on parity, family history (whether mother of the pregnant woman had pre-eclampsia) and using information on whether a previous pregnancy was affected by pre-eclampsia. The latter was done in two ways, one in which women with a previous pregnancy with pre-eclampsia were considered positive, and the remaining women receive serum screening, and another in which all women receive serum screening and a previous history of pre-eclampsia contributed to the risk estimate. The modification of risk estimates using these factors were based on a previously reported meta-analysis which showed that women are 7.2 (95% confidence interval [CI] 5.9 to 8.8) times more likely to develop pre-eclampsia in a current pregnancy if they had pre-eclampsia in a previous pregnancy compared with women who had not had pre-eclampsia in a previous pregnancy (a rounded estimate of 7 used; in a previous publication this was incorrectly stated to be relative to women who had not had pre-eclampsia in a previous pregnancy and women who had not previously been pregnant 2 but it should be just women who had not had pre-eclampsia in a previous pregnancy), nulliparous women are 2.91 (95% CI 1.28 to 6.61) times more likely to develop pre-eclampsia than multiparous women and women with a family history are 2.90 times (95% CI 1.70 to 4.93) more likely to develop pre-eclampsia than women without (rounded estimates of 3 used for both). 7 Appendix 1 (online-only) gives details of how these estimates are used to calculate the absolute risk of pre-eclampsia prior to applying the screening markers. The odds of developing pre-eclampsia given a positive test result were calculated for pre-eclampsia prevalence estimates of 0.5, 1, 2, and 4%, and detection and false-positive rates were calculated according to risk cut-off for the same estimates of prevalence. Bootstrapping was used to estimate confidence intervals for detection rates and marginal increases in the detection rates of endoglin and/or PlGF added to the Quadruple test markers. This involved sampling individual cases and controls (with replacement) from the data to generate 1000 different datasets of equal size to the original data (i.e. 88 cases and 275 controls). Detection rates were calculated for each of the 1000 datasets yielding estimates of the variance associated with the observed detection rates from which confidence intervals could be estimated. All analyses were performed using STATA (version 10, StataCorp 2007).
To determine if our results for endoglin and PlGF were consistent with those in the literature we performed a meta-analysis of the median endoglin and PlGF MoM values in pregnancies affected with pre-eclampsia using a random effects model. 8 Data sources were identified using a search of Medline and EMBASE databases and a manual search of the citation lists of the relevant publications and reviews. Key words for the Medline search were pre-eclampsia and endoglin or pre-eclampsia and placental growth factor. All studies published until October 2010 were eligible provided (i) they reported results based on samples of blood collected during the early second trimester of pregnancy (14–20 weeks’ gestation) and (ii) the median MoM and standard deviation in pregnancies that were later affected with pre-eclampsia were reported (or other results from which these could be derived).
Results
Figure 1 shows the concentration of PlGF in affected pregnancies according to gestational age. The median for unaffected pregnancies increased by 19% a week. Sixty-five percent of affected pregnancies had values below the median for unaffected pregnancies and 45% were below 0.5 MoM. The median PlGF in affected pregnancies was 0.68 MoM, and after adjusting for maternal weight was 0.67 MoM (95% confidence interval, 0.59 to 0.76). There was no relationship between weight adjusted PlGF MoM values and gestational age in affected pregnancies (P = 0.116).
Placental growth factor (PlGF) according to gestational age in pre-eclampsia and unaffected pregnancies Squares are weekly medians in unaffected pregnancies, dots are values in affected pregnancies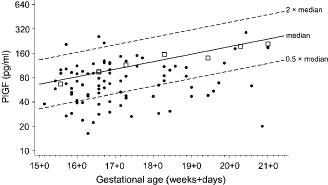
Figure 2 shows in a similar way the results on endoglin values. The median for unaffected pregnancies decreased by 4% a week. Seventy-five percent of affected pregnancies had values above the median for unaffected pregnancies and 25% were above 2.0 MoM. The median endoglin in affected pregnancies was 1.26 MoM, and after adjusting for maternal weight was 1.31 MoM (95% confidence interval 1.20–1.43, P < 0.001). There was no relationship between weight adjusted endoglin MoM values and gestational age in affected pregnancies (P = 0.509).
Endoglin according to gestational age in pre-eclampsia and unaffected pregnancies. Squares are weekly medians in unaffected pregnancies and dots are values in affected pregnancies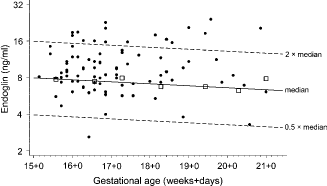
Figure 3 shows the median AFP, uE3, hCG (total and free β), inhibin-A, PlGF and endoglin in pregnancies that developed pre-eclampsia. All but AFP and free β-hCG were significantly raised or decreased.
Median AFP, uE3, hCG (total and free β), inhibin-A, PlGF and endoglin MoM values (and 95% confidence intervals) in pregnancies that developed pre-eclampsia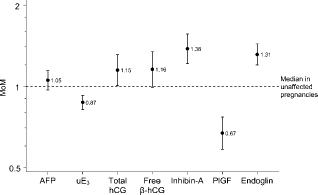
Probability plots of maternal weight-adjusted MoM values for the Quadruple test screening markers, PlGF and endoglin, together with the truncation limits used in this study for the estimation of screening performance are shown in Appendix 2 (online-only) Figure 1.
Table 1 shows the screening performance for the individual markers for early pre-eclampsia, late pre-eclampsia, and all pre-eclampsia, ordered from least to most discriminatory. The three best screening markers for all pre-eclampsia are endoglin, placental growth factor and inhibin-A, with DRs of 43%, 37% and 35% respectively, all for a 10% FPR. Endoglin performs better for early pre-eclampsia than for late pre-eclampsia (a 49% DR compared with a 37% DR respectively for a 10% FPR). The same pattern was evident for PlGF, inhibin-A and AFP but hCG (total or free β) and uE3 showed the opposite pattern.
Pre-eclampsia detection rates for individual markers according to false-positive rate
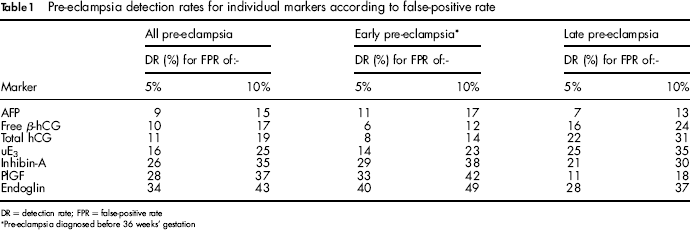
DR = detection rate; FPR = false-positive rate
Pre-eclampsia diagnosed before 36 weeks’ gestation
Table 2 shows the results for combinations of markers. Endoglin, on its own, performed better than PlGF, but its higher correlations with hCG and inhibin-A results in PlGF being the most discriminatory of the two when included with the Down's syndrome screening Quadruple test markers. With the addition of endoglin there was a nine percentage point increase in the detection rate; from 34% to 43% for a 5% false-positive rate. With the addition of PlGF, however, the detection rate increased to 45%. Including both markers increased the detection rate by five percentage points to 50%. There was no material difference in screening performance according to whether total or free β-hCG is used.
Pre-eclampsia detection rates (95% confidence interval) for the Quadruple test (AFP, uE3, hCG and inhibin-A) without and with the addition of endoglin and/or placental growth factor (PlGF)
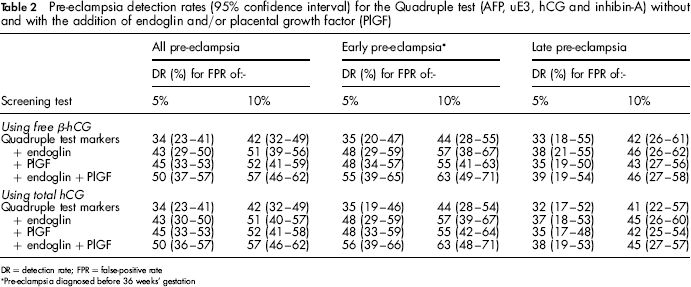
DR = detection rate; FPR = false-positive rate
Pre-eclampsia diagnosed before 36 weeks’ gestation
Table 3 shows the marginal increase in detection rates (with confidence intervals) using the Quadruple test markers and the addition of endoglin and/or PlGF compared with using the quadruple test markers alone. For all pre-eclampsia the addition of endoglin and/or PlGF resulted in a statistically significant increase in the detection rate, for example an increase of 9 percentage points (95% confidence interval 3 to 16) with the addition of endoglin and 11 percentage points (5 to 20) with the addition of PlGF (using total hCG; results were similar using free β-hCG). The increase in the detection rate was greater for early pre-eclampsia but there was no statistically significant increase in the detection rate for late pre-eclampsia with the addition of endoglin and/or PlGF.
Marginal increase in detection rate (95% CI) with the inclusion of endoglin and/or PlGF to the Quadruple test markers
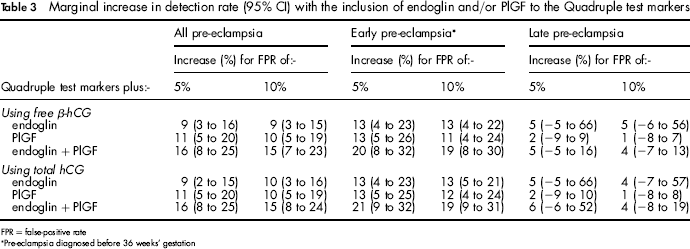
FPR = false-positive rate
Pre-eclampsia diagnosed before 36 weeks’ gestation
Table 4 shows the pre-eclampsia screening performance based on (i) women with a history of pre-eclampsia being classified as screen-positive regardless of their risk and (ii) using risk with a history of a previous pre-eclampsia pregnancy contributing to the risk estimate. All estimates also include parity and family history contributing to risk. Estimates of the detection rate for a 5% false-positive rate (DR5) are given for all pre-eclampsia, according to the prevalence of pre-eclampsia. Including a previous pre-eclampsia history in risk calculation yields almost identical screening performance to when women with a history are automatically classified as positive. With history contributing to risk only 3% or less of affected pregnancies with a history of pre-eclampsia would be missed but those will be balanced by a higher detection in women without a previous history.
Detection rate for a 5% false-positive rate (DR5) and odds of developing pre-eclampsia given a positive screening result with risk cut-off required according to marker combination, prevalence of pre-eclampsia and whether a history of previous pre-eclamspia is always screen-positive or history is used as a marker (total hCG used)
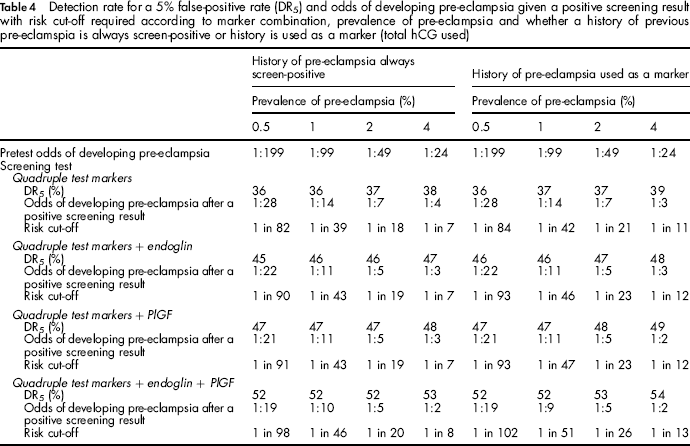
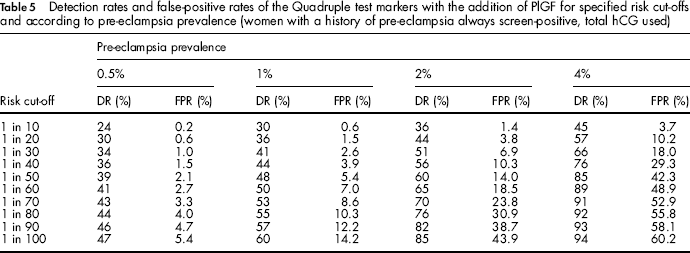
Table 5 shows, for the Quadruple test markers with the addition of PlGF the detection and false-positive rates according to the risk cut-off and the pre-eclampsia prevalence (women with a previous history of pre-eclampsia screen-positive and remaining women receiving serum screening). For a prevalence of 0.5%, a risk cut-off of 1 in 100 would achieve a detection rate of 47% and a false-positive rate of 5.4%. As the prevalence increases the risk cut-off to achieve similar screening performance increases so that if the prevalence were 4% a risk cut-off of 1 in 10 would achieve similar screening performance (45% detection rate and 3.7% false-positive rate).
Detection rates and false-positive rates of the Quadruple test markers with the addition of PlGF for specified risk cut-offs and according to pre-eclampsia prevalence (women with a history of pre-eclampsia always screen-positive, total hCG used)
Screening marker parameters (means, standard deviations, correlation coefficients and truncation limits) for all the markers are given in Appendix 2 Table 1.
Discussion
Our results show that the measurement of PlGF as an additional marker to the Quadruple test markers used to screen for Down's syndrome significantly improves the screening performance for pre-eclampsia. Despite similar screening performance univariately, the measurement of endoglin as an additional marker to the Quadruple test showed less of an improvement than the addition of PlGF (because endoglin is more highly correlated with the Quadruple test markers than PlGF). There is only a modest extra benefit in adding endoglin as well as PlGF to the Quadruple test.
The MoM values for PlGF and endoglin in our study are similar to the summary estimates from other studies. Figure 4 shows a meta-analysis (forest) plot for early second-trimester PlGF and pre-eclampsia based on the median levels in affected pregnancies from 11 previous studies together with the result from this study. The overall summary estimate of the median MoM in pregnancies affected with pre-eclampsia was 0.70 MoM; similar to our estimate of 0.67 MoM.
Placental growth factor (PlGF) median MoM in pregnancies that developed pre-eclampsia (labelled ‘cases’) from different studies and overall summary estimate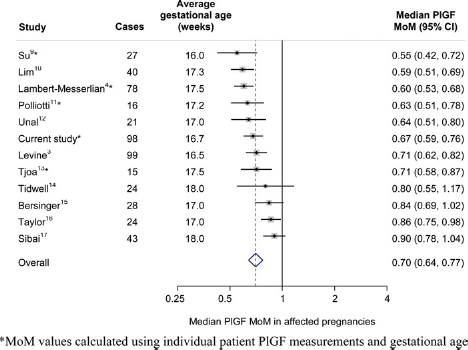
Figure 5 shows a similar meta-analysis plot of the median second-trimester endoglin levels in affected pregnancies from five previous studies together with the result from this study. The overall summary median MoM was 1.34, but this was heavily influenced by the results from one study.
21
If this outlying result is excluded the overall median MoM was 1.21, similar to our estimate of 1.31.
Endoglin median MoM in pregnancies that developed pre-eclampsia (labelled ‘cases’) from different studies and overall summary estimate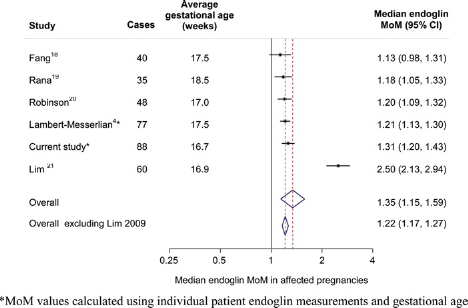
In screening it is worthwhile including an enquiry about a previous pregnancy with pre-eclampsia. If the prevalence of pre-eclampsia is 2%, screening using the Quadruple test markers with PlGF and a history of a previous pregnancy with pre-eclampsia can detect an estimated 47% of pre-eclampsia pregnancies with a 5% false-positive rate (45% without using history) yielding an odds of being affected given a positive result of 1:5, so 1/6 (17%) in this group will be expected to develop pre-eclampsia in their pregnancy. The most efficient policy is to include previous history of pre-eclampsia in the risk calculation whether or not women with a previous history are automatically classified as positive because this provides women with the most accurate risk estimate. However, classifying all women with a previous history of pre-eclampsia as positive (regardless of their risk) is sensible because these women will be particularly concerned with avoiding a recurrence of the disorder they had in a previous pregnancy, and there is little lost in screening efficacy.
Early pre-eclampsia is often severe and therefore of greater concern. In view of this our estimates of the screening performance of early pre-eclampsia are likely to be the most clinically relevant.
The value in screening for pre-eclampsia is threefold. First, to offer preventive treatment with aspirin (although more randomized trial evidence is needed to estimate the magnitude of the preventive effect 22 ); second, to provide more intensive antenatal monitoring for the early signs of pre-eclampsia with a view to early delivery if these become evident; and third, to conduct randomized trials of possible new preventive treatments such as L-arginine supplementation. 23
In summary, prenatal screening programmes for Down's syndrome could usefully add PlGF to the Quadruple test markers and include information on whether a previous pregnancy was affected by pre-eclampsia so that Down's syndrome screening and pre-eclampsia screening could be performed at the same time and on the same sample of blood.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.