
Abstract
Objective
To evaluate the effectiveness of two screening methods (imitanciometry screening and questionnaire) to identify children at risk for conductive hearing loss, comparing this data with complete audiologic evaluation.
Methods
Of 507 children aged between three and six, 111 completed all procedures. The observational methods used were: imitanciometry screening, a questionnaire to identify risk factors for hearing loss and complete audiologic evaluation. Results obtained in the first two instruments were compared with results from complete audiologic evaluation (gold standard). From these comparisons, sensitivity and specificity, accuracy, positive and negative predictive values, and odds ratio were determined for the two screening methods and for the combination of both methods.
Results
The two methods applied in series (questionnaire and after imitanciometry screening) showed a greater odds ratio and better correlation between sensitivity and proportion of false-positives (ROC curve).
Conclusion
Combining the two tests in series improved screening accuracy. This combination was the best tool for identifying children at risk for conductive hearing loss.
INTRODUCTION
Epidemiological data on the prevalence of hearing loss in developing countries is scarce, but there are estimates that hearing loss affects almost twice as many people in developing countries compared with developed countries. 1 The prevalence of mild- or greater-degree permanent hearing loss is estimated at one in every 10 people. 2 Although now legally required in Brazil, newborn hearing screening has as yet been implemented in only a few localities. Many children with congenital hearing loss are still being diagnosed late (age range 2–7 years old). 3
Otitis media (OM) is one of the most common disorders in childhood and about 80% of school-age children suffer at least a temporary hearing loss during any year. 4 Chronic OM is considered to be the main cause of mild to moderate hearing loss 1,5,6 with a prevalence from 1 to 46%. Prevalence is higher in developing countries, and it is considered by the World Health Organization to be a public health problem. 1,7
Assessments to identify hearing loss in children are important, as this group presents with a high rate of mild conductive hearing loss, which often does not attract the attention of family members, but can lead to serious consequences in children's development, as well as impairments of learning, language and sensory functions of higher centres. 8 In Brazil, hearing health actions in primary care are insufficient to provide adequate treatment, or even to identify this demand. There are few health professionals in this area 2 and the cost of equipment and human resources hinders the implementation of such programmes. The developing Family Health Strategy still lacks speech-language and audiology actions directed to primary care in audiology. Lower-cost procedures, which are accessible to poorer areas where there are currently limited resources, need to be introduced. 9
This study aimed to evaluate the effectiveness of two screening methods (imitanciometry screening and questionnaire) to identify children at risk for conductive hearing loss, by comparing this data with complete audiologic evaluation.
METHODS
The study involved 507 children aged 3–6 years, from two public preschools in the area served by the University Health Center Samuel B. Pessoa. While all the children from these preschools were invited to participate, the study sample comprises only the children whose parents signed the study consent form. From 507 children who had imitanciometry screening, 111 underwent a complete audiologic evaluation and questionnaire.
During 2009 and the first half of 2010, imitanciometry screenings were conducted in schools during school hours. The screening consisted of visual inspection of the external ear canal to identify possible restrictions to the testing and imitanciometry screening, using the equipment Otoflex 100 (Madsen). The imitanciometry test protocol was composed of tympanometry and ipsilateral acoustic reflexes scan from 500 to 4000 Hz at 100 dB. The screening results were classified ‘pass’ or ‘refer’. The latter was applied for any change in tympanometry (curves B, C, Ad and As) whether or not accompanied by the absence of acoustic reflex at one or more frequencies.
All 177 children who failed were referred for complete audiologic evaluation in the University Health Center. A further 50 children classified ‘pass’ were randomly selected to undergo complete audiologic evaluation, to allow comparison of the questionnaire applied in children who passed and failed in imitanciometry screening. However, of the 177 children who failed imitanciometry screening, 84 did not attend the scheduled evaluation, and only 18 of those who passed imitanciometry screening completed the assessment. Thus, 111 children underwent a questionnaire and complete audiologic evaluation (Figure 1).
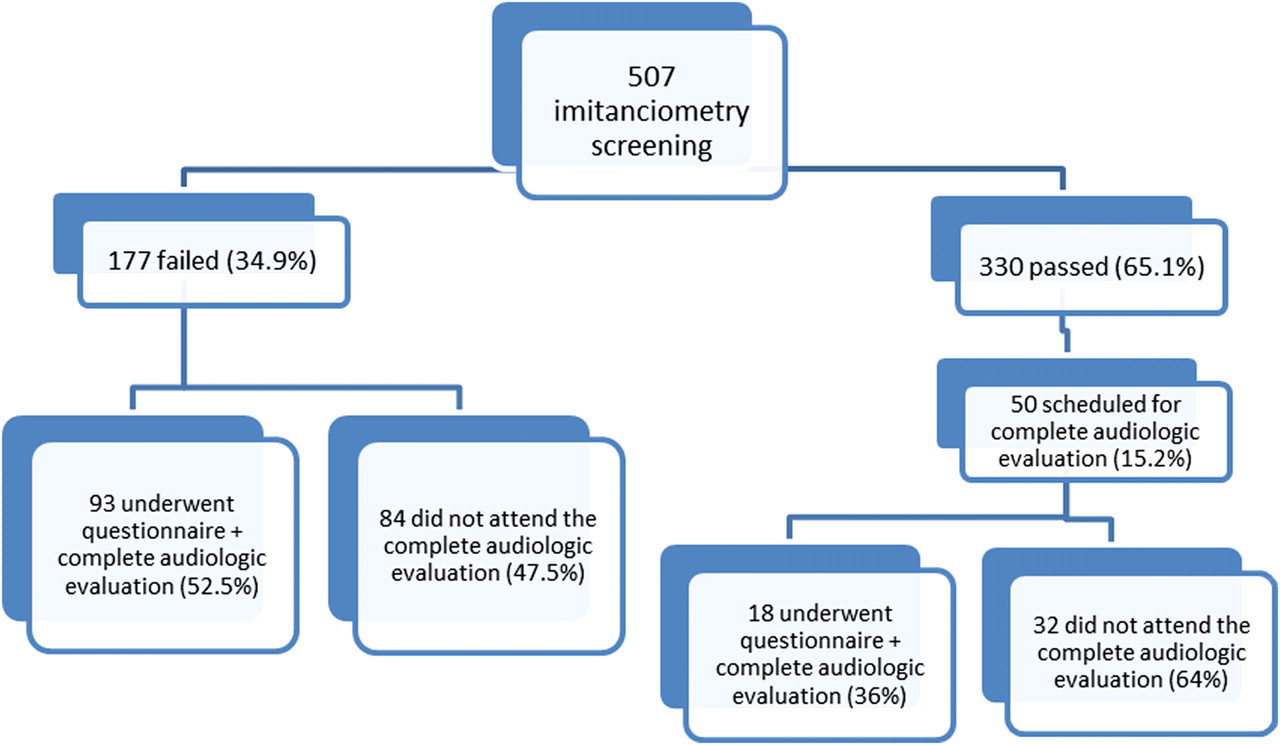
Flowchart of research participants' follow-up
The following procedures were performed after imitanciometry screening:
i) A 14-question survey, ‘Low cost instrument for identifying children at risk for hearing loss’, was developed, covering aspects of medical and otological history, global development, communication skills and hearing complaints. The questions were developed based on previous studies
3,10–14
and the questionnaire was validated in another investigation.
15
Each positive answer, indicating risk for hearing impairments, was scored with 1 point. In accordance with the ROC analysis (see Results), the classification rule was established as: total score from 0 to 3, or 0 to 4, or 0 to 5 – normal hearing (‘pass’) and total score greater than 3, or 4, or 5 – hearing loss (‘refer’). ii) Pure tone audiometry testing was performed in an acoustic booth (audiometer Itera II – Madsen). Auditory air-conducted thresholds at frequencies from 250 to 8000 Hz were obtained. When these thresholds exceeded 15 dB HL, bone-conducted thresholds (500 to 4000 Hz) were also determined. This test is the gold standard and its result was compared with the procedures: imitanciometry screening and questionnaire. iii) Imitanciometry was conducted (tympanometry and ipsilateral and contralateral acoustic reflexes at the frequencies 0.5 to 4 kHz) with the equipment AT 235 (Interacoustics). Before starting this procedure, a visual inspection of the ear canal was conducted to rule out any factors that might hinder the examination.
A normal audiologic evaluation was considered to be normal hearing thresholds, i.e. up to 15 dB HL, type A tympanometric curve and present acoustic reflexes in both ears. Abnormal results consisted of hearing thresholds greater than 15 dB HL, tympanogram type B, C, Ad or As and absence of acoustic reflexes in one or both ears.
The imitanciometry screening, complete audiologic evaluation and questionnaire were applied by different people, who did not know the results of the other procedures; nor did the patient or his/her family know the outcome of the imitanciometry screening (double blind), thus avoiding a possible source of bias in the study.
Sensitivity, specificity, positive and negative predictive values (PPV and NPV, respectively) and the ROC curve for each procedure, comparing the two methods (imitanciometry screening and questionnaire) with each other and combined with the audiologic evaluation were determined and analysed.
For each instrument (imitanciometry screening and questionnaire), sensitivity was defined as the percentage of patients with ‘fail’ results in the instrument among those who presented abnormalities in the audiologic evaluation. Specificity was defined as the percentage of patients with ‘pass’ results in the instrument who had normal audiologic evaluation. PPV was defined as the probability of an abnormal hearing evaluation among the patients with a ‘fail’ result in the instrument, while the NPV was the probability of a normal hearing evaluation among those with a ‘pass’ result in the instrument. Accuracy was measured by the sum of true-positive and true-negative cases over the total number of cases. In the serial and parallel analysis, the above criteria were employed, but using the combination of the two instruments. Using imitanciometry screening both first and after the questionnaire and complete audiologic evaluation, we could verify what would happen if the questionnaire was applied first, highlighting that the professional who applied the questionnaire was not the same person who carried out the imitanciometry screening. The serial analysis considered the result of the questionnaire and for those who failed (score greater than 3, or 4, or 5 – in questionnaire) also the result of imitanciometry screening; in this situation, the child was considered to have hearing loss only if they failed in two instruments (increased specificity). For the analysis in parallel, it was considered that the questionnaire and imitanciometry screening were performed simultaneously; in this instance, the child was considered not to have hearing loss only if they passed in both tests (increased sensitivity).
The statistical analyses were performed using SPSS 15.0, Medcalc and Minitab. The Kolmogorov-Smirnov test was applied to determine normality of variables distribution. The chi-square test with a significance level of 5% was used.
RESULTS
Table 1 shows that there was only a statistically significantly larger number of male subjects among those who underwent full audiologic evaluation. There was also a higher prevalence of children in the five-years-old age group in all evaluated children.
Characteristics of children who underwent imitanciometry screening (n = 507) – on the left, and children who underwent complete audiologic evaluation (n = 111) – on the right
Of the 330 children who passed imitanciometry screening, 49% were female and 51% male, with no statistically significant difference (P = 0.64). Among children who failed, 45.2% were female and 54.8% male, also with no statistically significant difference (P = 0.07).
Of the 111 subjects who underwent a complete audiologic evaluation, results were normal for 68 (61.3%) and abnormal for 43 (38.7%), i.e. normal results were significantly more common (P < 0.001). All abnormal results corresponded to mild to moderate conductive hearing loss.
Figure 2 and Table 2 compare the results obtained in each instrument (or combination of instruments) with the result of the complete audiologic evaluation. When tests in series were used, specificity, accuracy and odds ratio were better. The area under the ROC curves for each instrument was better for the tests in series (Figure 1).
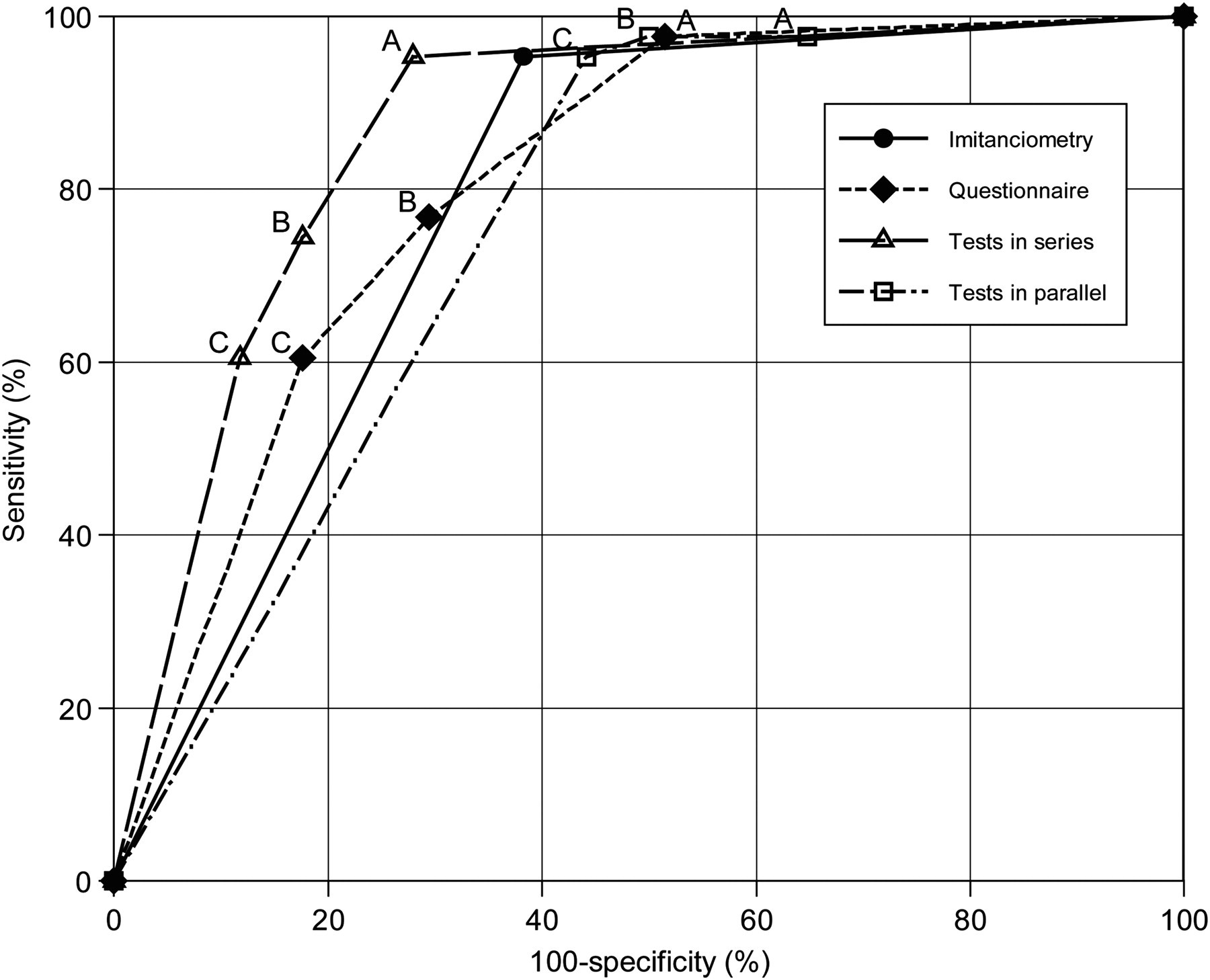
Single ROC plot to the imitanciometry screening, questionnaires and tests in series and in parallel based on the use of 0 to 3 points to determine ‘pass’ (condition A) when compared with other conditions B - 0 to 4 points and condition C - 0 to 5 points. Area under curve (AUC) for imitanciometry was 0.79. AUC for questionnaire was 0.81. AUC for tests in serial was 0.87. AUC for tests in parallel was 0.76
Sensitivity, specificity, positive predictive value, negative predictive value, accuracy and odds ratio of each instrument and their combination (tests in series or parallel) for all conditions
DISCUSSION
In the complete audiologic evaluation, results for 61.3% of subjects were normal and 38.7% were abnormal. All abnormalities corresponded to mild to moderate conductive hearing loss, a prevalence expected for developing countries. 1
A study conducted in Nigeria, 3 which also compared the efficacy of imitanciometry screening and questionnaire with audiometry findings in school children (mean age 6.7 years) found a conductive and mixed hearing loss prevalence of 10.6% and a sensorineural hearing loss prevalence of 3.3%. However, hearing loss was defined as hearing thresholds greater than 25 dB, compared with the thresholds above 15 dB in our study. This may explain the higher prevalence of conductive hearing loss in our study, which detected children with smaller hearing loss. The age ranges in the two studies also differ, 3 and it is recognized that the prevalence of otitis media is higher among two- and five-year-olds. 16,17 Also, above this age group, the prevalence of otitis decreases, which may explain the lower prevalence found in the Nigerian study. 3
A Polish study has also found a high prevalence of mild conductive hearing loss in school children aged six to 10 years, reinforcing the importance of using this type of evaluation in school-age children. 8 Similarly, a study of Brazilian school children aged from seven to 14 years using thresholds above 15 dB found 24% of ears had hearing loss, of which 7% was sensorineural and 17% conductive. 18 Another study 10 has found that 3.5% of the ears of 317 Chinese students aged from five to 12 years presented tympanometry results indicating alteration in the middle ear, and 6.9% had abnormal results in sweep audiometry, the majority of them corresponding to sensorineural hearing loss. This lower prevalence of conductive hearing loss in the two studies, when compared with the present one, can also be explained by differences in the age group studied.
Differences observed across studies of the prevalence of hearing loss in school children in developing countries have been noted by Olusanya 3 to range from 3.9 to 24.5% (with or without middle ear alteration), while middle ear disorders ranged from 7.3 to 36.2%, regardless of differences in the protocols employed.
The questionnaire and tests in parallel were the methods with higher sensitivity, but when tests in series were used, specificity, accuracy and odds ratio were better, although the accuracy should be considered with caution, because the prevalence of disease affects the validity of a test, i.e. less prevalent disease applies greater weight to specificity in calculation of overall accuracy. Conversely, more prevalent disease applies greater weight to sensitivity. 19 In this case, better accuracy was obtained using tests in series, and the odds ratio confirmed that tests in series, when the cut-off used in the questionnaire was over 3 points, were the best method to identify children with conductive hearing loss.
Despite the high sensitivity, the lower specificity of imitanciometry screening (an objective method) may be related to those children who failed the screening and had colds at the time of the test, thus presenting possible transient changes in the middle ear, or Eustachian tube dysfunction. These abnormalities may have had spontaneous resolution during the period between the screening and the complete audiologic evaluation 3 , which was an average of two to three weeks.
The questionnaire showed 97.67% sensitivity, 48.53% specificity, and accuracy of 67.56%. Other studies have found different values when comparing questionnaires with auditory thresholds obtained by audiometry, although the criteria for the classification of hearing losses and methods for obtaining the thresholds differ in each study. Hammond et al. 12 found 56% sensitivity and a specificity of 52%; Newton et al. 14 found 100% sensitivity and 75% specificity, although these authors only compared the results for children with thresholds above 40 dB HL, which facilitated the parents' perception of the hearing loss and therefore improved the sensitivity of the method. Olusanya 3 reported a sensitivity of 10% and specificity of 94% on questionnaire; Bu et al. 10 evaluated the sensitivity and specificity of each question in the questionnaire individually, and obtained values of 7 to 42% for sensitivity and 76–99% for specificity. The verified accuracy did not exceed 54%, which is below that observed in our study.
The diversity of results can be explained by differences between the questionnaires, screening methods and/or audiologic evaluation, classification criteria for pass/fail and hearing loss, and different ethnicities and age groups in the populations studied. The use of questionnaires to identify children at risk for hearing loss has limitations because it depends on the skills and motivation of the observer. 14 As reported in several studies, 3,10,14,20,21 hearing loss is difficult for parents to perceive, which could cause confusion in answering questionnaires, and even when hearing loss has occurred, speech and language development may follow typical patterns, which makes perception difficult. This may explain the lower specificity in our study, as most hearing losses observed in children participating in this study were mild and/or unilateral.
This lower specificity indicates that many children who do not have hearing problems failed, that is, obtained over 3 points in the questionnaire. This may be explained by two of the questions regarding previous hearing tests (newborn hearing screening or previous audiometry). The children who participated in this research had not benefited from the new law regulating newborn hearing screening, and in Brazil paediatricians and schools do not ask for hearing assessment as a common practice. 22 Thus, most children received two points in the questionnaire if they had not completed any previous hearing tests. Other questions regarding otological history or speech were often scored even when the child did not necessarily have any hearing problem. 10,12,14
To investigate improving the effectiveness of these instruments, the possibility of combined screening tests (in series or in parallel) was assessed. 3 The results demonstrate that the tests in series showed better specificity, accuracy and odds ratio when compared with screening (imitanciometry and questionnaire) separately or with tests in parallel. Sensitivity was similar to that obtained in other methods. These findings were similar to those obtained by Olusanya, 3 who found for the combined questionnaire and otoscopy a 60% sensitivity and 58% specificity, and for the combination of these two procedures with tympanometry, 76% sensitivity and 54.6% specificity, although our results are better, indicating that the proposed instruments in this study are more effective for this purpose.
A study of this issue 8 proposes the implementation of combined hearing screening using two instruments (sweep audiometry and speech test in noise using software) simultaneously, to increase the sensitivity of the evaluation. The present study showed a similar sensitivity using only the questionnaire or the combination of the two screening instruments (questionnaire and imitanciometry screening), but there was also improvement in the specificity due to the use of instruments in series (i.e. only those who failed the questionnaire also underwent the imitanciometry screening).
In this form of screening (in series) a questionnaire is administered by teachers, and only children who fail on the questionnaire are referred for imitanciometry, which requires special equipment and a trained professional. This would reduce the costs of screening as only children who have failed undergo this second procedure.
Calculation of the cost of the screening programme must take into account not only the direct cost of the screening procedures themselves but also the cost of the assessment that would be undertaken as a consequence of the screening. For this reason a better specificity is desirable, in order to reduce the costs associated with a false-positive test result (costs of parents' lost time from work, transportation, unnecessary tests and procedures, etc.). 23
The use of associated instruments (in series) improves the screening odds ratio, reducing both the number of false-positives and false-negatives. 9 To reduce the costs of hearing screening it would be sensible to administer the questionnaire (a low-cost instrument) initially, facilitating large-scale application in areas of the country with fewer financial and human resources. Then, for children who fail, the imitanciometry screening should be applied, as it is a more viable instrument to be employed in schools compared with audiometry, because of the noise in these institutions.
The number of children who did not attend the complete audiological assessment (47.46% of those who failed and 64% of those who passed in the imitanciometry screening) may have influenced our results. Adherence to this type of study is not always high, as found by Bu et al., 10 who obtained a 61% return of the questionnaires sent to parents, and by Manfredi & Santos, 24 who studied newborns at risk for hearing loss and had high rates of absence from the auditory monitoring programme (from 43.3% to 51.3%). These latter figures are similar to our own. The explanations given by absent parents in the Manfredi & Santos 24 study vary from forgetting the follow-up appointment to being short of money to pay for transportation.
The importance of the dropout rate in some of the work to which we refer 10,24 is also applicable to our situation. It is not possible to ensure adherence to follow-up. Failure to attend is due to a number of reasons, including a lack of understanding of the importance of follow-up (regardless of whether this is related to a study), and financial impediments, especially in developing countries like Brazil. An effective, low-cost tool is required, to provide data and to facilitate the referral of children who really need a complete audiological evaluation and a medical assessment.
Further studies should be conducted to improve the effectiveness of the questionnaire investigated here, to employ alternative forms of school-age screening, and to evaluate other low-cost tool combinations which may be more effective in identifying children with hearing problems. No children with sensorineural hearing loss were included in this study, and so our results are only relevant and effective in screening for conductive hearing loss.
The development and validation of questionnaires based on parents' observations, which can be important low-cost tools for identification of children at risk for hearing loss in developing countries, are of great value because they may be used routinely in the school system in the future. They may also be incorporated into the Family Health Strategy, maximizing the coverage of hearing health services and diminishing the time between the parents' perception of a possible hearing impairment and referral for diagnosis and, if necessary, assistance. If this practice could be established, children who have any kind of hearing problem could benefit from early treatment. Guidance might also then be provided by health professionals to parents and teachers regarding hearing level in classrooms (minimum signal to noise ratio to assure learning). The importance of such guidance to this age group was evident from the levels of conductive hearing loss observed in this study, which, if untreated, could affect the auditory, linguistic and scholastic development of the children significantly. 6,8
CONCLUSION
Individually, imitanciometry screening and the questionnaire showed good sensitivity, but low specificity, in identifying children at risk for hearing loss. The combination of these two tests in series showed a sensitivity of 95.35% and specificity of 72.02%, and is the best screening tool for identifying children at risk for conductive hearing losses.
Footnotes
ACKNOWLEDGEMENTS
This study was funded by FAPESP (The State of São Paulo Research Foundation) Protocol 2008/08496-7.
Appendix
Questionnaire to identify risk for hearing loss (2–10-year-old children)
1. Identification
2. Birth locality (maternity/city)
3. Did child have some hearing screening on birth?
– Yes
– No (1 point)
4. Did child ever have a hearing test?
– Yes
– No (1 point)
5. Was there presence of any risk indicators for hearing loss (according to Joint Committee on Infant Hearing, 2000) – all risks are enumerated.
– Yes (1 point)
– No
6. In what position is the child breastfed? (to describe)
– Lying down (1 point)
– Sitting?
7. Family history: is there any deaf person in your family? Who?
– Yes (1 point)
– No
8. Did child have any health problems? (Some diseases are enumerated: meningitis, brain injury, frequent otitis media or ear infection).
– Yes (1 point)
– No
9. Does child pay attention to loud noises?
– Yes
– No (1 point)
10. Does child pay attention when he/she is called by their name?
– Yes
– No (1 point)
11. Does he/she need gesture or high-intensity voice to understand?
– Yes (1 point)
– No
12. Does your child hear as well as other children of the same age?
– Yes
– No (1 point)
13. Does your child speak as well as other children of the same age?
– Yes
– No (1 point)
14. Does your child understand orders, even if not looking at the speaker? For example: bring the spoon to the mother (without pointing to the object)?
– Yes
– No (1 point)
15. Does your child like music?
– Yes
– No (1 point)
16. Did anybody comment that your son/daughter does not hear well or that his/her speech is very bad?
– Yes (1 point)
– No