
Abstract
Objectives
To evaluate a two-tier reflex guaiac-based faecal occult blood test (gFOBT)/faecal immunochemical test (FIT) algorithm in screening for colorectal cancer.
Setting
Fourth screening round in NHS Tayside (Scotland).
Methods
gFOBT were sent to 50–74-year-olds. Participants with five or six windows positive were offered colonoscopy. Participants with one to four windows positive were sent a FIT and, if positive, were offered colonoscopy. Participants providing an untestable gFOBT were sent a FIT and, if positive, were offered colonoscopy. Outcomes following positive results, cancer stages and key performance indicators were assessed.
Results
Of 131,885 invited, 73,315 (55.6%) responded. There were 66,957 (91.3%) negative, 241 (0.3%) strong positive, 5230 (7.1%) weak positive and 887 (1.2%) untestable results. The 241 participants who had five or six windows positive had more cancers than those positive by other routes: only 3 of the 30 cancers (9.7%) were Dukes' A. Among the 983 positive results from the weak positive gFOBT then positive FIT route, there were fewer cancers and more normal colonoscopies, but more adenomas than in the group with a strong positive gFOBT. In those with an untestable gFOBT, 77 had a positive FIT result, with fewer true and more false positive results than in the other groups. Fewer males had cancer and stages were earlier than in females, but more had adenoma. The detection rate for cancer was 0.18% and the PPV for cancer and all adenomas was 41.3%.
Conclusions
The algorithm and FIT following a weak positive gFOBT have advantages. FIT following an untestable gFOBT warrants review.
INTRODUCTION
Randomized controlled trials have shown that colorectal (bowel) cancer screening using guaiac-based faecal occult blood tests (gFOBT) reduces disease-specific mortality. 1 Three demonstration pilot screening rounds, inviting all 50–69-year-olds, and using gFOBT alone, were carried out in 2000–2, 2002–4 and 2005–7 in three NHS Boards in Scotland, namely Fife, Grampian and Tayside. 2 The experience gained from the demonstration rounds informed the development of the Scottish Bowel Screening Programme (SBoSP). Roll-out of the SBoSP began in June 2007 and is now complete. 3
Most gFOBT involve collection of two samples from each of three faecal specimens onto a single card. The randomized controlled trials that used such gFOBT employed various approaches, with differences in dietary restriction, rehydration of test kits prior to development and number of windows considered positive. This makes comparison of findings difficult, which makes setting of the detailed approach to be used in any new screening programme problematic. Moreover, gFOBT have many disadvantages for screening programmes, 4 including lack of analytical specificity for blood.
During the pilot screening rounds, evidence showed that faecal immunochemical tests (FIT), sometimes called immunochemical faecal occult blood tests (iFOBT), had significant advantages over gFOBT. 4, 5 However, available qualitative FIT, those that simply give positive or negative results, were considerably more costly than gFOBT and their lower analytical detection limits meant that the positivity rate would be much higher than the planned 2% that could be sustained by the available colonoscopy resource in Scotland. Their use as a first-line test was therefore precluded. A suggested strategy to achieve better analytical specificity and to reduce the false-positive test rate when using gFOBT alone is the use of gFOBT as a first-line test, followed by FIT for individuals with positive gFOBT on the same sample of faeces. 6 We investigated an adaptation of this strategy 7, 8 and the theoretical benefits were attained, at least in the research setting. We described the approach as the two-tier reflex gFOBT/FIT screening algorithm 7 and, because of our positive experiences, this strategy was adopted for the SBoSP, in which all individuals aged 50–74 years are invited to participate every two years.
We here describe the outcomes of an observational study using this strategy over a two-year screening round in NHS Tayside, mainly incident, and likely to be in, or approaching, steady state because it is the fourth screening round. We aimed to provide in-depth insight into the translation of our research findings into service delivery and document, for the first time, the detailed outcomes to aid others considering adopting this particular screening algorithm.
METHODS
All invited subjects were sent the gFOBT used in the three Scottish pilot screening rounds and currently used in the three other countries of the UK, which required two samples from each of three faeces collected by cardboard applicator and applied to the six windows of the test card (hema-screen, Immunostics Inc, Ocean, NJ, USA), The kit was accompanied by a ‘Know the Facts’ leaflet and information on how to perform the test; these are available on the Internet. 3 If no windows were positive, the participant was sent a letter noting that the screening test was not perfect and highlighting the need to consult a general practitioner if any relevant symptoms arose. If five or six windows were positive (a strong positive result), the participant was sent a letter, as was their general practitioner, and referred for colonoscopy. If one to four windows were positive (a weak positive), the participant was sent a FIT kit that required samples from each of two faeces collected by cardboard applicator and applied to the two windows of the card collection device. After completion of collection and return to the Laboratory, the faeces smeared to fill the windows on the tab of the card (hema-screen DEVEL-A-TAB, Immunostics Inc, Ocean, NJ, USA) were delivered into a specimen preparation tube containing phosphate buffered saline (hema-screen SPECIFIC). After mixing on a horizontal rotary mixer for 30 min, a portion of the faeces in buffer was dropped into the specimen well of an immunochromatographic test cassette. At five minutes, positive results are detected for haemoglobin (Hb) at a concentration of 50 ng Hb/mL buffer. This is equivalent to 50 µg Hb/g faeces. Further details of this FIT methodology have been described elsewhere. 8 If the test result was positive, the participant was informed by letter and referred for colonoscopy and, if negative, the participant was sent the appropriate letter as described above. Some participants provided an untestable gFOBT due to the kit being expired, incomplete, spoiled by the participant or unused, or having a technical problem or an irresolvable participant identity difficulty. To expedite the screening pathway, these individuals were sent a FIT rather than a repeat gFOBT.
All analyses were carried out in the Scottish Bowel Screening Centre Laboratory by trained staff whose major function is to perform faecal test analyses. The Laboratory is consultant-led, has a comprehensive total quality management system and is accredited to ISO 15189 based standards by Clinical Pathology Accreditation (UK) Ltd.
All results from 1 July 2007 to 30 June 2009 inclusive were examined: this represents the entire fourth round of screening in NHS Tayside. Positive results arose because the participants' test results were (1) strong positive initial gFOBT, (2) weak positive gFOBT then followed by a FIT positive test result or (3) a kit being submitted then followed by a FIT positive test result. For all positive results, data for colonoscopy outcomes and pathology were downloaded from the appropriate NHS Tayside clinical IT systems. Data on colonoscopy were collected on the quality of the investigation, including quality of preparation and completeness of colonoscopy, and on the results including number, size and localization of colorectal cancers and adenomas, and whether biopsy was performed. Full pathological data were collected on all excised and biopsied specimens including polyp type, presence or absence of malignancy and, in all adenomas, the severity of dysplasia. Adenomas were classified as recommended by the British Society of Gastroenterology. 9
This evaluation was approved by the Scottish Bowel Screening Programme Board and the Caldicott Guardian of NHS Tayside.
RESULTS
Over this screening round, 131,885 people were invited and 73,315 responded, a 55.6% tested population rate (53.2% for men and 60.3% for women). Of the initial responses, 66,957 (91.3%) results were negative. There were 241 (0.3%) strong positive results, of which 143 (59.3%) were men, 5230 (7.1%) weak positive results of which 2999 (57.3%) were men, and 887 (1.2%) untestable tests of which 471 (53.1%) were men.
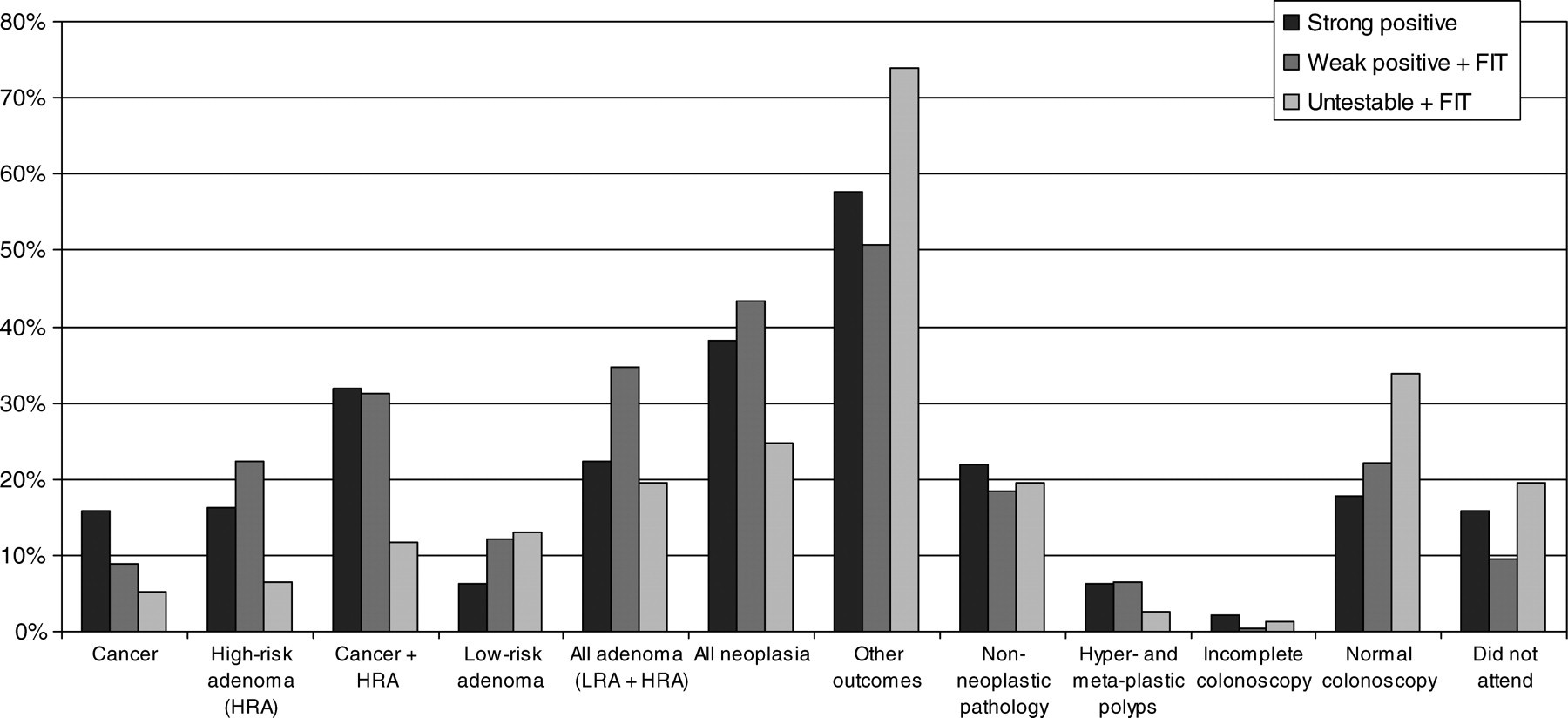
The clinical outcomes of colonoscopy and pathology in the 1301 participants with positive test results and in the groups with the three different routes to positivity, namely, strong positive gFOBT (241, 18.9%), weak positive gFOBT then followed by positive FIT (983, 75.6%) and untestable then followed by positive FIT (77, 5.9%), are shown in Table 1. The overall final positivity rate was 1.77%. The overall data for the three routes to positivity are shown in Figure 1. In all three groups, 785 (60.3%) positive results were found in men. Of the strong positive gFOBT, weak positive gFOBT plus positive FIT and untestable followed by positive FIT routes, 143 (59.3%), 600 (61.0%) and 42 (54.5%), respectively, were men.
Outcomes for 1301 participants with positive test results for the three routes to positivity
Outcomes for participants with positive results and percentages of totals for the three routes to positivity
aAll neoplasia comprises cancer + HRA + LRA
bOther outcomes comprises non-neoplastic pathology + incomplete colonoscopy + normal colonoscopy + did not attend
cNon-neoplastic pathology includes hyper- and meta-plastic polyps and other bowel diseases including diverticular disease, haemorrhoids and inflammatory bowel disease
Of those 106 cancers for which staging was available, the Dukes' stages are shown in Table 2. In men, 18 (30.5%), 20 (33.9%), 20 (33.9%) and 1 (1.7%) were Dukes' A, B, C1 and C2, respectively; in women, 13 (27.6%), 8 (17.0%), 23 (48.9%) and 3 (6.4%) were found for these stages.
Overall stages of detected cancers and percentages of totals for the three routes to positivity
The overall uptake, positivity rate, cancer detection rate, positive predictive value (PPV) for cancer and PPV for cancer and all adenoma are shown in Table 3 along with the data from the three pilot screening rounds carried out in Scotland 2 in 2000–2, 2002–4 and 2005–7 and in two pilot screening rounds in 2000–2 and 2002–4 and in the first screening round of the NHS Bowel Cancer Screening Programme in England. 10
Key Performance Indicators in this study and from three screening rounds in Scotland and England
DISCUSSION
As is the case in pilots and programmes throughout the UK 2,10 and elsewhere, 11 many of the findings in this fourth screening round, which is mainly incident but has a small number in prevalent screening, are as expected when compared with the large amount of data available on the many screening programmes using faecal tests. 12 Fewer men participated and, overall and for all three routes to positivity, there were more men with positive test results than women (see Table 1).
A small number of participants (241, 0.3% of those who returned a gFOBT) had five or six windows positive on gFOBT. This group, who have some evidence of blood present in every faecal sample collected, had more cancers than those positive by the other two routes. Although non-neoplastic pathology including diverticular disease, haemorrhoids and inflammatory bowel disease are more common in this group than those positive by the other two routes, these individuals do have more advanced cancers with only three of the 30 cancers (9.7%) being Dukes' A. Fewer had a normal colonoscopy than in the other two groups. A recent study has confirmed that number of positive windows is related to severity of neoplasia. 13 These findings support the current screening algorithm where individuals with strong positive gFOBT results are referred directly for colonoscopy without further testing. Disappointingly, 38 (15.8%) did not attend for colonoscopy, although a small number considered unfit for such invasive investigation might have been included here. These could not be identified as such from the NHS Tayside IT systems.
The majority of positive test results found arose from the weak positive gFOBT then followed by positive FIT route; 5230 (7.1%) participants who returned a test kit had an initial weak positive gFOBT result and it would be impossible to directly refer all of these 5230 individuals, albeit with some evidence of blood in their faeces, for colonoscopy directly. Our thesis was that undertaking a FIT rather than a second gFOBT would improve outcomes because fewer false-positive results would occur due to the better analytical specificity of FIT. 7,8 Of those with a weak positive gFOBT, only 18.8% had a subsequent positive FIT leading to an overall positivity rate (1.77%) that could be sustained by the available resources in NHS Tayside. Although this group had fewer cancers and more normal colonoscopies than the group with a strong positive gFOBT, the number of adenomas, both high- and low-risk, was higher. It has been documented previously that FIT is better at detecting adenomas than gFOBT. 14 As shown in Table 2, a high proportion of the cancers (37.5%) were Dukes' A. Ninety-four (9.7%) did not attend for colonoscopy. It may be that receipt of two faecal tests of different types raises the levels of concern in participants and encourages attendance when a final positive test result is communicated.
The group who submitted an untestable gFOBT kit were sent a FIT kit so these participants were actually undertaking a qualitative FIT as a first-line test. In view of the low analytical detection limit of 50 µg Hb/g faeces for the FIT used, compared with the 600 µg Hb/g faeces of the gFOBT used, a high positivity rate was expected. Of the 887 individuals in this group, 77 gave a positive FIT result, a positivity rate of 8.7%, confirming our concept that use of such a qualitative FIT as a first-line test would be currently unsustainable in view of the limited colonoscopy resources available. Only 1.2% of respondents submitted an untestable kit, which led to only 5.9% of the positive test results being due to this route to positivity. In contrast to possible expectations of a qualitative FIT as a first-line test, those who were FIT positive after an untestable result did not have more true positive results, less than 25% having any evidence of neoplasia. Moreover, these individuals had higher proportions of false-positive results due to non-neoplastic bowel conditions (as above) and normal colonoscopy: 19.5% did not attend for colonoscopy. Thus, in spite of the theoretical advantages of FIT as a first-line test, the detection of significant neoplasia was low and the false-positive rate was high. In addition, FIT kits are more expensive than gFOBT and take significantly more time to process in the laboratory. Sending a repeat gFOBT to those who submit an untestable kit rather than a FIT may save considerable resources without loss of clinical performance.
Although men had more positivity than women, a smaller proportion had cancer. Cancer stages in men were earlier than in women, 35.6% of men having Dukes' C in contrast to the 55.3% in women. This raises some concern as it has been found that more women have interval cancers than men in Scotland. 15 Because this is the fourth screening round in NHS Tayside, and most who participate in screening do so regularly 16 , this implies that the current screening strategy misses significant neoplasia and it might be that evolution to an approach that uses an automated quantitative FIT would be of advantage in this regard. 11 Men did, however, have more adenomas of all types than did women.
The important question is whether the two-tier reflex gFOBT/FIT algorithm used in the SBoSP (and in Wales and Northern Ireland) delivers benefits. Documentation of a small number of the many Key Performance Indicators used in the SBoSP with those that are available in the literature for the first three screening rounds in Scotland 2 and in England 10 is shown in Table 3. Further comparison can be done with the detailed overall outcomes in Scotland and the 14 NHS Boards 17 , but this would be confounded by the fact that 11 of these are at different stages of screening due to the phased roll-out across the country. Comparison of outcomes across screening programmes is difficult, but recent results from an international survey 12 might prove of interest for comparison of programmes. It should be borne in mind that aspects of the six screening rounds documented in Table 3 and this study differ, and there are significant caveats to simple comparisons. The first three screening rounds in Scotland were the demonstration pilot rounds which invited individuals aged 50–69 years and involved all eligible residents in three NHS Boards, Grampian, Fife, and Tayside, although the population demographic characteristics are not very different throughout East and North-east Scotland. The data from England are restricted to three Primary Care Trusts and encompass individuals aged 60–69 years only. Our data reflect outcomes over the ages 50–74 years. Comparison across age-adjusted data would have some advantages but such data are not available for all screening rounds in Table 3. The first screening rounds in both Scotland and England were prevalent screening; other rounds in both countries are mainly incident but include individuals in prevalent screening. Further, there were changes in the detailed delivery of the rounds. The first two screening rounds in Scotland and the three rounds in England used very similar screening strategies as described in detail previously. 18 Dietary restrictions for repeat tests in those with weak positive results were ceased after the first rounds. In addition, the third screening round in Scotland was rather different and used an approach identical to the two-tier gFOBT/FIT strategy except that gFOBT was used throughout rather than FIT. This approach was adopted because it was similar to that which would be used in the SBoSP, the protocols for which were being tested in detail at that time, and required fewer test kits and simpler IT. In spite of these significant caveats, some final conclusions can be drawn.
Uptake is similar across rounds, possibly unsurprising as all use gFOBT as the initial test. The positivity rate is lower than that found for first and second rounds in both countries, as expected, but higher than the third round in Scotland. The use of FIT as a follow-up to a weak positive gFOBT has advantages over a repeat gFOBT. The important published clinical outcomes, namely, cancer detection rate and PPV for cancer and for cancer and all adenoma were superior to those found in the mainly incident second and third screening rounds in both Scotland and England, and these findings confirm that the choice of the two-tier reflex algorithm leads to the detection of more significant neoplasia. Providing a FIT to those who submit an untestable gFOBT does not confer advantages, at least as far as outcomes are concerned, and should be reviewed.
DECLARATION OF INTERESTS
Professor CG Fraser, through NHS Tayside, held a consultancy contract with Immunostics Inc during part of the period of this study: this did not influence the study. All other authors: none to declare.